a Epidemiology and Laboratory Capacity Programme, Public Health and Hospital Emergency Preparedness Office, Commonwealth Health Care Corporation, Saipan, Commonwealth of the Northern Mariana Islands.
b Research Evidence and Information Programme, Public Health Division, Pacific Community.
c Notifiable Disease and Surveillance and International Health Regulations Division, Ministry of Health, Samoa.
d National Laboratory, Tupua Tamasesse Meaole Hospital, Samoa National Health Services.
e Johns Hopkins University Applied Physic Laboratory.
Correspondence to Paul White (email:paul.white@dph.gov.mp).
To cite this article:
White P, Saketa S, Durand A, Vaai-Nielsen S, Leong-Lui TA, Naseri T, et al. Enhanced surveillance for the Third United Nations Conference on Small Island Developing States, Apia, Samoa, September 2014. Western Pac Surveill Response J. 2017 Feb;8(1). doi:10.5365/wpsar.2016.7.4.002.
The Ministry of Health in Samoa, in partnership with the Pacific Community, successfully implemented enhanced surveillance for the high-profile Third United Nations Conference on Small Island Developing States held concurrently with the popular local Teuila festival during a widespread chikungunya outbreak in September 2014.
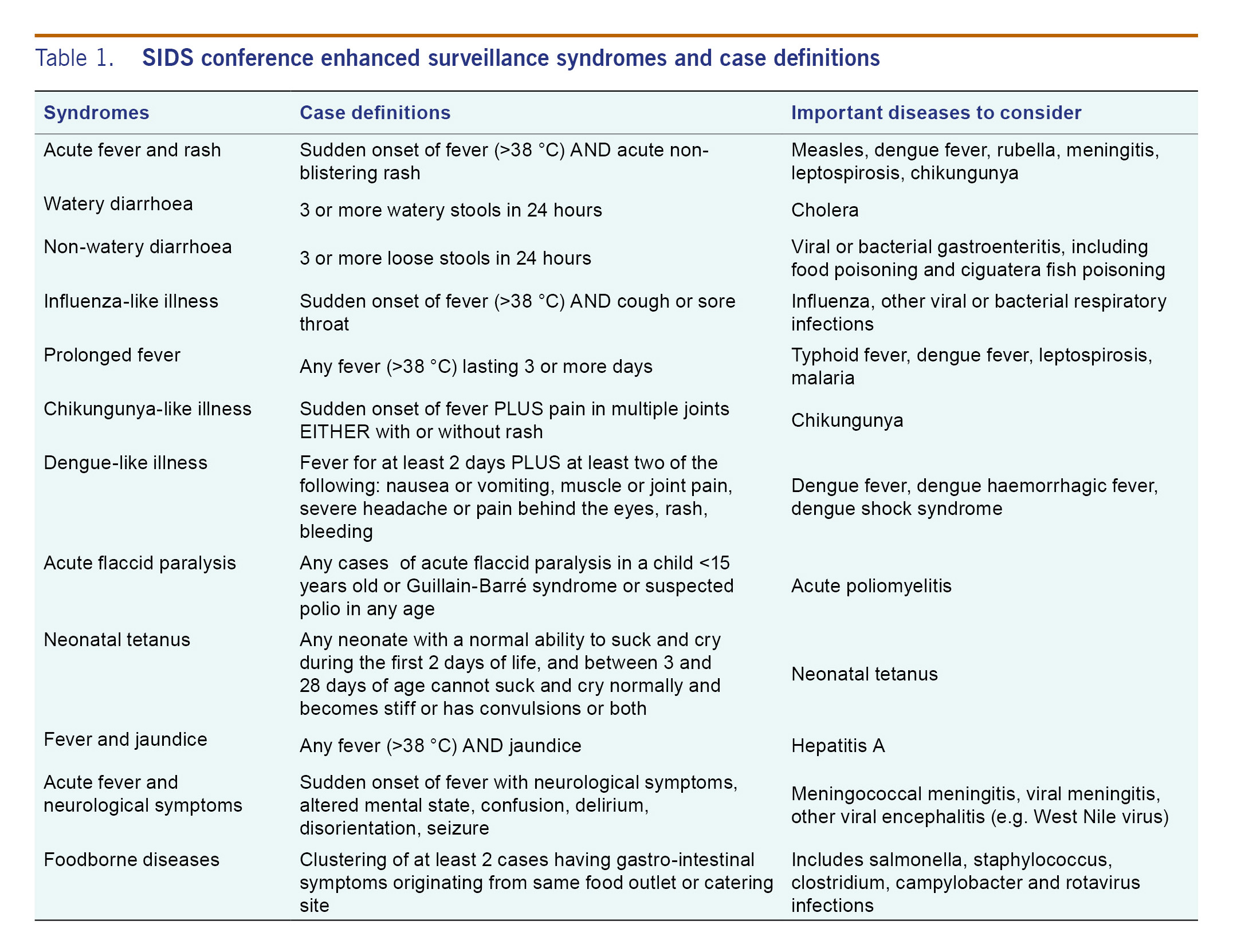
Samoa's weekly syndromic surveillance system was expanded to 12 syndromes and 10 sentinel sites from four syndromes and seven sentinel sites; sites included the national hospital, four private health clinics and three national health service clinics. Daily situation reports were produced and were disseminated through PacNet (the email alert and communication tool of the Pacific Public Health Surveillance Network) together with daily prioritized line lists of syndrome activity to facilitate rapid response and investigation by the Samoan EpiNet team. Standard operating procedures for surveillance and response were introduced, together with a sustainability plan, including a monitoring and evaluation framework, to facilitate the transition of the mass gathering surveillance improvements to routine surveillance.
The enhanced surveillance performed well, providing vital disease early warning and health security assurance. A total of 2386 encounters and 708 syndrome cases were reported. Influenza-like illness was the most frequently seen syndrome (17%). No new infectious disease outbreaks were recorded. The experience emphasized: (1) the need for a long lead time to pilot the surveillance enhancements and to maximize their sustainability; (2) the importance of good communication between key stakeholders; and (3) having sufficient staff dedicated to both surveillance and response.
The Third United Nations Conference on Small Island Developing States (SIDS) was held in Apia, Samoa, from 1 to 4 September 2014. Attracting over 3000 delegates from more than 100 countries and territories,1 this was the largest international event ever hosted by Samoa - a Pacific island nation of 187 820 people.2 The SIDS conference occurred simultaneously with the annual Teuila festival, one of the Pacific region's largest cultural events.
Large gatherings present considerable public health disease risks,3,4 particularly where there is a large and diverse international population influx. This was demonstrated in Samoa, as the two events coincided with outbreaks of chikungunya (CHIKV) locally5 and with the largest ever Ebola virus disease (EVD) outbreak in West Africa. While the EVD importation risk to Pacific island countries and areas was low,6 the stress on the Samoan health system to accommodate EVD cases in the event of any incidences would have been very high. The evolving CHIKV outbreak and ongoing dengue fever, measles and conjunctivitis outbreaks in neighbouring Pacific island countries and areas5 could have overwhelmed local health resources and disrupted the SIDS conference.
As part of meeting health security preparations for the SIDS conference, including International Health Regulations (2005) requirements for improving surveillance, the Samoan Ministry of Health (MoH) asked the Pacific Community (SPC) for technical support in planning, implementing and managing enhanced surveillance for the event. Enhanced surveillance is a practical response to elevated public health risks arising from "events attended by a sufficient number of people to strain the planning and response resources of a community state or nation".7 As a foundation of disease prevention and control,8 surveillance provides early warning of potential disease outbreaks, allowing timely response and prioritized management of surge demands on health services. Mass gathering surveillance is commonly implemented in many countries for a range of sporting,4,5 religious and cultural festivals,3,9 and international political meetings,10 ranging in size from a few thousand people (8th Micronesian Games) to millions (Hajj pilgrimages).
SPC has accumulated considerable Pacific experience in implementing enhanced surveillance during mass gatherings, including the 2012 11th Festival of Pacific Arts, Solomon Islands; the 2013 Pacific Mini-games, Wallis and Futuna; and the 2014 8th Micronesian Games, Pohnpei State, Federated States of Micronesia. Here we describe the SIDS conference surveillance implemented by the Samoa MoH and SPC, highlighting lessons that may be helpful to public health planners in preparation for disease surveillance for mass gatherings.
There were three primary purposes for the enhanced surveillance: (1) to provide a simple surveillance system for rapidly detecting and responding to disease episodes or outbreaks in a timely and effective manner; (2) to disseminate strategic epidemiological information throughout the Pacific region; and (3) to sustainably improve disease surveillance in Samoa beyond the mass gathering event.
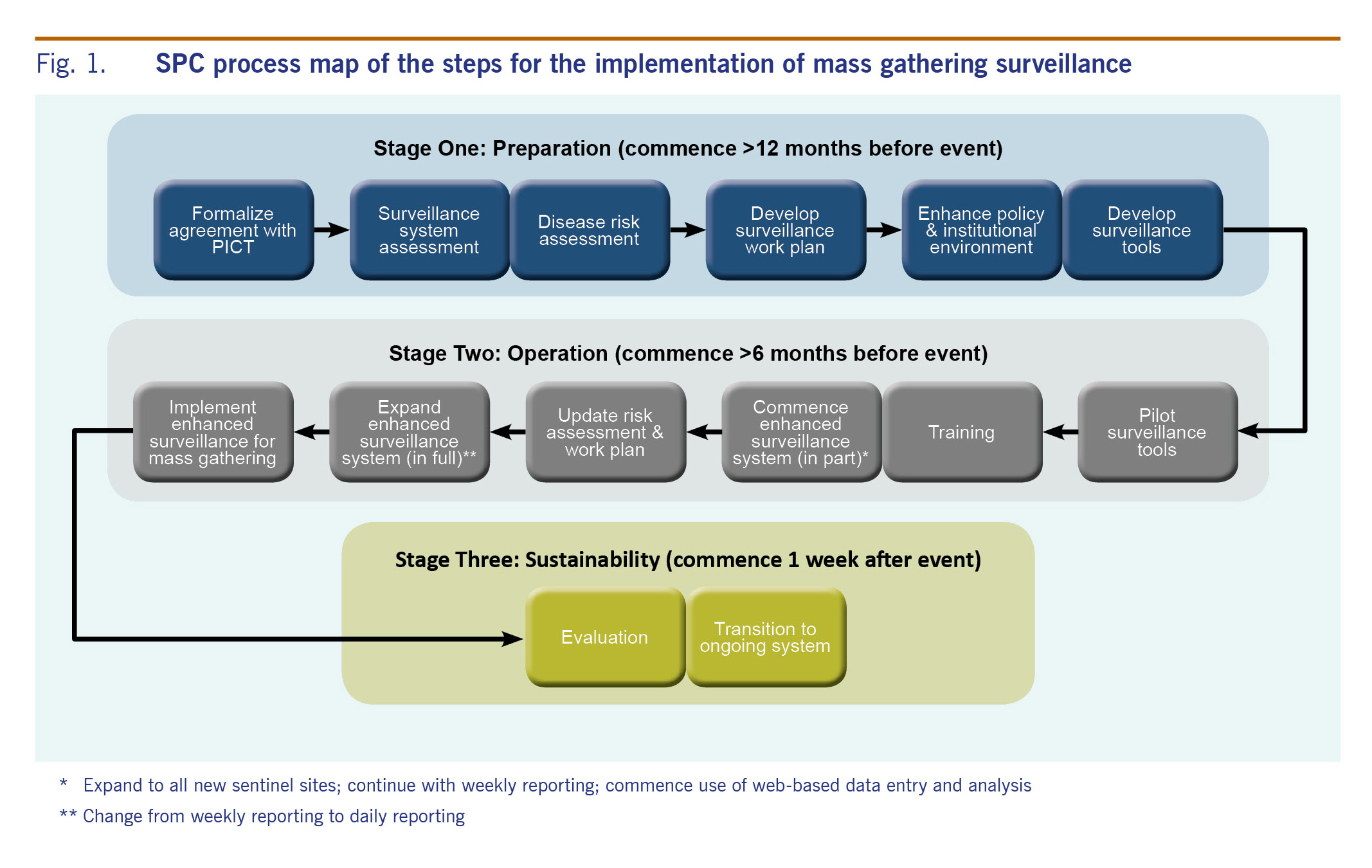
SPC employs a three-stage process for enhanced surveillance (see Fig. 1) comprising preparation, operation and sustainability functions. Preparation should commence 12 months before the event and includes assessing the surveillance system and disease risk and developing a work plan for enhanced surveillance. Surveillance operations of the second phase commences up to six months ahead of the event and includes pilot testing, training and implementing the enhanced surveillance system. The sustainability phase starts one week after the event and involves transition to the regular surveillance system and evaluation of the impact of the enhanced surveillance.
The surveillance needs for the SIDS conference were determined by assessing: (1) the current scope and scale of the existing surveillance system; (2) the number and geographical diversity of SIDS conference delegates; and (3) the disease risks.
Four themes emerged from the health risk assessment: the current CHIKV outbreak, outbreaks of other infectious diseases in Pacific island countries and areas (dengue, measles), fear of EVD importation and the increased pressure on existing health services if an outbreak occurred. Based on the assessment and building on the existing syndromic surveillance system, the following modifications were made for the mass gathering surveillance:11
A two-day training course was held for the sentinel site focal points with refresher training occurring during daily data collection rounds. Training focused on:
The surveillance was tested in the week preceding the SIDS conference and became operational on 26 August. The enhanced surveillance continued until 19 September, and the daily reporting ended on 6 September.
A surveillance register system captured daily acute care encounters and syndrome cases. The surveillance registers were collected at each sentinel site each day and exchanged for new registers.
SAGES OE is a freeware tool designed by Johns Hopkins University Applied Physics Laboratory (JHU-APL).12 SAGES OE was adapted for the enhanced surveillance by JHU-APL and SPC and had successfully been used previously by SPC for mass gathering surveillance;13 however, technical challenges in locally hosting the system precluded the full use of SAGES OE at the SIDS conference, so a spreadsheet-based alternative was used to store the daily data and generate graphical output. This output was incorporated into daily situation reports (SitReps), providing descriptive summaries (including laboratory results) and narrative interpretation of daily syndrome and encounter activity.
A laboratory surveillance focal point was selected to link syndromic surveillance and laboratory surveillance at the national laboratory in the Tupua Tamasese Meaole Hospital (TTMH). The diagnostic process included off-island sample referral protocols for confirmatory testing for epidemic-potential diseases.
The surveillance team provided early warning alerts for immediate response follow-up of any prioritized syndrome cases (such as acute fever and rash or bloody diarrhoea) that were found at the time of daily data collection. Additionally, daily case reports were given to the response team for follow-up investigation. SitReps were emailed to the MoH and the SIDS organizing stakeholders and were disseminated to regional public health professionals via the PacNet Pacific regional public health email network.
A sustainability plan was generated to transition improvements from the mass gathering surveillance to the routine surveillance system to harness the considerable effort involved in implementing the enhanced surveillance. This included a monitoring and evaluation plan to benchmark surveillance performance for future assessment. The sustainability plan was discussed during a joint SPC and MoH debriefing session at the end of the mass gathering.
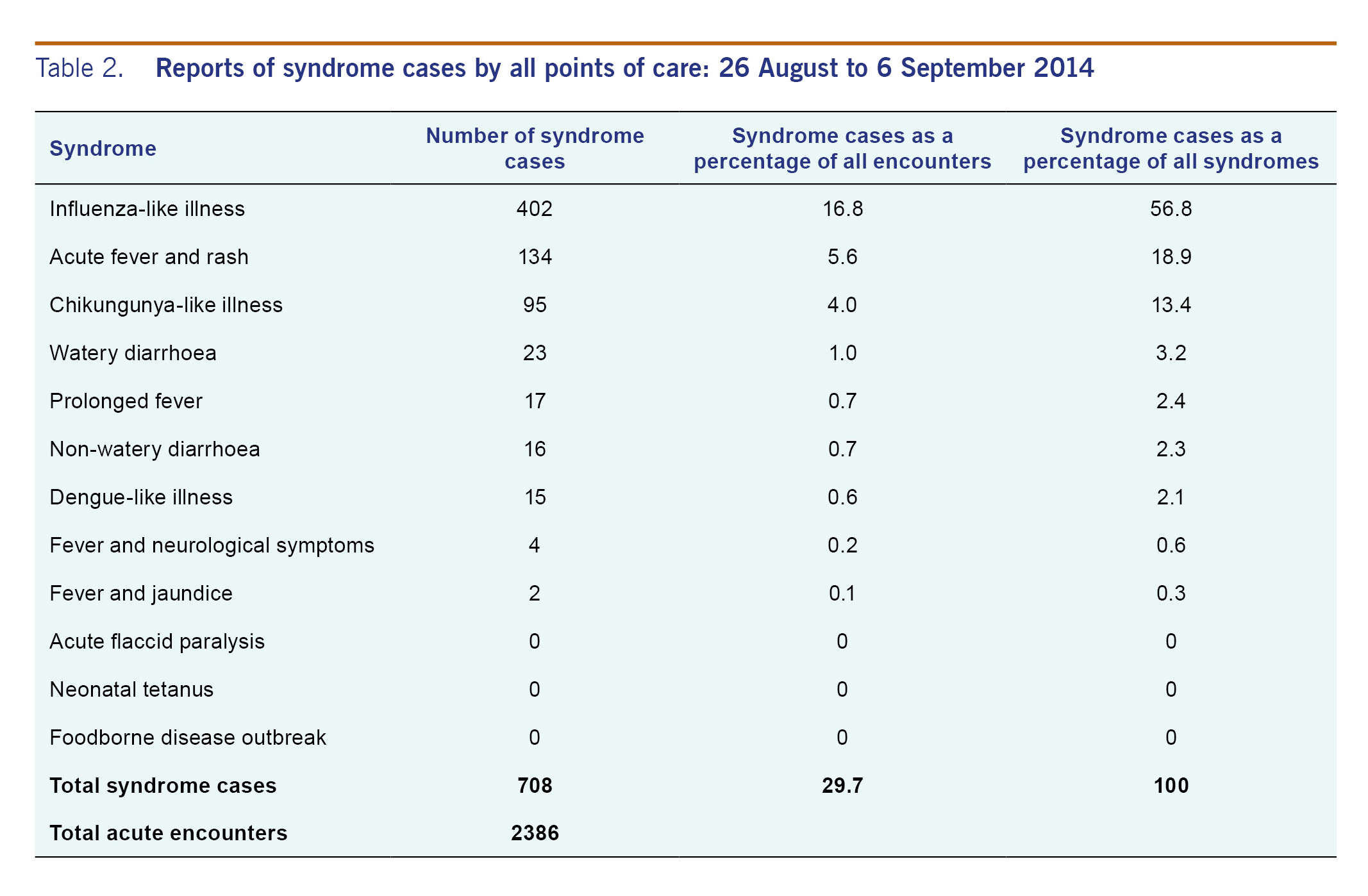
A total of 2386 encounters were seen at the 10 sentinel sites, from 26 August to 6 September 2014. Daily encounters at the sentinel sites ranged from 0 to 299. Seven hundred eight encounters (30%) presented with syndromes under surveillance (see Table 2). Three syndromes accounted for nearly 90% of all syndrome cases (n = 631) and more than a quarter of all encounters (26.4%): influenza-like illness - nearly 60% of syndrome cases (n = 402), acute fever and rash - 19% (n = 134) and chikungunya-like illness - 13% (n = 95). No acute flaccid paralysis, neonatal tetanus or foodborne diseases were reported. One case of dengue-like illness was investigated and tested positive by rapid test (NS1, Bio-Rad Laboratories, Marnes-la-Coquette, France), with evidence of acute (probable primary) dengue fever infection.13 Most syndrome cases were reported among Samoan nationals, and no importation of any infectious diseases among delegates and visitors were reported.
No new infectious disease outbreaks were recorded for the SIDS conference, and the surveillance system performed well, providing important assurances for public health safety. The CHIKV outbreak was well managed and did not impact the conference. Increasing reporting frequency from weekly to daily, increasing the number of syndromes and the number of sentinel sites improved public awareness of the health risks to the local and international community. These measures together with sentinel clinicians' awareness and accurate identification of syndrome definitions improved surveillance sensitivity. This is shown with 30% of encounters as syndrome cases, compared to only 7%-10% of encounters recorded as syndrome cases in previous SPC-implemented mass gathering surveillance activities in the Pacific. (White P, Mercier A, Saketa S, Hoy D. Sustaining Enhanced Syndromic Surveillance in Pohnpei (FSM). Noumea: The Pacific Community (SPC), unpublished report. 2014), (Dr Sala Saketa, The Pacific Community (SPC), personal communication, 12 January 2014)
The benefits of enhanced surveillance can be sustained when the mass gathering surveillance experience is integrated into long-term surveillance improvement plans rather than being treated as an isolated activity occurring only during a discrete time frame. Similarly, it is more likely that the extra effort involved in mass gathering enhanced surveillance will be implemented when the work involved is similar to the usual surveillance. The SIDS conference enhanced surveillance was implemented by building on the existing weekly surveillance, facilitating straightforward transition after the conference as well as enabling lessons learnt and benefits gained to be readily applied.
Lessons learnt from the SIDS conference enhanced surveillance experience identified important points for the future planning of mass gathering surveillance:
The enhanced surveillance for the SIDS conference was a large surveillance operation that provided important public health security assurance in support of a high-profile United Nations meeting simultaneously with an equally large local festival that both occurred concurrently with a widespread CHIKV outbreak. Sustainable benefits of the enhanced surveillance included fostering a closer working relationship between public health authorities, the TTMH laboratory and clinical services and improving surveillance activities.
Mass gathering surveillance typically involves a short period of intense activity that can be an extra burden on over-stretched public health resources. However, impacts on resources and staff can be minimized by building on and enhancing existing surveillance activities. This allows for the efficient commencement of enhanced surveillance and transition back to routine surveillance. This approach can result in improvements to public health systems in both capacity (training of staff) and capability (efficiency and quality improvements in the functioning of the surveillance system) that remain long after the mass gathering is over. The benefits from these improvements include better health security arising from the ongoing surveillance operations and indirect benefits from improvements to the epidemiological evidence base available to health planners that accrue through having better-trained surveillance staff, providing better-informed information, from improved data collection and surveillance coverage. Accordingly, mass gathering surveillance can stimulate improvements in public health surveillance that may not have otherwise occurred. The diligent work of the Samoan public health communicable disease surveillance team during the SIDS conference, and the experience they gained in enhanced surveillance, was applied during the mass gathering surveillance for 2015 Commonwealth Youth Games, which was also held in Apia, Samoa.
None.
We wish to thank all of the Samoa Ministry of Health staff who assisted with data entry for the enhanced surveillance and all of the Samoa National Health Services hospital and community health-care providers who were at the sentinel surveillance sites.