a National Tuberculosis Control Programme Viet Nam, Hanoi, Viet Nam.
b Centre for Operational Research, International Union Against Tuberculosis and Lung Disease, Paris, France.
c Viet Nam Association for Tuberculosis and Lung Disease, Hanoi, Viet Nam.
d Ministry of Health, Department of International Cooperation, Viet Nam.
e Hanoi Medical University, Hanoi, Viet Nam.
f Hanoi School of Public Health, Hanoi, Viet Nam.
Correspondence to Nguyen Binh Hoa (email: nguyenbinhhoatb@yahoo.com).
To cite this article:
Hoa NB et al. Prevalence of resistance to second-line tuberculosis drug among multidrug-resistant tuberculosis patients in Viet Nam, 2011. Western Pacific Surveillance and Response Journal, 2016, 7(2):35–40. doi:10.5365/wpsar.2016.7.2.002
Introduction: Extensively drug-resistant tuberculosis (XDR-TB) represents an emerging public health problem worldwide. According to the World Health Organization, an estimated 9.7% of multidrug-resistant TB (MDR-TB) cases are defined as XDR-TB globally. The objective of this study was to determine the prevalence of drug resistance to second-line TB drugs among MDR-TB cases detected in the Fourth National Anti-Tuberculosis Drug Resistance Survey in Viet Nam.
Methods: Eighty clusters of TB cases were selected using a probability-proportion-to-size approach. To identify MDR-TB cases, drug susceptibility testing (DST) was performed for the four major first-line TB drugs. DST of second-line drugs (ofloxacin, amikacin, kanamycin, capreomycin) was performed on isolates from MDR-TB cases to identify pre-XDR and XDR cases.
Results: A total of 1629 smear-positive TB cases were eligible for culture and DST. Of those, DST results for first-line drugs were available for 1312 cases, and 91 (6.9%) had MDR-TB. Second-line DST results were available for 84 of these cases. Of those, 15 cases (17.9%) had ofloxacin resistance and 6.0% were resistant to kanamycin and capreomycin. Five MDR-TB cases (6.0%) met the criteria of XDR-TB.
Conclusion: This survey provides the first estimates of the proportion of XDR-TB among MDR-TB cases in Viet Nam and provides important information for local policies regarding second-line DST. Local policies and programmes that are geared towards TB prevention, early diagnosis and treatment with effective regimens are of high importance.
Tuberculosis (TB) is a leading cause of death in communicable diseases. According to the World Health Organization (WHO), an estimated 9.6 million people developed TB and 1.5 million died from the disease worldwide in 2014.1 Viet Nam ranks 12th among the 22 high-burden TB countries.1 In 2007, the first nationwide TB prevalence survey in Viet Nam showed a prevalence of bacteriological-positive TB of 307 per 100 000 adult population (15 years or older) and a prevalence of smear-positive TB of 197 per 100 000 adult population.2
Resistance to anti-TB drugs is a public health threat to controlling TB worldwide.1,3,4 Globally, the proportion of cases with multidrug-resistant TB (MDR-TB)4 is 3.3% among new TB cases and 20% among previously treated TB cases, accounting for about 480 000 people in 2014.1 Viet Nam is among the 27 high MDR-TB burden countries; the estimated proportion of new MDR-TB cases in Viet Nam was 4.0%, and the estimated proportion of MDR-TB among re-treatment cases was 23% in 2014.1,5 Based on the Fourth National Anti-Tuberculosis Drug Resistance Survey in Viet Nam and the WHO Global Tuberculosis Report 2015, there were an estimated 5100 cases with MDR-TB among notified TB cases in Viet Nam.1,5
In 2009, the Viet Nam National Tuberculosis Programme (NTP) implemented programmatic management of drug-resistant TB (PMDT) to diagnose and provide treatment with second-line TB drugs (SLDs) for MDR-TB under programme condition. The PMDT has been integrated into the general national TB control programme with additional financial and technical support to manage MDR-TB cases. The number of MDR-TB cases detected and enrolled for MDR treatment increased from 101 in 2009 to 2131 in 2015. These cases account for 42% of the estimated 5100 MDR-TB cases in Viet Nam, which is much higher than the proportion (26%) in the global estimation.1 However, this achievement still needs to be improved to achieve the national target of MDR-TB case enrolment for treatment.
Extensively drug-resistant TB (XDR-TB) represents an emerging public health problem worldwide.1,3 According to WHO, an estimated 9.7% of global MDR-TB cases had XDR-TB.1 The emergence and spread of MDR and XDR-TB is a big challenge for TB control activities as treatment of MDR and XDR-TB cases is more expensive, has more adverse drug reactions, is less successful and has higher death rates than other types of TB.1,3,4,6
In 2011, the Viet Nam NTP conducted the Fourth National Anti-Tuberculosis Drug Resistance Survey in Viet Nam to assess the burden of TB drugs resistance in the country.5 In this study, we performed drug susceptibility testing (DST) for first-line TB drugs to estimate the prevalence of MDR-TB; we also conducted DST for SLDs (ofloxacin, amikacin, kanamycin and capreomycin). We aimed to determine the prevalence of XDR-TB among all MDR-TB cases detected in the Fourth National Anti-tuberculosis Drug Resistance Survey in Viet Nam.
The full details of the study design, sampling strategy, sample size calculation and analysis of the Fourth National Anti-Tuberculosis Drug Resistance Survey in Viet Nam are described elsewhere.5 Briefly, it was a cross-sectional survey that used a probability-proportional-to-size (PPS) sampling approach based on notifications of new smear-positive TB cases to assess the prevalence of MDR-TB among TB cases in Viet Nam. This survey was conducted in 80 clusters chosen from all district TB units in the country where TB cases were diagnosed and registered for treatment. Eligible cases were smear-positive TB cases newly registered for treatment (both new and previously treated TB cases) in the selected clusters during the period of recruitment. The required sample size was 1612 new smear-positive TB cases; therefore, each cluster was required to enrol at least 22 new TB cases during the six month period from June to December 2011. All previously treated smear-positive TB cases identified during this period were enrolled in this study.
Data collection and laboratory procedures have also been described in detail elsewhere.5 Briefly, TB cases were interviewed face-to-face to collect information on age, sex, region of residence, previous TB treatment history, symptoms and HIV status. Two sputum samples were collected from each patient for culture and DST. The samples were transported, within 48 hours after collection, in chilled containers (2–8 °C) to two national/regional laboratories and five provincial laboratories that have the capacity and facilities for TB culture. The specimens were decontaminated using 4% NaOH, and 0.1 mL of the mixture was inoculated onto two Ogawa tubes (according to the modified Petroff’s method).7 The isolates were then sent to two national laboratories for identification and DST, using the proportion method on Loewenstern-Jensen medium for four drugs: Isoniazid (INH), Rifampicin (RMP), Ethambutol (EMB) and Streptomycin (SM) with the following critical concentrations: INH 0.2 µg/ml, RMP 40 µg/ml, EMB 2 µg/ml and SM 4 µg/ml. The proportion method on Loewenstern-Jensen medium was also conducted for DST for all SLDs including ofloxacin (OFX), amikacin (AM), kanamycin (KM) and capreomycin (CM) with the following critical concentrations: OFX 2 µg/ml, KM 30 µg/ml, AM 40 µg/ml, CM 40 µg/ml, according to WHO standard.8
To ensure the quality of the DST, all samples of MDR-TB cases’ isolates in the two national hospitals were sent for re-testing by crosscheck between two national and regional laboratories following WHO guidelines for surveillance of drug resistance in TB.9 Quality assurance for the culture and DST in this study was provided by a reference laboratory in Adelaide, Australia.
We followed WHO-recommended definitions for TB drugs resistance cases:4
All data were extracted from the survey database and laboratory database of the Fourth National Anti-Tuberculosis Drug Resistance Survey in Viet Nam. Data analysis was performed using Stata version 12 SE software (Stata Corporation, College Station, Texas, USA). We calculated the numbers and proportions of MDR-TB cases who had resistance to SLDs (based on the four SLDs as described previously). The 95% confidence intervals (CI) were calculated throughout and the level of significance was set at P ≤ 0.05.
The study protocol was approved by the Ethical Institutional Review Board of the National Lung Hospital, Viet Nam.
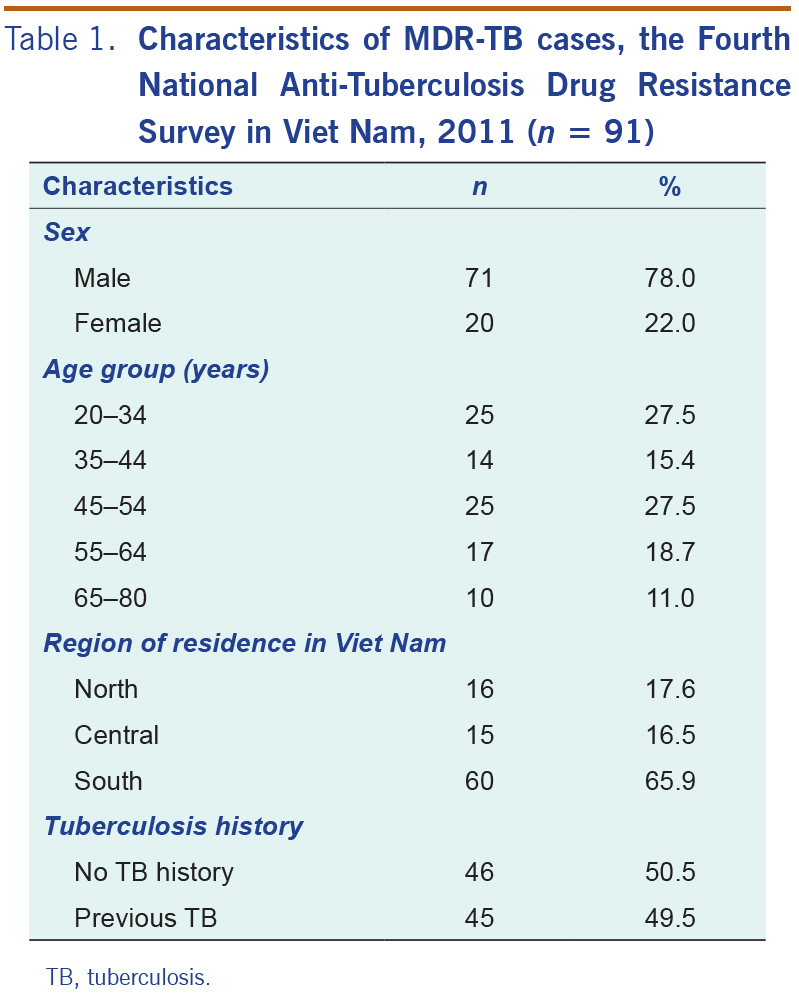
The survey was conducted in 80 TB clusters from 1 June to 31 December 2011 and enrolled 1840 smear-positive TB cases. Nine clusters were excluded due to a laboratory contamination problem identified after the end of the case enrolment period in one of the seven culture laboratories. In total, 1552 samples that had been cultured were included in the analysis. Of those, the total number of people diagnosed with smear- and culture-positive TB was 1341; DST results were available for 1312 cases. Of those, 91 MDR-TB cases were reported, including 46 MDR-TB among 1105 new TB cases (4.2%, 95% CI: 2.5–5.4) and 45 MDR-TB among 195 previously treated TB cases (23.1%; 95% CI: 16.7–29.9). Table 1 shows the demographic characteristics of the 91 MDR-TB cases. The median age of these cases was 46.2 years (range 20–80 years); 27.5% were in the 20–34 year age group. Of the 91 MDR-TB cases, 78.0% were male and 65.9% were residents of the southern region in Viet Nam.
TB, tuberculosis.
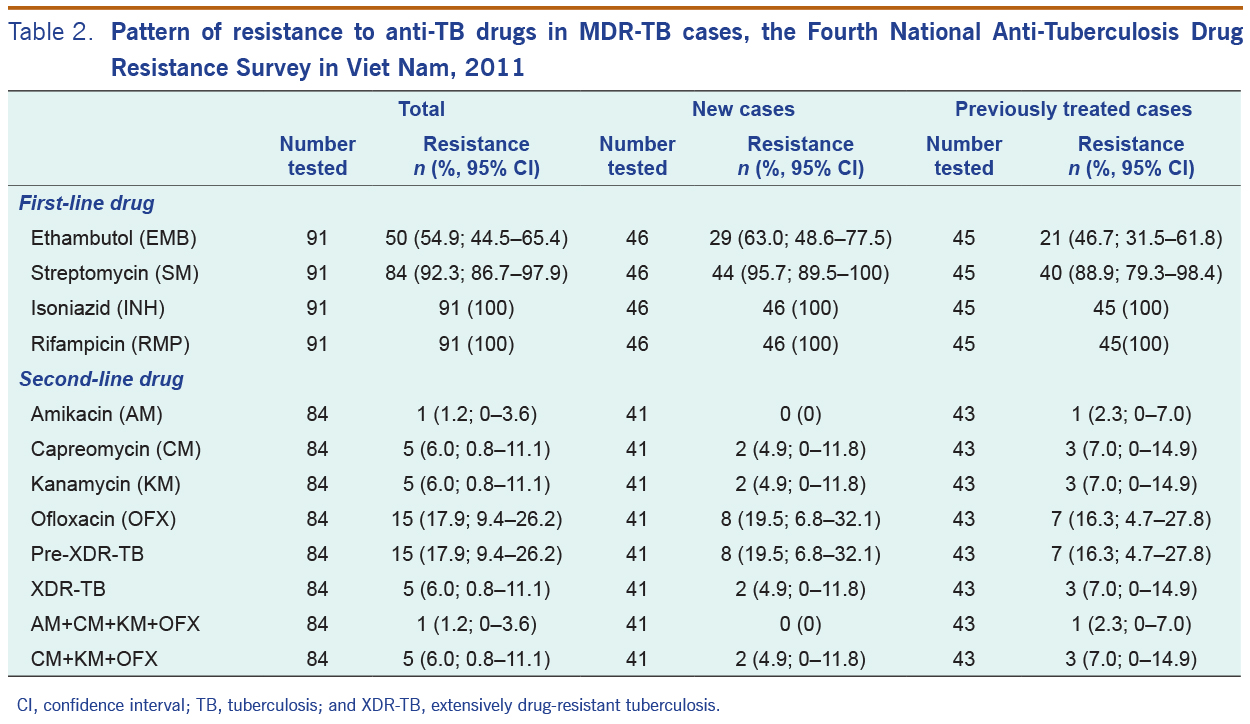
By definition, all of the 91 MDR-TB cases were resistant to INH and RMP (Table 2). In addition, 50 MDR-TB cases (54.9%; 95% CI: 44.5–65.4) were resistant to EMB, 84 (92.3%; 95% CI: 86.7–97.9) were resistant to SM and 47 (51.6%; 95% CI: 41.2–62.1) were resistant to both EMB and SM. Of the 46 new MDR-TB cases, 29 (63.0%; 95% CI: 48.6–77.5) were resistant to EMB, 44 (95.7%; 95% CI: 89.5–100.0) were resistant to SM and 27 (58.7%; 95% CI: 43.9–73.5) were resistant to both EMB and SM. Of 45 re-treated cases, 21 (46.7%; 95% CI: 31.5–61.8) were resistant to EMB, 40 (88.9%; 95% CI: 79.3–98.4) were resistant to SM and 20 (44.4%; 95% CI: 29.3–59.5) were resistant to both EMB and SM.
Of the 91 MDR-TB cases, second-line DST results were available for 84 (92.3%) of them (Table 2). The overall proportion of pre-XDR was 17.9% (95% CI: 9.4–26.2). The proportion of pre-XDR in new cases (n = 41) was 19.5% (95% CI: 6.8–32.1) and 16.3% (95% CI: 4.7–27.8) in previously treated cases (n = 43). A further five cases, 6.0% (95% CI: 0.8–11.1) were classified as XDR-TB, including two new (4.9%, 95% CI: 0–11.8) and three previously treated cases (7.0%, 95% CI: 0–14.9).
CI, confidence interval; TB, tuberculosis; and XDR-TB, extensively drug-resistant tuberculosis.
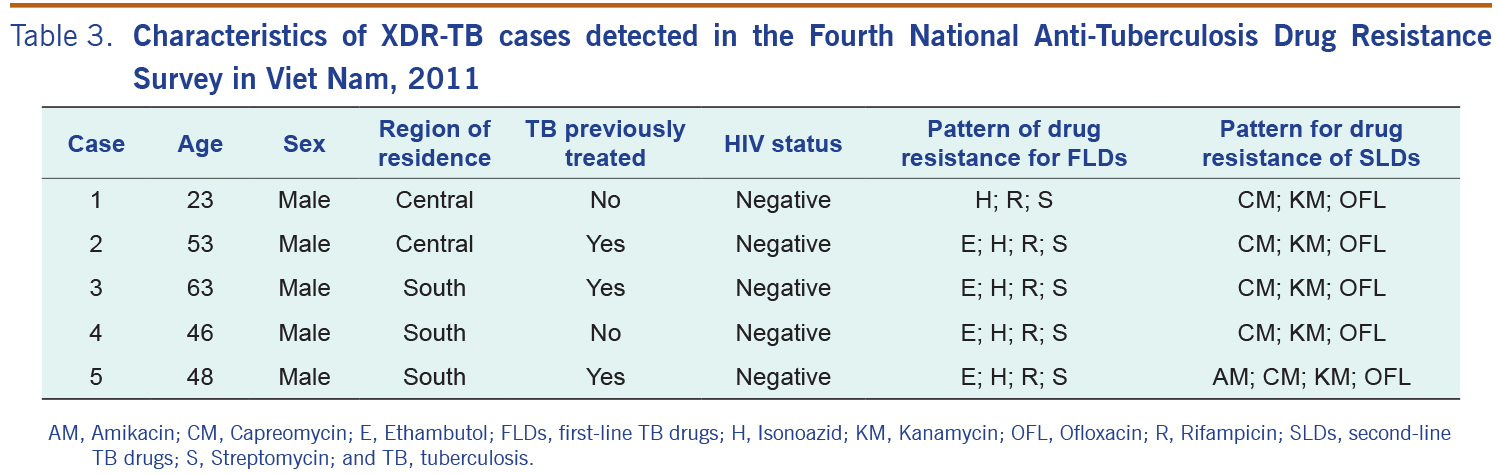
Table 3 presents the characteristics of the five XDR-TB cases. All of them were male and were HIV sero-negative. The median age of XDR-TB cases was 48 years with the youngest aged 23 years and the oldest 63 years old. The XDR-MTB isolates originated from the central (n = 2) and southern (n = 3) regions of Viet Nam.
AM, Amikacin; CM, Capreomycin; E, Ethambutol; FLDs, first-line TB drugs; H, Isonoazid; KM, Kanamycin; OFL, Ofloxacin; R, Rifampicin; SLDs, second-line TB drugs; S, Streptomycin; and TB, tuberculosis.
We observed high levels of resistance to SLDs among MDR-TB cases. Our findings support data presented by other studies.4,6,10–14 The overall proportion of XDR-TB among MDR-TB cases in this study was still lower than the global average estimate.1 Whereas the proportion of XDR-TB among MDR-TB cases elsewhere varied from 5% to 21%.4,6,10–14 However, James et al. reported a very high percentage of XDR-TB among MDR-TB cases (60%) in India.15 This could be due to referral bias because that study was conducted among the cases referred to the tertiary care hospital.
We believe the main reason for XDR-TB is indiscriminate use of antibiotics that are also used as second-line anti-TB drugs. (FQs and others second-line drugs were available in pharmacies in high TB burden countries.)16 It is also due to inadequate treatment by health staff and low compliance to full therapy by TB cases. In Viet Nam, of 1380 MDR-TB cases enrolled for treatment during 2010–2012, 372 (27%) were unable to complete treatment. (This proportion varied in different parts of Viet Nam.) Loss-to-follow-up was the main unfavourable treatment outcome (13%) and may be due to the long treatment period.17
MDR-TB and XDR-TB are indicators of TB control failures; they emerge due to several reasons: (1) provider may prescribe insufficient drug regiments for TB cases; (2) TB cases may not adhere to an appropriate regimen; (3) drugs may be of poor quality; and (4) there is transmission of MDR-TB and XDR-TB in the community. In Viet Nam, anti-TB drugs (both first-line and second-line drugs) are available without a medical prescription. About half of the private pharmacies were willing to dispense drugs either to TB cases or to those who asked for TB medication.18 We found a high prevalence of resistance to OFX (9.4–26.2%), similar to other studies.10,13,14,19,20 This may be due to the fact that TB cases who received treatment may have used OFX before. The high prevalence of pre-XDR TB cases might imply the inappropriate usage of drugs, especially FQs including OFX. This drug is the most commonly prescribed antibiotic for respiratory tract infections as well as other bacterial infections, and in some cases it is available in local drug stores in Viet Nam without presenting a prescription.16 Easy access and inappropriate use of these drugs increase the risk for drug-resistant TB emergence.
In this study, all TB cases who were resistant to KM were also resistant to CM, consistent with other studies.21,22 CM is not widely available as it is expensive, and is not commonly used in Viet Nam. Maus et al. reported the cross-resistance between KM and CM in a study in the United States of America.21 The study describes isolates resistant to CM and LM caused by mutations in the rrs gene. The isolates recovered from TB cases treated with KM were resistant to KM and CM, and the resistance of the strains to CM varied with the level of KM resistance.21 Further investigation of the rrs gene for MDR-TB cases is needed to confirm the cross-resistance to KM and CM in Viet Nam.
There are limitations in this study. First, the clusters were selected based on the notification of new smear-positive TB cases in 2003 but not on more recent data. However, case distribution for TB notifications remained fairly stable from 2003 to 2011.5 Second, this study did not include the private health sector, therefore we could not estimate the burden of MDR-TB in the private sector. Nevertheless, in spite of these shortcomings, samples in this study generally represent all of Viet Nam.
This survey provides the first estimates of the proportion of XDR-TB among MDR-TB cases in Viet Nam. The results provide important information for clinicians and local policy-makers as well as international health agencies regarding the conduct of second-line DST. Local TB policies and programmes that are geared towards prevention, early diagnosis and treatment with effective regimens are of high importance.
None declared.
None.
The authors thank the National Tuberculosis Programme Board; all national, regional, provincial, district and commune-level staff involved in the survey; and all patients taking part in the study. We sincerely thank Dr Edine W Tiemersma, from the KNCV Tuberculosis Foundation, The Hague, the Netherlands for her support in data management and validations as well as Richard Lumb from the Mycobacterium Reference Laboratory, Adelaide, Australia for his support in quality assurance for the culture and DST in this survey.
{kind=link}
{kind=link}
{kind=link}