a Field Epidemiology Training Program Alumni Foundation Incorporated, Department of Health Compound, Sta Cruz, Manila, Philippines.
b Office of the WHO Representative in the Philippines, Sta Cruz, Manila, Philippines.
Correspondence to Sheila Tante (email: epidoc_sheila@yahoo.com).
To cite this article:
Tante S et al. Which surveillance systems were operational after Typhoon Haiyan? Western Pacific Surveillance and Response Journal, 2015, 6(Suppl 1):66–70. doi:10.5365/wpsar.2015.6.2.HYN_015
Introduction: Effective disease surveillance is vital for a successful disaster response. This study assessed the functionality of the three disease surveillance systems used post-Haiyan: Philippine Integrated Disease Surveillance and Response (PIDSR), Event-based Surveillance and Response (ESR) and Surveillance in Post Extreme Emergencies and Disasters (SPEED).
Methods: A survey of 45 government health officers from affected areas was conducted in March 2014. The survey documented when each of the systems was operational and included questions that ranked the functionality of the three surveillance systems and whether they complemented each other.
Results: Two of 11 (18%) surveillance units had an operational SPEED system pre-event. PIDSR and ESR remained operational in five of 11 (45%) surveillance units without interruption of reporting. Ten surveillance units (91%) rated PIDSR as functional post-Typhoon; eight (72.7%) considered ESR functional. SPEED was rated as functional by three (27%) surveillance units. Seven of 11 (63.6%) surveillance units rated the three systems as being complementary to each other.
Discussion: In most of the areas affected by Typhoon Haiyan, the routine surveillance systems (PIDSR and ESR) were not disrupted; although, in Leyte it took seven weeks for these to be operational. Although SPEED is recommended for activation within 48 hours after a disaster, this did not occur in most of the surveyed areas. Most of the surveillance units rated PIDSR, ESR and SPEED to be complementary to each other.
Disease surveillance is an integral part of health emergency and disaster management as it allows for the early detection of epidemic-prone diseases for timely and appropriate response, prevention and minimizing morbidity and mortality.1
In the Philippines, the Department of Health (DOH) redesigned the existing disease surveillance mechanisms into the Philippine Integrated Disease Surveillance and Response (PIDSR) system in 2008.2 PIDSR is a casebased surveillance system for the routine reporting of 11 identified diseases on a daily basis (Category 1) with another 14 reported weekly (Category 2).3 The Event-based Surveillance and Response (ESR) system was established in 2010 to complement PIDSR and includes the reporting of events not captured by other systems. ESR can capture rare, unusual or unexpected events with formal reporting through a reporting system, media, health workers or nongovermental organizations (NGOs); or informally through rumours, phone calls or text messages.2
In 2010, the DOH-Health Emergency Management Bureau, with assistance from the World Health Organization (WHO), introduced Surveillance in Post Extreme Emergencies and Disasters (SPEED). This electronic-based surveillance mechanism was specifically designed for use during an emergency or disaster. It captures data on 21 communicable and noncommunicable syndromes with case definitions that are different from the regular surveillance systems.4 Data are collected by SPEED coordinators and surveillance officers from health units and sentinel sites specific to the disaster and are reported daily using a structured reporting mechanism. SPEED was activated in Region 6 in October 2013 when the provinces of Cebu City and Bohol were hit by an earthquake. As SPEED includes syndromes of certain conditions, the reporting should be faster than the routine schemes. Once SPEED has been activated, it continues to operate until conditions return to routine levels.
After Typhoon Haiyan hit the Philippines on 8 November 2013, these three surveillance systems were compromised as several health facilities were destroyed and most key health personnel were victims. This study aimed to determine which of the three disease surveillance systems were operational, as well as their functionality and whether they complemented each other for the six months post-Haiyan.
In March 2014, we conducted a survey of 45 government health officers who represented cities, municipalities and provinces from Regions 6, 7 and 8 – the areas worst hit by Haiyan. DOH regional and central counterparts at the local level also participated in the survey; almost half (49%) were Health Emergency Management Coordinators, SPEED coordinators and PIDSR-ESR surveillance officers. The survey assessed the three disease surveillance systems for the period each was operational, their functionality and whether they complemented each other.
We asked the participants to assess functionality in the context of the following attributes: (a) the simplicity of the system while being able to meet its objectives; (b) its flexibility to accommodate (e.g. new events); (c) the completeness and validity of the data recorded; (d) sensitivity to detect outbreaks and monitor changes; and (e) timeliness between steps in a public health surveillance system.5 For Leyte and Tacloban City, functionality was assessed over two time periods which corresponded to when PIDSR and ESR were not operational (November to December 2013) and when they were operational (January 2014 onwards). Functionality was ranked using a Likert Scale of 1 to 5 where 1–2 was not functional, 3 neutral and 4–5 functional. We also asked the participants to consider whether the three systems complemented each other post-Haiyan. Responses were also measured using a Likert Scale of 1 to 5 where 1–2 was not complementary, 3 neutral and 4–5 complementary.
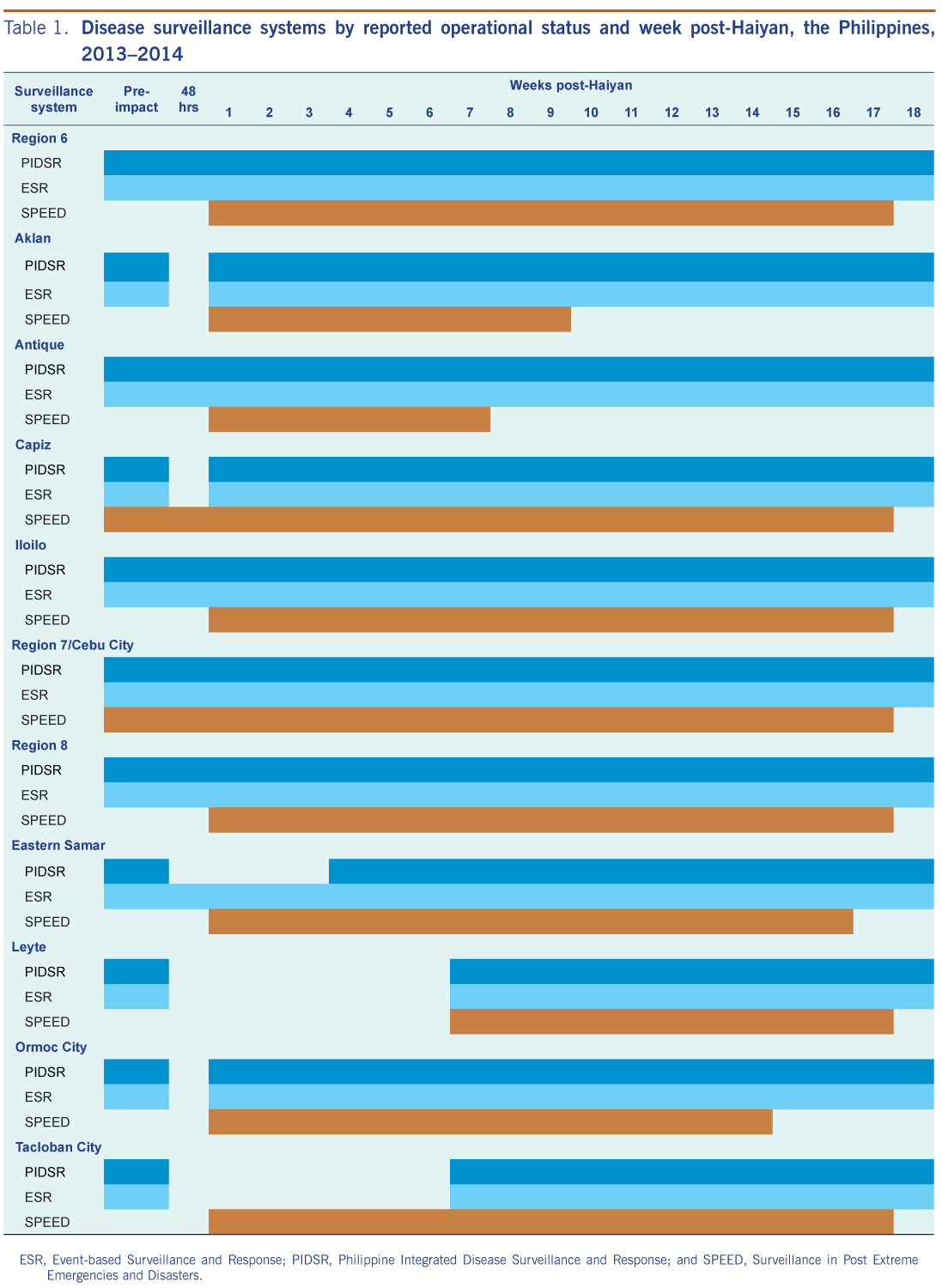
The operation of the three disease surveillance systems varied post-Haiyan by region and province/cities (Table 1). Two of 11 (18%) surveillance units (Region 7 and Capiz) had an operational SPEED system pre-Haiyan. Capiz activated SPEED one day before landfall and Region 7 had SPEED ongoing as a 7.2 magnitude earthquake had struck the province of Bohol three weeks prior. Of the remaining nine surveillance units, eight (89%) had SPEED operational within one week post-Haiyan, and one (11%) was operational within seven weeks (Leyte).
ESR, Event-based Surveillance and Response; PIDSR, Philippine Integrated Disease Surveillance and Response; and SPEED, Surveillance in Post Extreme Emergencies and Disasters.
PIDSR and ESR remained operational in five of 11 (45%) surveillance units without interruption of reporting. One (9%) surveillance unit had no interruption of ESR, but PIDSR was suspended until six weeks post-Haiyan.
The hardest hit areas, Leyte and Tacloban City, had variable interruptions of PIDSR and ESR surveillance activity. In Leyte, limited reporting was back online one week post-Haiyan. In Tacloban City, PIDSR and ESR activities were suspended until seven weeks post-Haiyan. In Tacloban City, SPEED was operational one week post-Haiyan; in Leyte, SPEED was operational seven weeks post-Haiyan.
Deactivation of SPEED occurred 17 weeks post-Haiyan in most (7/11) surveillance units. The number of weeks of activation ranged from 7 to 17 weeks (mean 15 weeks).
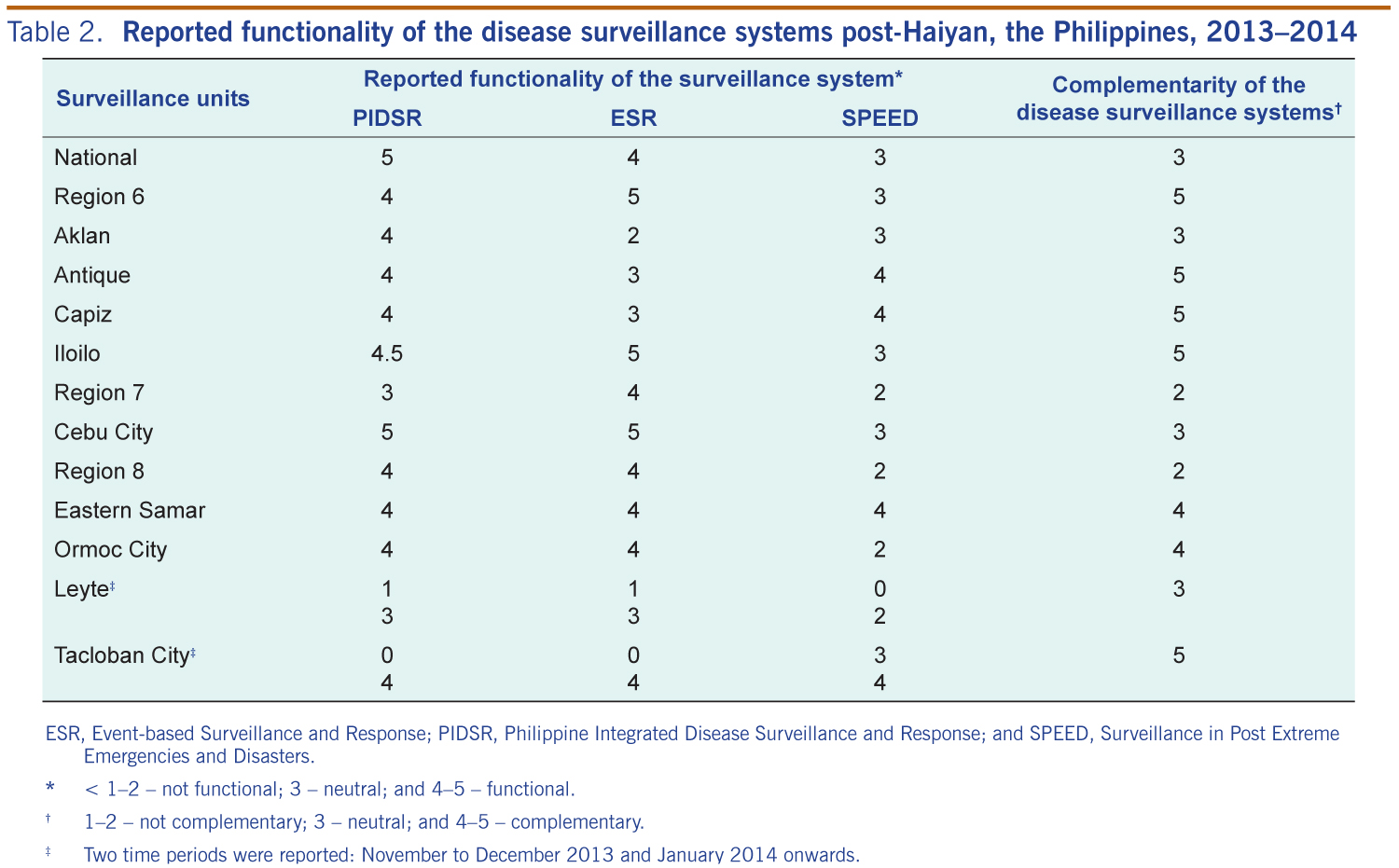
Ten of 11 (91%) surveillance units rated PIDSR as functional post-typhoon. Eight (73%) considered ESR functional. SPEED was rated functional by three (27%) surveillance units (Table 1).
In Leyte and Tacloban City, PIDSR and ESR were rated separately for functionality from November to December and January onward as their situations changed. In the first period, both rated the three systems to be not functional. In January and onward, Leyte rated the functionality as neutral for both PIDSR and ESR, and SPEED as not functional. Tacloban City rated the three surveillance systems as functional at this time (Table 2).
ESR, Event-based Surveillance and Response; PIDSR, Philippine Integrated Disease Surveillance and Response; and SPEED, Surveillance in Post Extreme Emergencies and Disasters.
* < 1–2 – not functional; 3 – neutral; and 4–5 – functional.
† 1–2 – not complementary; 3 – neutral; and 4–5 – complementary.
‡ Two time periods were reported: November to December 2013 and January 2014 onwards.
Seven of 11 (63.6%) surveillance units reported that the three systems were complementary to each other post-Haiyan. Four (30.7%) rated the three systems as neutral and two (15.3%) rated them as less complementary to each other.
This study shows that in most of the surveillance units in the areas affected by Typhoon Haiyan, the routine surveillance systems (PIDSR and ESR) were not disrupted. The disruption in the routine surveillance systems in other areas lasted for only one week post-impact except in Leyte and Tacloban City where it took seven weeks to activate routine surveillance. The delay was due to the extent of the devastation after Haiyan due to power and network failures as well as unavailability of surveillance officers who were typhoon victims themselves. Region 6 had less disruption in the operations of the two systems compared to Region 8, which could be related to the magnitude of the devastation in the latter that reduced the ability to continuously perform routine surveillance activities.6
Almost all of the surveillance units had delayed activation of SPEED – which is recommended to be activated 48 hours after a disaster as per the guidelines.4,7 Despite extensive damage to the Region 8 health office, Tacloban City and Eastern Samar did activate SPEED the week immediately after Haiyan. This could be attributed to the haste at which emergency assistance was delivered by the national health office; other unaffected regional health offices; and from several international organizations.8 In Leyte, SPEED was activated seven weeks after Haiyan because the health facilities were severely damaged, most of the health workers were affected and there was a threat to the peace and order in the area.
Most of the surveillance units rated the routine surveillance systems as being functional, but few reported SPEED as functional. Some respondents were not confident of the functionality of SPEED because they had encountered various difficulties upon its application. Some of the difficulties – lack of proficiency in performing the syndromic approach and reverting to paper-based reporting due to power and network failures – have been reported previously for other similar systems.9
The majority of respondents reported that SPEED complemented PIDSR and ESR in such a manner that it guided the health officers to verify and validate the particular syndromes and the areas affected for possible outbreaks. Although ESR was functional also, events were not reported, most likely because this system also employs a syndromic approach similar to SPEED.
One limitation of this study is that the responses were subjective; therefore, different respondents may have different interpretations of functionality and whether the systems were complementary.
In this study, we observed that routine surveillance systems can function even after a disaster and more so when health infrastructures are less damaged. SPEED could be a useful disease surveillance system in future disasters or emergencies but may require better training among field workers. SPEED should not replace PIDSR and ESR as such systems can supplement the other two by rapidly generating reports from health units. Emphasis in disaster preparedness to establish the needed capability proficiency in health units to ensure the functionality of SPEED is required. We recommend refresher courses, simulations and on-site mentoring on SPEED to enhance the surveillance and health officer’s capabilities.
None declared.
This study was funded by WHO.
We express our gratitude for the full support and cooperation of all PIDSR-ESR surveillance officers, Health Emergency Management Bureau and SPEED coordinators as well as all the health managers/officers from the national, regional and local government health offices in making this post-incident evaluation of disease surveillance systems possible.
{kind=link}
{kind=link}