a Office of the WHO Representative in the Philippines, Sta Cruz, Manila, Philippines.
b Bureau of International Health Cooperation, Department of Health, Sta Cruz, Manila, Philippines.
c Disaster Response and Management, Division of Health Security and Emergencies, World Health Organization Regional Office for the Western Pacific, Manila, Philippines.
Correspondence to Nevio Zagaria (email: zagarian@wpro.who.int).
To cite this article:
Peiris S et al. Is registration of foreign medical teams needed for disaster response? Findings from the response to Typhoon Haiyan. Western Pacific Surveillance and Response Journal, 2015, 6(Suppl 1):29–33. doi:10.5365/wpsar.2015.6.2.HYN_014
In the last three decades there has been an increase in the number of sudden onset disasters causing more than 800 000 deaths and affecting approximately 1 billion people.1,2 The Islamic Republic of Iran earthquake in 2003, South-East Asia tsunami in 2004, Pakistan earthquake in 2005, Pakistan floods and Haiti earthquake in 2010 all required an immediate health response, surpassing national capacities. A large number of foreign medical teams (FMTs) were deployed in these responses, for example more than 300 after the Haiti earthquake.3
FMTs are groups of health professionals and support staff operating outside their country of origin that provide health care to disaster-affected populations.4 They are classified according to team size, capability and capacity. Type 1 provides outpatient emergency care, Type 2 outpatient and inpatient surgical emergency care and Type 3 are inpatient referral care teams (capable of complex surgery and high-level medical care). Specialized teams provide specialist care, for example, orthoplastic care, dialysis and care for crush syndrome and maxillo-facial surgery.
Several FMT-related concerns have been reported, including teams arriving in an affected country without approval; lack of coordination, resulting in some areas over served and others underserved; lack of accountability; questionable professional standards of care and an absence of clear exit strategies.5
In September 2013, the FMT Working Group of the Global Health Cluster (GHC) published the Classification and minimum standards for FMTs in sudden onset of disasters,5 which outlines six guiding principles and 13 core standards that are to be observed by all FMTs, as well as the minimum technical standards per type of FMT and for each service.
Typhoon Haiyan was declared a Level 3 emergency by the Inter-Agency Standing Committee;6 calling immediately for international humanitarian assistance. As one of the world’s most disaster-prone countries,7 the Philippines has required FMT assistance in the past, and the Department of Health (DOH) has an established FMT coordinating mechanism which facilitates the entry, processing and accommodation of FMTs once they arrive incountry. However, this system does not assign the teams to their final operational destination.
For the response to Haiyan, the DOH adopted the new classification and registration form and it was the first time the form had been used globally. Although a description of the FMT’s response for the first month following Typhoon Haiyan has been published to our knowledge,8 no study has documented the classification and registration process of FMTs. Therefore, this paper aims to document the new FMT classification and registration process post-Typhoon Haiyan and provide recommendations for the review of the Classification of minimum standards for FMTs in sudden onset of disasters.
We conducted a descriptive study on the deployment of all FMTs to Haiyan-affected areas in the Philippines from 8 November 2013 to 30 June 2014. An FMT coordinating body was established at the national level which comprised representatives from the DOH and the World Health Organization (WHO) Representative Office in the Philippines. This team disseminated the new registration form to all FMTs that had contacted the WHO Western Pacific Regional Office, WHO Representative Office in the Philippines and the DOH from 10 November (two days after the typhoon made landfall). All FMTs were required to register regardless of their location inside or outside the Philippines at the time.
Completed registration forms were submitted via email and entered into an Excel spreadsheet. Information from the weekly monitoring forms and exit reports were also recorded in the spreadsheet along with daily tracking; updating and reporting of FMT activities, including the area of deployment, date of arrival, operational and demobilization dates and the health services being provided. Incomplete data fields were followed up by telephone and email to FMT coordinators and by triangulating information from other sources such as social media and external reports. During the response, this spreadsheet was analysed and presented twice a day on thematic maps posted on the web with the operational status and type of each FMT, location, final destination and expected day of departure. We analysed the final version of the spreadsheet up until 30 June 2014.
Information on non-registered teams was provided from Health Cluster hubs; these non-registered teams were classified using the GHC definitions (i.e. FMT Type 1) even if the number of staff was lower than specified. All information about these teams was added to the spreadsheet. Only the registered and non-registered FMTs known to the national FMT coordinating body were included in this study.
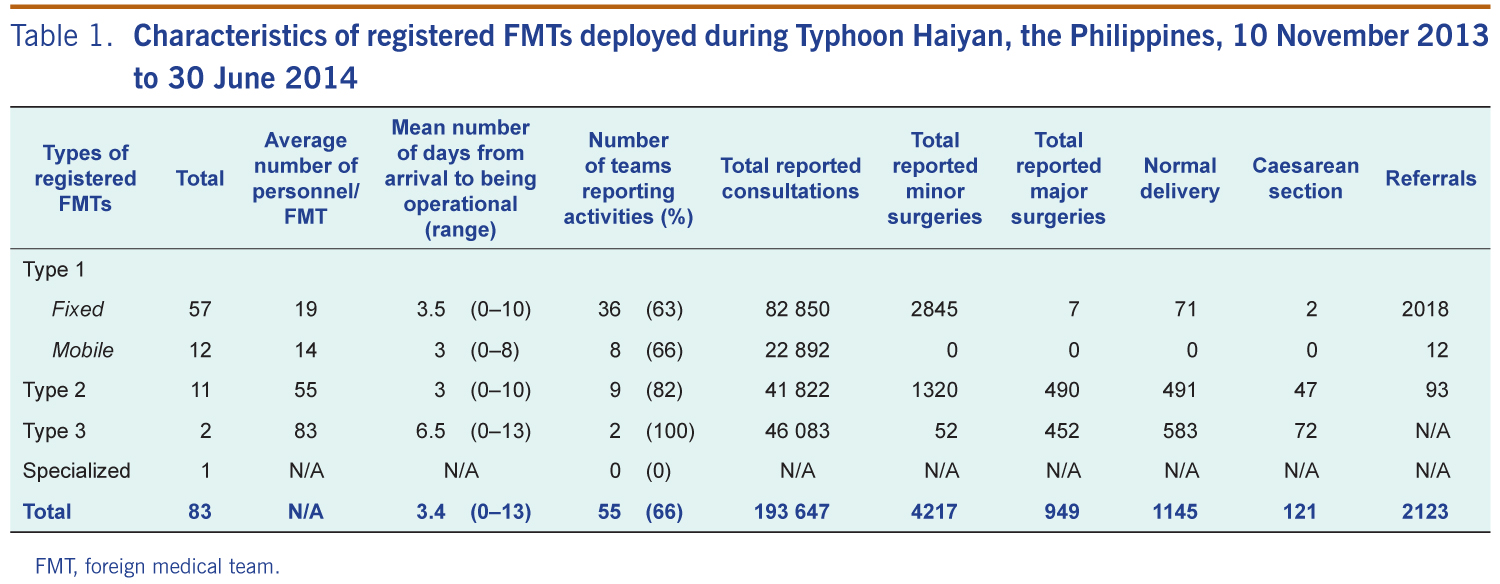
There were 150 FMTs that provided health services during the Haiyan response; 83 were registered using the new GHC registration form; 67 were not registered. The majority of the 83 registered FMTs were Type 1 (57 fixed and 12 mobile), 11 were Type 2 and two were Type 3. One registered FMT was a specialized FMT, providing ophthalmology services (Table 1).
FMT, foreign medical team.
All registered FMTs reported their total staff number with two thirds reporting their team composition (54/83, 65%). The average number of personnel in a registered Type 1 fixed, Type 1 mobile, Type 2 and Type 3 FMT were 19, 14, 55 and 83, respectively.
For all registered teams, the mean number of days from arrival in country to being operational (i.e. providing services) was 3.4 days (range: 0–13 days). The Type 3 FMT took 6.5 days due to the complexity of the set up of their required structure. There was no observed difference between Types 1 and Type 2 FMTs on this indicator, despite the more complex structure and higher number of team members of the Type 2 versus Type 1 (Table 1).
More than two thirds of registered teams (n = 55) submitted weekly reports and/or exit reports (Table 1). These teams reported a total of 193 647 consultations (including 2018 patients referred to higher level health care), 949 major surgical procedures, 4217 minor surgical procedures, 121 Caesarean sections and 1145 vaginal deliveries.
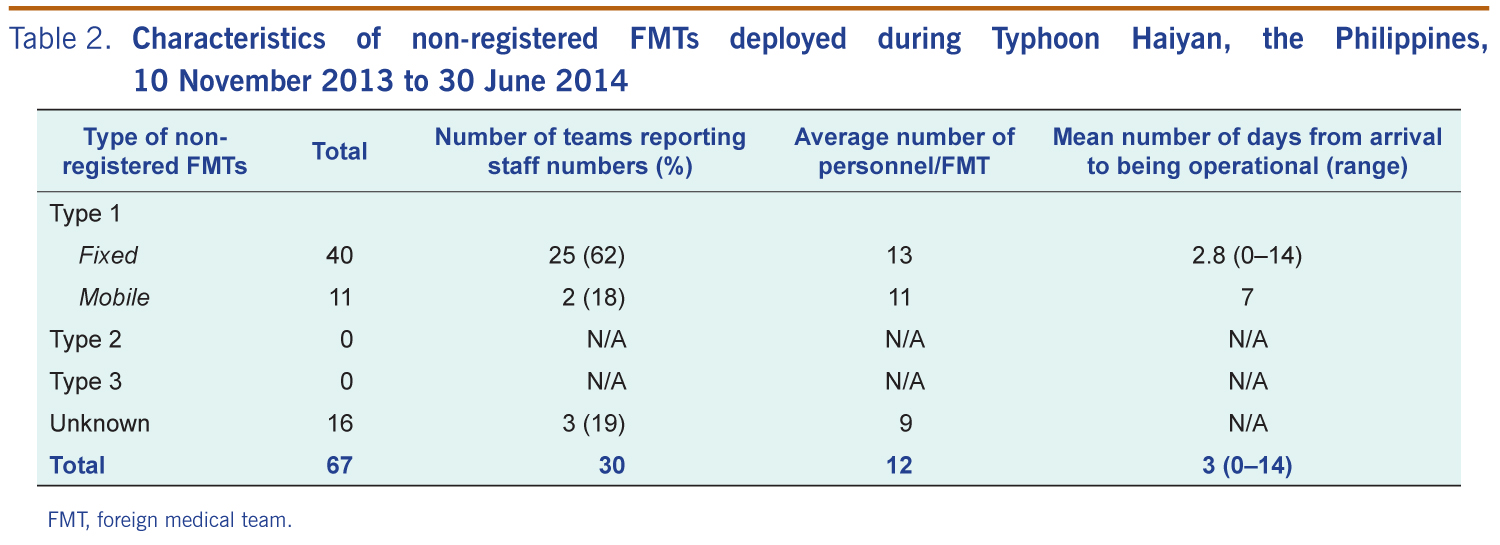
In addition to the 83 registered FMTs, there were 67 FMTs in other operational teams (Table 2). Most were Type 1 fixed (n = 40), 11 were Type 1 mobile, while for 16 (19%) the type was not recorded. Staff numbers was recorded for 30 of these FMTs (45%) with an average staff number of 12. There was an average of three days between arrival and service delivery. None of the 67 non-registered teams submitted reports to the DOH or WHO outlining the services they provided.
FMT, foreign medical team.
Adopting the new classification system for FMTs for the Haiyan response was beneficial as it provided a clear and precise description of the characteristics of each FMT type.8 It improved the coordination of the teams, especially in allocating the geographical location for each FMT. The registration process occurred before the arrival of some teams in the Philippines, thus reducing the time to become operational after arrival.
Most of the registered Type 2 teams had their own field hospital tents with an operating theatre, and all had prior experience in responding to disasters. They were aware of the mechanisms for coordinating a humanitarian response and were operational within a shorter time frame than Type 1 teams, despite having more staff, equipment and medical supplies. This shorter time frame was also due to the information provided by the teams on the registration forms which allowed the logistics hubs at the Ninoy Aquino International Airport in Manila and Mactan–Cebu International Airport in Cebu to facilitate their arrival efficiently.
Being registered allowed for FMTs to be matched to the health needs in the affected area, which prevented an oversupply of FMTs in one location. Knowing the composition of most registered teams assisted with team assignment and sometimes relocation based on changing needs. The location of all registered teams was mapped using a geographic information system; team location was updated twice daily for the first three weeks, then daily for the following two months and was posted on the web for the general public. As there were five regions impacted by the typhoon, the maps helped to strategically position the FMTs, in particular Type 2 FMTs, to ensure referral capacity between Type 1 and Type 2. This was not possible for the non-registered FMTs, none of whom had previously been used in a disaster in the Philippines.
Unlike in other sudden onset disasters,9 the need for surgical and trauma care was limited to the initial two to three weeks post-Haiyan, then changed to a high demand for general practitioners, reproductive and public health specialists. By registering FMTs, the DOH was able to ask teams to exclude trauma specialists and include primary care and public health specialists instead.
All registered teams reported the total number of staff; this information was available for less than half the non-registered FMTs. The average number of staff for the registered Type 1 fixed and mobile FMT was 19 and 14, respectively compared with 13 and 11 for the reported non-registered FMTs. FMTs are required to have a minimum number of staff to achieve maximum efficiency and be fully self-sufficient. Because non-registered FMTs had fewer than the required number of staff, the quality of service delivery was questionable. Most of the non-registered FMTs arrived four to six weeks after Haiyan and most of these teams were small with little or no medical equipment so they were only able to operate in the easily accessible areas, such as Tacloban City.
Activity reports and exit forms were submitted to the DOH by most registered FMTs; these were also used to determine if the teams upheld FMT minimum technical standards.10 The non-registered teams did not provide any reports, although some external reports from these teams were found through social media searches by the DOH and WHO. This highlights a lack of knowledge of the guidelines for FMTs and suggests that most of these non-registered teams were ad hoc and formed rapidly to respond out of benevolence and solidarity. Although noble, they did not comply with the core FMT standards; many were not self-sufficient for drug and medical supplies or food and logistics for their staff, causing additional burden. This influx of non-registered teams was possible due to the waiver for professional license processes and registration fees and the relaxation of visa and immigration regulations for foreign humanitarian workers and volunteers made by the Philippines’ Professional Regulations Commission11 and Bureau of Immigration.12
As the registration form was used for the first time, there were some issues with the process. The form did not capture all information on classification and minimum standards, so whether these standards were met could not be assessed. There was no debriefing for FMTs and lack of Internet access at the early stage of the response limited the ability to receive reporting forms that explained some of the incomplete information reported by registered FMTs. Another study concluded that poor data reporting made it impossible to fully assess the performance and activities of FMTs.7 The lack of information on the non-registered FMTs also limited documentation of the services they provided. Finally, we recommend the development of a FMT global and/or regional platform that would include a roster of available FMTs to share with WHO Member States such as the Global Foreign Medical Teams Registry.13
This study shows that the new FMT classification and registration process enabled the Philippines to strategically deploy international assistance according to the health needs in affected areas. It facilitated faster, more efficient deployment and helped ensure a coordinated, timely and credible response to the disaster.
We recommend that a similar process be used for future responses, although we recommend that the classification of Type 1 FMTs be expanded to differentiate between Type 1 fixed and mobile FMTs as reported in this study. We also recommend mechanisms to enforce the registration of all FMTs, and the timely reporting and monitoring of FMT activities. A standard exit report should be developed and required to be submitted before leaving the country. We also recommend that the registration form include the details of the breakdown of the international staff deployed to be able to check compliance with minimum standards. Finally, we recommend the development of a FMT global and/or regional platform that would include a roster of available FMTs to share with WHO Member States. This will then support countries that request assistance in the future and allow for more accurate and faster waiver processes for visas and licensing. These measures could greatly improve coordination and quality of the health sector response to disaster.
None declared.
None.
The authors would like to acknowledge the support of Dr Teodoro Herbosa, Undersecretary of Health, DOH Philippines, for his role as DOH FMT coordinating team leader during Typhoon Haiyan. Likewise, we would like to thank Dr Julie Lyn Hall, WHO Representative in the Philippines, and Ms Maylene Beltran, Director of the Bureau of International Health Cooperation, DOH Philippines, for their amazing support throughout the response. We would also like to thank all the FMTs that responded.
{kind=link}
{kind=link}