a Office of the WHO Representative in the Philippines, Sta Cruz, Manila, Philippines.
b World Health Organization Regional Office for the Western Pacific, Manila, Philippines.
c Department of Rehabilitation Medicine, Eastern Visayas Regional Medical Center, Tacloban City, Leyte, Philippines.
d Handicap International, Avenue des Frères Lumières, Lyon, France.
Correspondence to Mylene Rose Benigno (email: benignom@ wpro.who.int or myles_md@yahoo.com).
To cite this article:
Benigno MR et al. Responding to the health and rehabilitation needs of people with disabilities post-Haiyan. Western Pacific Surveillance and Response Journal, 2015, 6(Suppl 1):53–59. doi:10.5365/wpsar.2015.6.2.HYN_010
Introduction: It is estimated that 15% of the world’s population has a disability, and disasters increase their risk and vulnerability. Rehabilitation services were limited in the area of the Philippines that was affected by Typhoon Haiyan. This study describes the initial rehabilitation needs assessment and activities to increase rehabilitation services conducted in Leyte province of Region 8 after Haiyan.
Method: A rehabilitation needs assessment for people with disabilities and injuries needing physical and functional rehabilitation care and assistive devices was conducted in health facilities, evacuation centres and selected municipalities in Leyte province between 9 November 2013 and 30 April 2014 by a consortium of agencies. Improvements to service delivery and referrals were documented.
Results: Rehabilitation services were reduced immediately after Haiyan, but they increased in the following months and peaked four months after Haiyan. There were 2998 individuals needing medicine and rehabilitation management, functional care and assistive devices. These included persons with pre-existing disabilities whose situations had worsened and people who had sustained injuries in the typhoon. Additional improvements included rehabilitation services with provision of assistive devices at the regional hospital, development of a directory of disability services in the region and advocacy through community-based rehabilitation.
Discussion: Information services and community knowledge for people with disabilities improved in Region 8 after Typhoon Haiyan, demonstrating that strengthening rehabilitation systems is a realistic goal after disasters.
More than a billion people, or about 15% of the world’s population, are estimated to live with some form of disability.1 Disability, as defined by the International Classification of Functioning, Disability and Health, refers to an impairment, activity limitation or participation restriction that is the result of the interaction between health conditions and environmental and personal factors. It relates to the body functions and structures of people, the activities people do, the life areas in which they participate and the environmental factors that affect these experiences.2
Disasters impact people with disabilities disproportionately; in settings where resources are limited, like the Philippines, the impact of disasters on these people can be long-term and far-reaching.3 Disasters affect people with existing disabilities and create a new generation of people with disabilities, most of whom will need rehabilitation services. People with disabilities are at an increased risk in emergency and disaster situations.4 They may experience increased vulnerability due to limited access to information, healthcare and rehabilitation and loss of support networks, especially if family and caregivers are killed or injured in the disaster.5 During the disaster, they may have more difficulty evacuating; following the disaster, they may have difficulty physically accessing essential service (latrines, water, etc.). Losing an assistive device in a disaster, such as an artificial limb, hearing aide or spectacles, also increases vulnerability.
In the Philippines, rehabilitation services are limited, particularly in the public (government-funded) health sector, and are mainly found in major cities in Level 3 hospitals.6 Most specialists, particularly physiatrists, practice in the National Capital Region (Manila).7 Rehabilitation, as defined for the scope of this paper, is a set of measures that assist individuals with disabilities, both pre-existing and new, to achieve and maintain optimal body function in interaction with their environment.1
Nationwide in 2011, there were 305 729 low-income households with members having disabilities. Region 8, the area most affected by Typhoon Haiyan, had 13 478 low-income households in which people with disabilities lived.8 Following Typhoon Haiyan in November 2013, all six hospitals in Tacloban City, the capital of Leyte province, that previously offered rehabilitation services were devastated. The entire physical therapy unit of the Eastern Visayas Regional Medical Center (regional hospital) was flooded, most of the therapeutic equipment was destroyed and medical records were water damaged. Shops that sold assistive devices (standard orthopaedic wheelchairs, crutches, walkers and canes) were also damaged. Like the rest of the people of Tacloban City, hospital and health personnel were also victims of the disaster. Immediately after Haiyan, all services, including rehabilitation services for people with disabilities and injuries ceased at both in- and out-patient facilities. Some limited services resumed a few weeks after the disaster with the help of local and international volunteers and the establishment of temporary facilities such as field hospitals.
In this paper we describe the needs assessments and the activities conducted to increase access to rehabilitation and other services for people with disabilities and with injuries. The assessments were conducted by the World Health Organization (WHO), Handicap International (HI), Department of Health (DOH) and rehabilitation medicine specialists in Leyte province during the acute response up to April 2014, five months post-Haiyan.
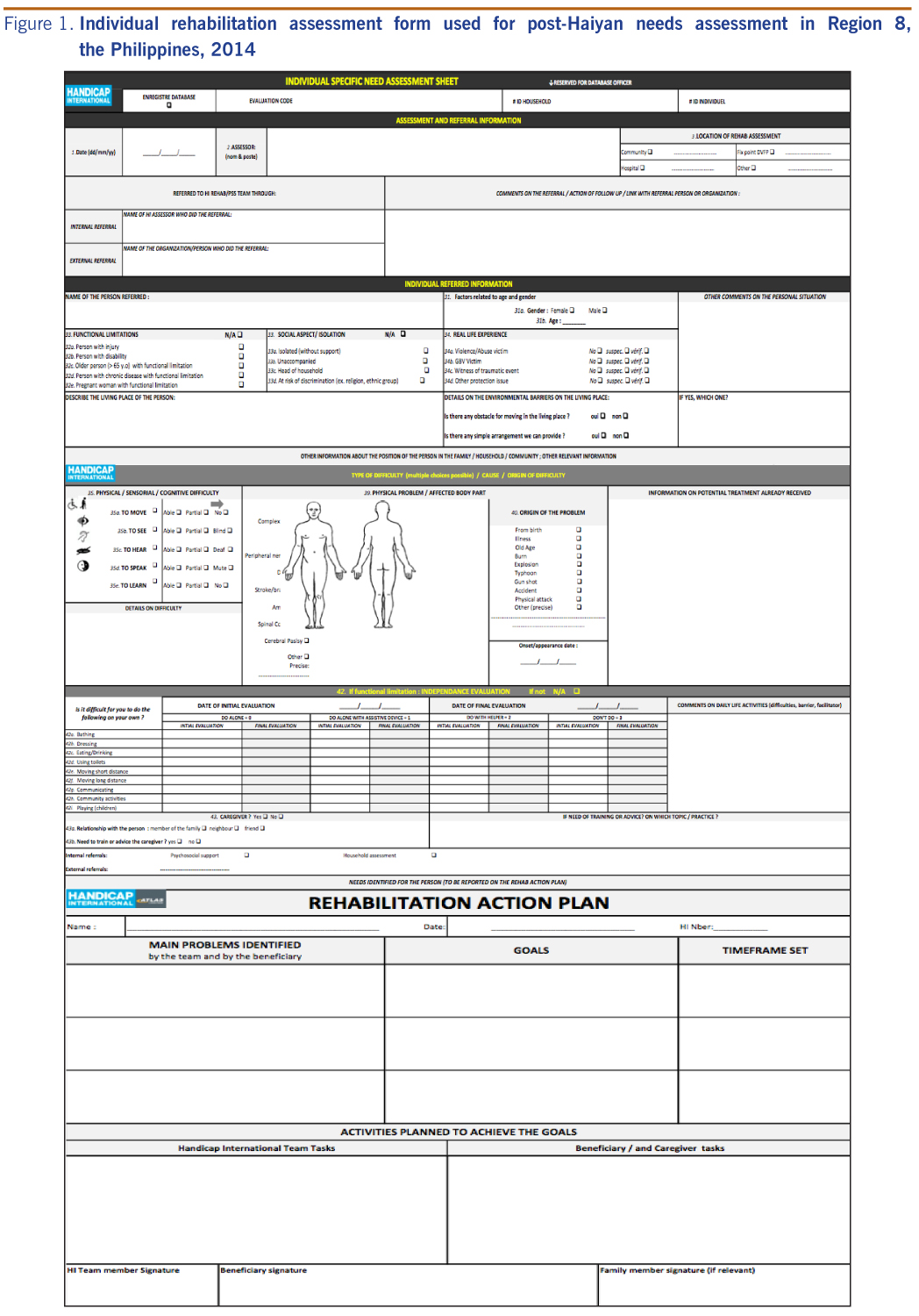
A rehabilitation needs assessment for people with disabilities and injuries needing physical and functional rehabilitation care and assistive devices was conducted in health facilities (four hospitals and four temporary field hospitals), evacuation centres and selected municipalities (Alang-Alang, Babatngon, Palo, Pastrana, Sta Fe, Tacloban City, Tanauan and Tolosa) in Leyte province, Region 8 between 9 November 2013 and 30 April 2014 by HI through a grant agreement with WHO using the individual rehabilitation assessment form (Figure 1) and by rehabilitation specialists of tertiary hospitals in Tacloban City. People with injuries and disabilities were assessed according to their physical, sensorial and cognitive difficulties and functional limitations in performing activities of daily living such as eating, drinking, dressing, bathing, toileting, moving, communicating and playing with children.
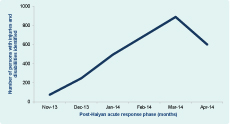
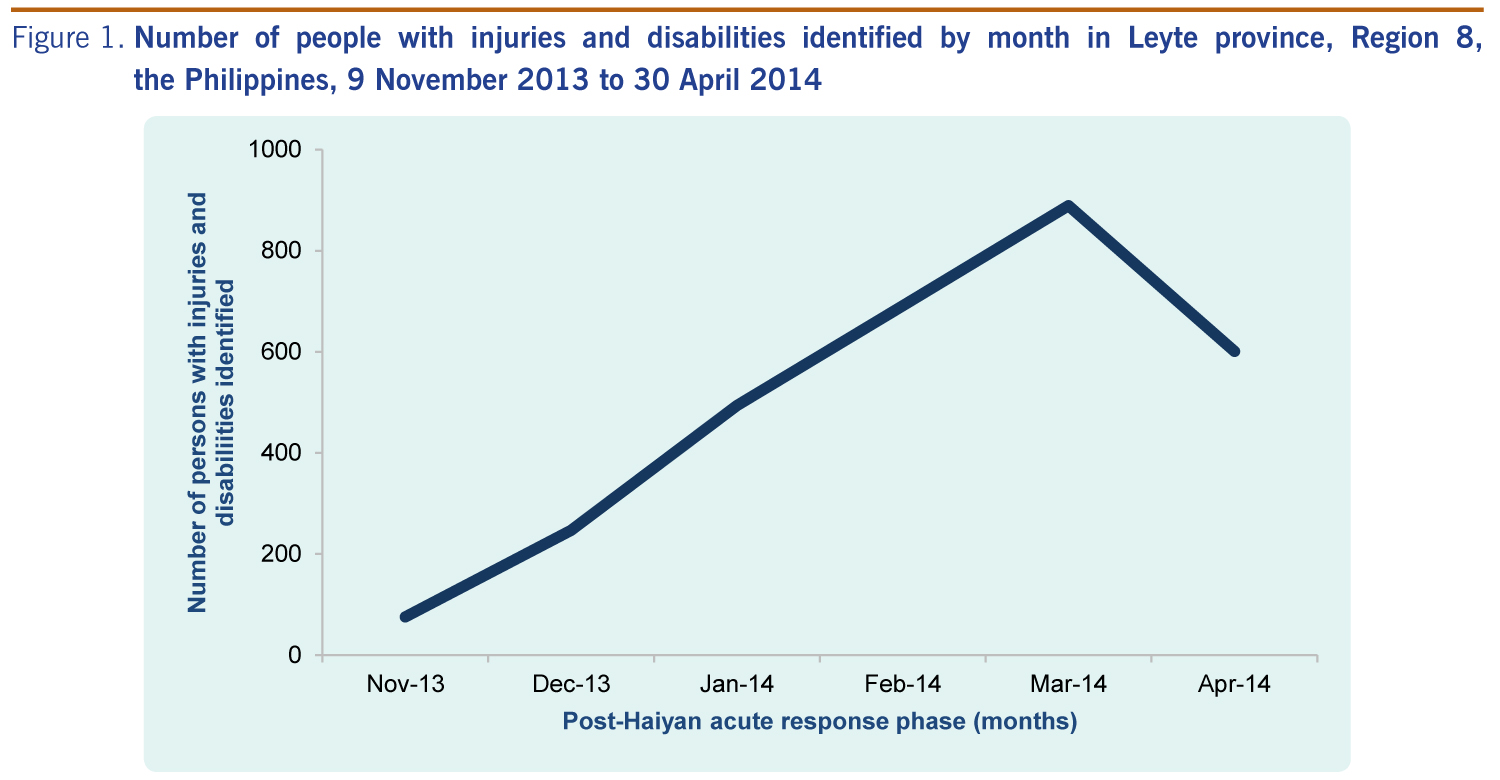
There were 2998 individuals identified as needing physical medicine and rehabilitation management, functional care and assistive devices, including persons with pre-existing disabilities and people who had sustained injuries in the typhoon. There was a consistent increase in the number of cases identified from November 2013 until the peak during March 2014 when a total of 889 patients were seen reflecting peak in referrals and availability of services (Figure 2).
More people were identified in health facilities compared to in the community (2232 versus 766, respectively) due to limited human resources and accessibility to the community (evacuation areas and houses). All needed rehabilitation services were delivered, including independence training in daily activities, proper transfer and transition techniques, therapeutic exercises, and gait and mobility training on how to use the assistive mobility devices.
Almost 400 devices, including 50 prostheses and 320 mobility devices (133 canes, 98 crutches, 50 walking frames and 39 wheelchairs), were provided to people with new injuries or pre-existing disabilities.
Many people with disabilities were evacuated to Manila, however, the exact number is unknown. Based on hospital records gathered from the major hospitals in Manila and Cebu with comprehensive rehabilitation medicine services, forty people needing critical care and rehabilitation management were transferred from Region 8.
Prior to Typhoon Haiyan, there were few rehabilitation services in Leyte province and they were commonly led by rehabilitation medicine specialists. Of the 79 hospitals in Region 8, rehabilitation services were only provided in nine (11% of hospitals); two were government hospitals offering services at reduced costs (2.5% of hospitals). One of these was the Eastern Visayas Regional Medical Center (EMVRCM) in Tacloban City, a regional hospital which offered primarily home-based exercise programmes as physical therapy services.
Following Haiyan, strengthening these services was a priority for hospital management and the DOH. In April 2014, five months post-Haiyan, EVRMC established a Department of Rehabilitation Medicine that increased the coverage of rehabilitation services to include not only physical therapy but also physiatric consultations, occupational therapy sessions and provision of prostheses and orthoses. A workshop to manufacture for prostheses and orthoses was established to cater to the demand from the rehabilitation medicine team (physiatrist, physical therapists and occupational therapist), and it became the first provider of prostheses (e.g. artificial legs) and orthoses (e.g. leg braces) in Region 8. Psychiatry and social services were also provided in the hospital as an integral part of rehabilitation.
The WHO Representative Office in the Philippines contributed to improving rehabilitation medicine by procuring rehabilitation equipment (e.g. therapeutic ultrasound, resistive exercise products and fine motor and dexterity activity sets).
As a result of these improvements, the regional hospital provided rehabilitation to more patients, including those in critical care units, for a wider range of musculoskeletal and neurological conditions. The number of patients receiving rehabilitation in the regional hospital grew from 533 patients per year before Haiyan to 1547 in 2014.
A Directory of Health, Rehabilitation and Disability Services for Region 8 was published in November 2014.9 This directory served as a guide for all personnel advocating, treating and caring for people with disabilities in the health and social welfare sectors as it provided information on available services, including health professionals and facilities, sources of assistive devices, schools and therapy centres, support groups, disabled persons organizations and professional groups. With all this information in one directory, people with disabilities had better access to information on various services and programmes.
Most of the key stakeholders in the disability sector (18/25, 72%) attended the launch of the directory. It was also distributed to government offices, nongovernmental organizations and their substituents in all six provinces of Region 8.
Community-based rehabilitation (CBR) is a programmatic approach to increase awareness and inclusion of people with disabilities at the community level and was implemented by the local government with support from WHO. The post-Haiyan CBR initiative was developed through orientation lectures, situational analysis, resource mapping, development of a plan of action and formation of a CBR working group. Tacloban City was chosen as the model city for CBR, in line with the Presidential Order, and the mayor designated an officer and provided an office space.
At the regional and provincial level, there was participation by most key stakeholders (21/25, 84%) in CBR orientation and training conducted by WHO from 20 to 21 November 2014. Attendees included officers from the departments of Persons with Disability Affairs Office (PDAO), Welfare and Social Development, Health, Education, Public Works and Highway, Interior and Local Government, Transportation and Communications, Budget and Management as well as other components of the Regional Committee on Disability Affairs, professional groups and disabled persons organizations (DPO).
At the city level, CBR orientation and workshops were conducted in Tacloban City by WHO from 23 to 24 October 2014; these were well attended by 88% (22/25) of key stakeholders. These included local government representatives, city officials from social welfare and development, budget, health, hospitals, special education, planning, Public Employment Service Office, professional groups (doctors, teachers), DPOs (Autism Society, Parent group, PWD cooperative), nongovernmental organizations and advisers from the National Council for Disability Affairs (NCDA). A PDAO-CBR Technical Committee was formed in Tacloban City comprised of 18 members of key stakeholders, line agencies and advocates. The group worked on budget proposals and plans of actions for the city’s priority disability programmes.
At the community level, CBR training and orientation was conducted at all 138 villages in Tacloban City by WHO from 13 to 19 March 2015. Information on CBR was disseminated widely through the barangay captains, health workers, day care workers and volunteers. As a result, the issues faced by people with disabilities are more widely known. During the sessions, disability issues (awareness, sensitization, data consolidation, education, livelihood, employment, organization, participation, health services, social welfare) were included in the barangay development plan and budget. The PDAO-CBR Technical Committee will continue to guide and strengthen the Tacloban City CBR program.
In March 2015, DOH conducted a two-day training course on disability-inclusive health and rehabilitation services at the primary health care level. Approximately 50 non-specialist doctors and nurses participated from selected cities and municipalities of Region 8. The training presented the various laws regarding people with disabilities, the range of services needed, and the specific people, agencies and facilities in Region 8 that can address disability needs.
At the national level, the NCDA produced and disseminated two advocacy documents promoting consultation and inclusion of people with disabilities in rebuilding efforts.
Several other tools were collaboratively developed to promote disability awareness at the community level in Region 8. The most widely reproduced was a poster advocating actions for information, empowerment and respect for people with disabilities. The posters were distributed to all 510 government offices and nongovernmental organization in Region 8 and promoted positive behavioural changes in the community.
Rehabilitation services for people with disabilities are necessary and can be effective after a disaster. Although rehabilitation services at the regional hospital in Leyte province declined immediately after Haiyan, they increased in the months following to a peak of people accessing these services four months after Haiyan. This increase in patients can be attributed to the improvement in services at the regional hospital as well as increased awareness of the referral system.
Haiyan provided an opportunity to “build back better” in terms of infrastructure and service development, particularly at the regional hospital, which was significantly damaged. Expansion of services in the region helped decentralize specialized disability services that were previously only available in Manila and Cebu.
The fact that services, information and community knowledge for people with disabilities improved in Region 8 after the initial needs assessment post-Haiyan shows the importance of conducting such assessments after a disaster to critically address the specific needs of people with disabilities. In a relatively short period of time, i.e. five months, sustainable improvements in health service delivery resulted in more than double the number of people with disabilities being seen for a wider range of conditions.
There were several approaches adopted which helped to ensure people with disabilities were accepted as contributing members of the community. One approach was disability-inclusive development and inclusion in recovery and rebuilding efforts; another was through the CBR initiative that resulted in the community having a better understanding of the needs of people with disabilities. An ideal CBR programme reduces the effects of poverty, promotes human rights and ensures dignity for all persons with disabilities and their family members.10
Some limitations to this work were that resources did not allow support to all areas of Leyte, rather it focused on selected municipalities. There were also other actors for disability that contributed to the response effort who were not part of this paper. It is likely that some underestimation of the number of people with disabilities and injuries occurred and other activities may not have been documented.
This study also found that detailed pre-disaster data were limited and that having estimations and profiles of people with disabilities in communities before a disaster would improve the response. Efforts to increase referral for the Philippines PWD Identification Card is currently being conducted through active identification through the PDAO office and through CBR referral efforts from the barangay health workers of Tacloban City;11 this would be one way to identify people with disabilities post-disaster. The needs assessment that was conducted has been the only assessment done in Region 8. Accurate situational assessments of needs and available services accelerated relief and recovery efforts and mitigated some of the consequences of Haiyan for this vulnerable population.
Developing rehabilitation services in all hospitals in the Philippines will improve the quality of life and decrease the burden of disease. Of significant concern is that only 11% (9 out of 79) of hospitals in Region 8 offered rehabilitation services. Advocating for wider implementation of Republic Act No. 10070, an Act to Establishing Institutional Mechanism to Ensure the Implementation of Program and Services for Persons with Disability in every Province, City and Municipality,11 will improve conditions for people with disabilities, not only after disasters, but all the time.
The number of people with disabilities and injuries increases after a disaster. Determining those who will need specific disability and rehabilitation services, as well as mapping these services, are vital responses following a disaster. Inclusion of people with disabilities in initial health assessments should become routine after disasters. Without information about the situation and the services, the conditions of people with disabilities and injuries will worsen over time.
Working with health, rehabilitation and disability sectors is essential for improving access to services for people with disabilities. Improving the coordination and planning between these stakeholders, for example through development and utilization of the regional service directory and CBR programme development, increased access to services. This study demonstrated that improving services and increasing coordination between services, beyond pre-disaster levels, was a realistic goal.
None declared.
None.
We thank the Eastern Visayas Regional Medical Center, Divine Word Hospital and Remedios T Romualdez Hospital for their involvement in this work. We also acknowledge HI for conducting the initial needs assessment and providing the data.
{kind=link}
{kind=link}