a Office of the WHO Representative in the Philippines, Sta Cruz, Manila, Philippines.
b Health Emergency Management Bureau, Department of Health, Sta Cruz, Manila, Philippines.
Correspondence to Allison Gocotano (emails: gocotanoa@who.int or allisongocotano@gmail.com).
To cite this article:
Gocotano A et al. Is the response over? The transition from response to recovery in the health sector post-Typhoon Haiyan. Western Pacific Surveillance and Response Journal, 2015, 6(Suppl 1):5–9. doi:10.5365/wpsar.2015.6.2.HYN_007
The Philippine National Disaster Risk Reduction and Management Plan divides disaster management into four phases: (1) prevention and mitigation; (2) preparedness; (3) response; and (4) recovery and rehabilitation.1 The recovery process is defined as “a sequence of interdependent and often concurrent activities that progressively advance a community toward a successful recovery” and extends from ongoing preparedness to long-term recovery with an overlap between the acute response and short-term and intermediate recovery.2 In this paper, this period of overlap between response and recovery in the Philippines occurred three to seven months post-Typhoon Haiyan – February 2014 to July 2014.
The need to define when recovery began post-Haiyan had programmatic implications which included (1) waiving the normal policy of donated medicines and shouldering the tax duties of donors, (2) waiving the licence to practise medicine for foreign professionals and (3) expedited government and non-government administrative processes during an emergency. Government and humanitarian actors needed a common understanding of the different phases of the emergency to determine programme priorities. For instance, the tuberculosis programme prioritized tracing all patients (and records) and restoring their treatment in the response phase; in the recovery phase, active case finding was resumed.3 The Philippines’ Surveillance in Post Extreme Emergencies and Disasters (SPEED), the mobile-based early warning system, was implemented during the response phase and should be shifted to the Philippine Integrated Disease Surveillance and Response system in the recovery phase.4
During the overlap period between response and recovery activities, the authors were all working in the health sector at the national level supporting coordination and strategic planning with government and partners and at the field level implementing response activities and revisiting the medium- and long-term programming approach to recovery. It is from this perspective, combined with data from existing documents such as plans, reports and policies, that we highlight the need to define a period of transition from response to recovery of the health sector as it may have important implications on the health system functioning as a whole.
The Philippine Government declared a State of National Calamity on 11 November 2013, three days after the typhoon, triggering the involvement of the international community. The Philippine health sector response started before this declaration and was characterized by the deployment of personnel, monetary assistance and the distribution of goods for lifesaving measures in preparation for anticipated health needs. The Emergency Relief Coordinator formally activated an Inter-Agency Standing Committee (IASC) Level 3 emergency response the following day (12 November), noting that the magnitude of this sudden-onset humanitarian crisis justified system-wide resource mobilization.5 A massive international response was launched, and more than 450 international, surge-capacity staff of various expertise were deployed within three weeks. The United Nations Humanitarian Coordination Team in the Philippines issued a humanitarian action plan on the same day as Level 3 activation.6
A month later, in December 2013, the Office of the Presidential Assistant for Recovery and Rehabilitation (OPARR) was established. OPARR was an ad hoc government agency mandated to coordinate, facilitate, and integrate the short-, medium- and long-term recovery plans with an overall strategic vision. Prior to Typhoon Haiyan, disaster rehabilitation efforts were overseen by the Philippine National Economic and Development Authority (NEDA) that worked with OPARR to monitor and evaluate the rehabilitation effort.
Plans issued from nongovernment and government sectors detailed damage and needs assessments, and the funding requirements for response. One month after Haiyan, the Strategic Response Plan was released by the United Nations Humanitarian Coordination Team detailing the health sector’s priorities to provide life-saving measures, immediate access to water, sanitation, hygiene and to re-establish health services to prevent increased morbidity and mortality.7 The Government, through NEDA, issued Reconstruction Assistance on Yolanda (RAY), a strategic plan to guide the recovery and reconstruction of areas affected by Typhoon Haiyan (Yolanda) over the short (2013 to 2014) to medium term (2015 and beyond).8 The health priorities of RAY were repair and reconstruction of public facilities to their pre-disaster state; risk reduction and community resilience, support for health services; mental health and psychosocial support; and governance strengthening.
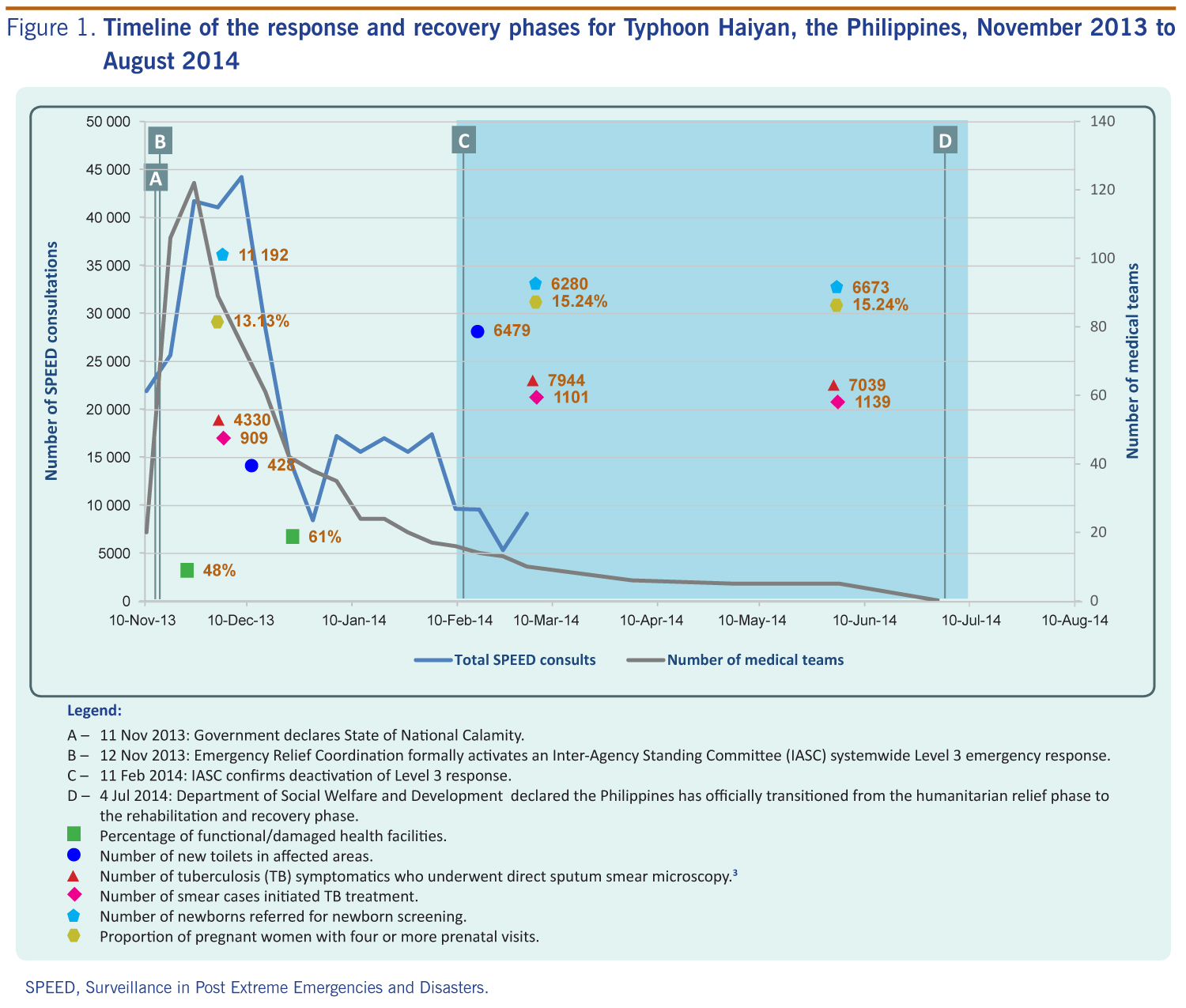
There were differing views as to when the response phase ended and recovery began. From the international view, IASC confirmed the deactivation of the Level 3 response on 11 February 2014 (three months after it was issued).5,9 From the national view, it ended when the Philippines officially transitioned from the humanitarian relief phase to the rehabilitation and recovery phase on 4 July 2014 (seven months post-Haiyan).10 This four-month difference between declarations represented the overlap between the response and recovery phases for Typhoon Haiyan from both perspectives, and in the context of this discussion, is labelled as the ‘transition phase’.
When Level 3 was de-activated, SPEED was seeing a decline in consultations to the level similar to normal conditions.11 Almost half of the foreign medical teams left after the first month of the response (Figure 1).12
SPEED, Surveillance in Post Extreme Emergencies and Disasters.
The decline of consultations and utilization of medical missions coincided with the work of nongovernmental organizations (NGOs) supplementing the health sector. Most of the NGO medical missions were funded and active between four and six months post-Haiyan. Since consultations had reduced, there was no urgency to continue their services. Around the fourth month, local governments took over the bulk of health service delivery to the people. Many of the international partners handed over patients and donated surplus medical equipment and supplies to local health authorities when they left. Of the health partners who stayed on, a shift from an emergency to a medium- to long-term development agenda was observed.
During this period, coordination of remaining health actors also evolved. While a cluster system of coordination was still operational at the national and regional levels, in March 2014, OPARR requested all health actors develop rehabilitation plans. These then formed the master rehabilitation plan, including activities for health facility repairs and construction for social services through support to several public health programmes.13 The private sector contribution was also documented in the OPARR master plan.
In May 2014, two months later, the transition to recovery was formalized when the national emergency response health cluster structure transitioned into the Health Sector Rehabilitation and Reconstruction Coordination Group.14 This national-level action was reflected at subnational government levels in three ways: (1) individual cluster meetings (health; water, sanitation and hygiene; nutrition; and mental health and psychosocial support) were integrated; (2) the frequency of meetings decreased from daily to monthly by June 2014; and (3) activities initially supported by the international co-cluster leads were gradually handed over to the government. The previously established five subnational level health coordination hubs (Ormoc, Roxas, Cebu, Tacloban and Eastern Samar) were reduced to four with the remaining hubs coordinating recovery work.15
As well as the ongoing disaster-related activities, annual operational plans had to be implemented by the government. In some instances this caused tension between international and government health workers. International health workers felt a strong responsibility to the still affected population and national health workers had a strong desire to rebalance priorities.6 Given this, minor setbacks in achieving routine outcomes were expected during this period. However, this was not the case post-Haiyan, as setbacks were minimal.
Similar indications of transition were observed in service delivery and health programmes during this four-month period. There was an increase in the percentage of functional health facilities in the affected area from 48% (139/289) in November 2013 to 61% (177/289) in December (Figure 1);16 functionality was an indication of continuity of basic health-care services. In addition, the increase in the number of toilets installed from 428 in December 2013, to 6479 in February 2014 addressed water and sanitation concerns.17 The local heath capacity was further improved with several trainings on long-term health programming. The Package of Essential Noncommunicable Disease Interventions for Primary Health Care in Low Resource Settings (PEN) started in June 2014 to address early detection and treatment in the community;18 the Mental Health Gap Action Programme (mhGAP), with more than 130 health professionals, institutionalized the mental health services at the primary care level.19 Another sign of a recovering health system was the improvement in selected indicators (Figure 1).3
The IASC, in its evaluation, concluded that transition included a change in (1) the nature of affected people’s needs (emergency to early recovery); (2) the type of programme approaches to meet changing needs (humanitarian to recovery to development); and (3) structures and systems for coordination of assistance (closure of response clusters).6 The lack of familiarity with the capacities of a middle-income country; differences between international and national planning time frames; and different views on the boundaries and linkages between emergency relief, early recovery and recovery all contributed to the complexities of transitioning from relief to recovery programming. Further complications were that sectors and regions recovered at different paces and uncertainty on the government’s timetable to begin large-scale recovery programmes.6
Labelling a temporal mark between response and recovery may have varying implications. First, the degree of significance of the emergency in terms of local and global attention could be altered with consequences on funding opportunities. Second, the declaration of recovery does not imply a reduced humanitarian need or that ongoing interventions can cease; rather, that there is a change in the type of assistance needed. Third, activities might be the same but are now viewed more from the outlook of proactive governance. This change in outlook from victims to survivors is an important factor in the normalization of day-to-day activities which facilitates recovery.
There is a growing notion that recovery starts immediately after an event, but the Haiyan experience showed the transition period was an overlap of different activities among non-government and government agencies at different levels of the health sector. There may have been variability in the way transition was experienced by key stakeholders, operationally and for reprogramming, and there were some improvements within the health system, such as the decrease of external medical teams, handing over patients to local health authorities, increase in functional health facilities as well as capacity-building activities through trainings like PEN and mhGap. Therefore, we suggest that there is no one-time point in which recovery begins, rather there is a transition period of response to recovery that may be different for each disaster. This transition involves the complex network of stakeholders and actions that define the transition period – a period where remaining gaps in response are addressed and that identifies the direction and speed of improving the state of the public’s health to better than what it was before the disaster.
None declared.
None.
The authors would like to thank the Philippines Department of Health, in particular the Health Emergency Management Bureau and Regional Offices 6, 7 and 8. We also extend our gratitude to the staff of WHO Representative Office in the Philippines for sharing their experiences and expertise. Finally, we would like to acknowledge those who worked on the front lines for the Typhoon Haiyan response and recovery.
{kind=link}