a Field Epidemiology Training Program, Epidemiology Bureau, Department of Health, Sta Cruz, Manila, Philippines.
b Department of Health, Sta Cruz, Manila, Philippines.
Correspondence to Paola Katrina Ching (email: paolaching@gmail.com).
To cite this article:
Ching PK et al. An assessment of disaster-related mortality post-Haiyan in Tacloban City. Western Pacific Surveillance and Response Journal, 2015, 6(Suppl 1):34–38. doi:10.5365/wpsar.2015.6.2.HYN_005
Introduction: Tacloban City was seriously affected by Typhoon Haiyan with 2321 deaths distributed across its 138 villages and subvillages. In January 2014, a team from the Department of Health conducted a mortality assessment to identify risk factors for deaths that occurred during Typhoon Haiyan.
Methods: A retrospective case-control study was conducted in the four coastal villages in Tacloban City with the highest numbers of typhoon-associated deaths. A case was defined as a person who died in Tacloban City during Typhoon Haiyan and whose body was recovered and identified. Controls were selected from surviving family members. Information about typhoon-related knowledge, attitudes and practices of the cases was collected using a standardized questionnaire.
Results: There were 100 cases and 100 controls included in the study. The cause of death for all cases was drowning, and all bodies were found inside or near their house. Multivariate analysis identified that the significant risk factors for mortality due to Haiyan were not evacuating before the storm hit (odds ratio [OR] = 10.0; 95% confidence interval [CI]: 3.8–29.1) and exiting their house during the storm (OR = 3.6; 95% CI: 1.9–7.1). Proxies reported that all cases had heard about the coming typhoon, but that 88% did not understand the message about the storm surge. Ninety-five per cent of cases did not evacuate because they did not expect the magnitude of storm.
Conclusion: Warning messages delivered before and during emergencies should be conveyed in terms understood by the population at risk. We recommend that the results from this study be used to develop more effective messages to be used before future disasters.
The Philippines is one of the most disaster-prone countries in the world due to its geographic location which renders it vulnerable to natural disasters.1 Between 2000 to 2012, 207 natural disasters were reported to have caused 12 899 deaths.2
As early as 4 November 2013, when it was known that Typhoon Haiyan was coming, the Philippine Government held emergency meetings for storm preparation in Tacloban City. Many local officials disseminated storm warnings by personally going to the area to inform the community that a super typhoon would arrive. Local government units designated evacuation areas in each village. Communities were warned that along with a very strong storm, a storm surge might occur, and residents were encouraged to evacuate.
After Typhoon Haiyan hit, Tacloban City was the major focus of devastation because of its location and its large population in low-lying areas. This paper describes a study conducted in January 2014 by the National Epidemiology Center and the Region 8 Epidemiology and Surveillance Unit team to identify factors for mortality and survival.
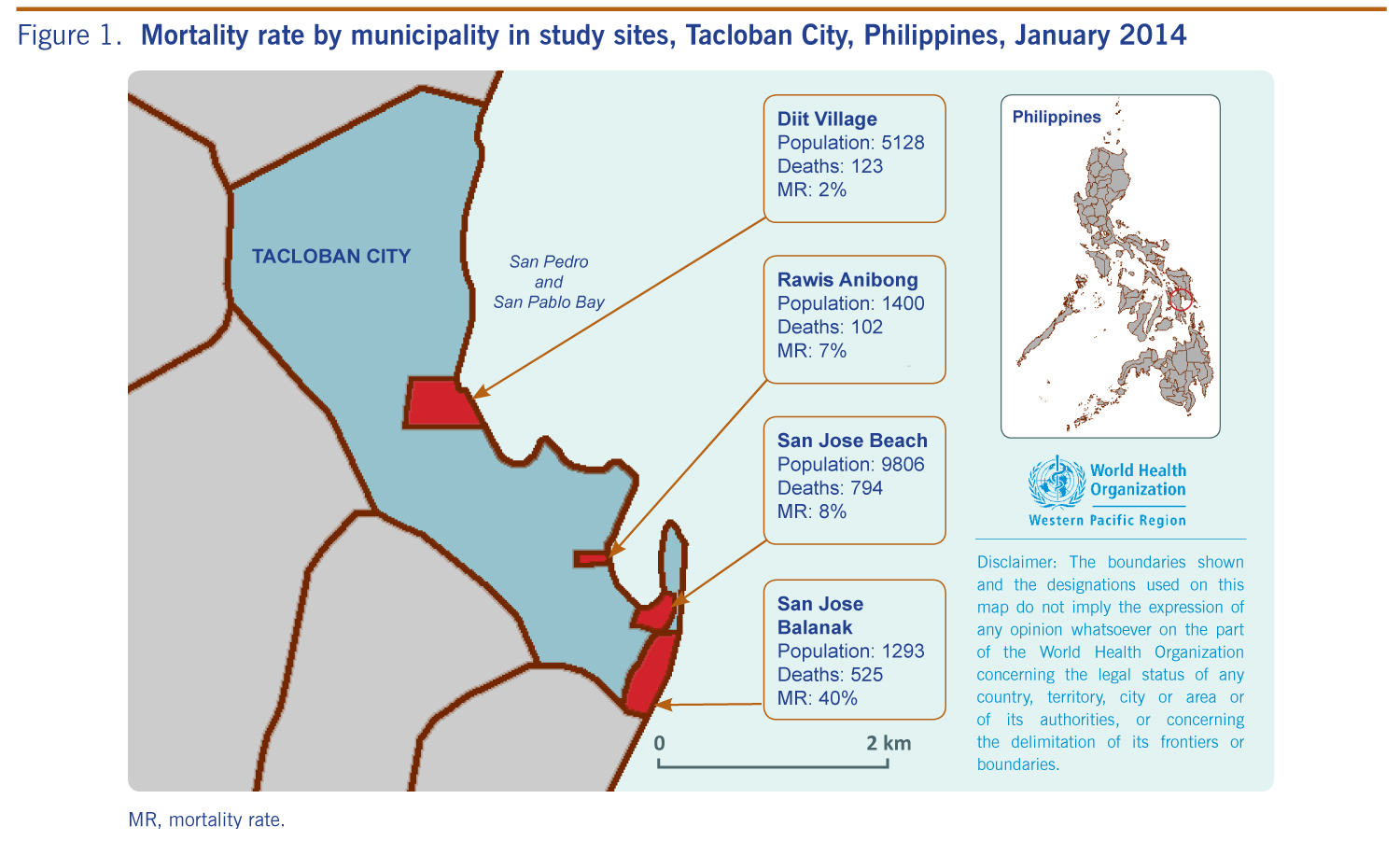
The four subvillages with the largest number of Haiyan-related deaths in Tacloban City were purposively sampled: San Jose Balanak, San Jose Beach, Rawis Anibong and Diit. The mortality rates for these subvillages were 40%, 8%, 7% and 2%, respectively (Figure 1). All were coastal areas.
MR, mortality rate.
To identify cases, we reviewed records from the village secretariat in these four subvillages and the roster of deaths in the Village Affairs Office. Available death certificates provided by relatives of the victims were validated to ensure that the bodies were recovered. Those with pending death certificates were verified at the Mayor Alfred Social Action Office. We calculated a sample size of 100 using a 95% confidence interval (CI) and a margin of error of 10%.
We conducted a 1:1 unmatched case-control study to identify risk factors associated with mortality from Typhoon Haiyan. A case was defined as a person who died during Typhoon Haiyan on 8 November 2013 and whose body was recovered and identified. A relative of each case was interviewed. A control was defined as a surviving family member of a case who was in Tacloban City at the time that Typhoon Haiyan made landfall. Only those aged more than 10 years were recruited as controls.
Relatives were found by searching in the community and evacuation centres, and were interviewed face-to-face. A knowledge, attitude and practice survey of cases only, through their proxies, was used to identify knowledge of the typhoon, behaviours as the typhoon approached and practices before and during the typhoon. We analysed risk factors using bivariate odds ratio (OR) and logistic regression models in Epi Info version 3.5.4.
All cases died inside or near their houses with drowning as the documented cause of death. There were 52 cases from San Jose Beach, 34 from San Jose Balanak, eight from Diit and six from Rawis. The median age of cases was 41 years (range: 7 months to 81 years). Sixty-two cases were female (Table 1).
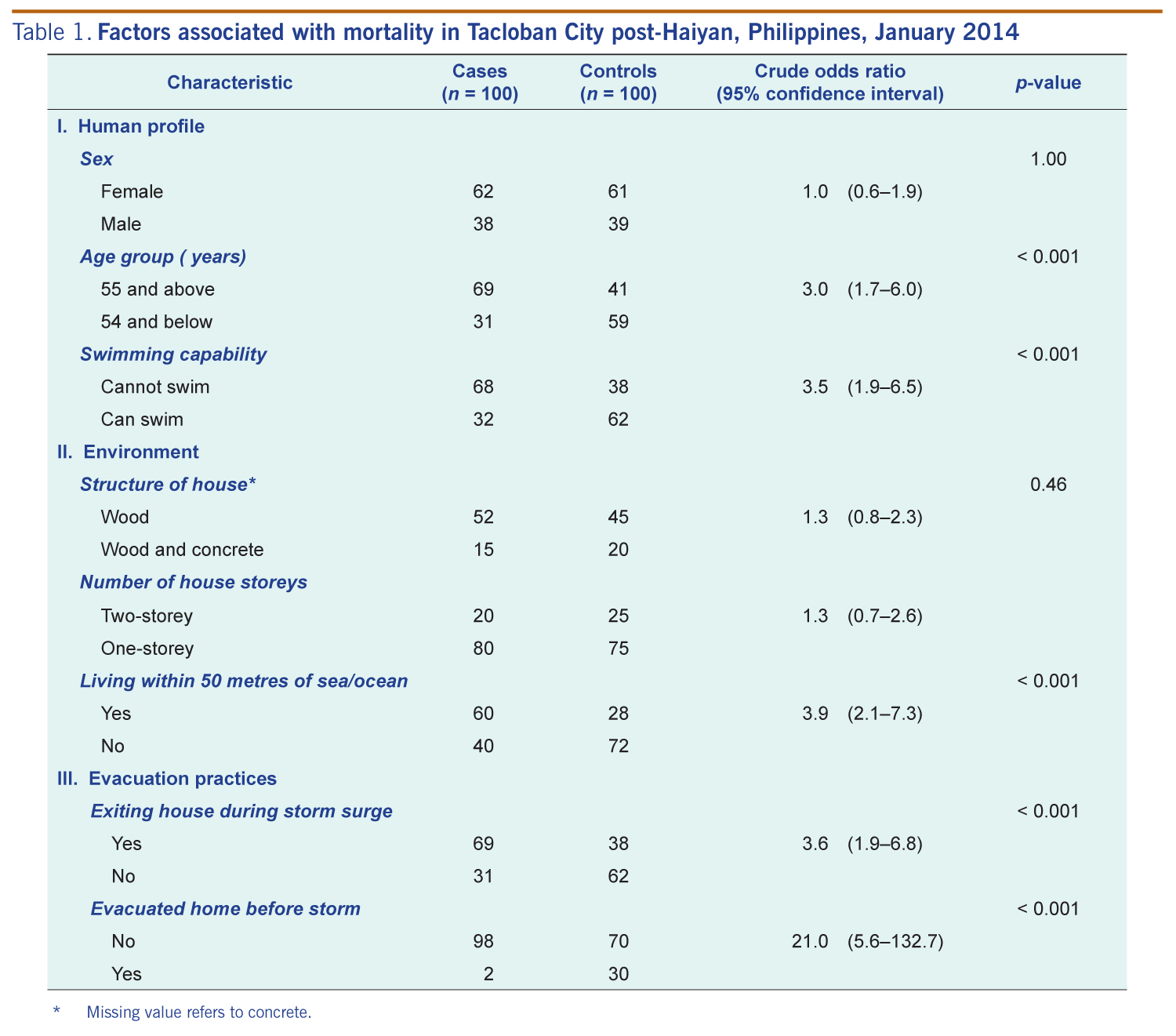
* Missing values refer to concrete.
There were 100 cases and 100 controls in the study. Univariate analysis identified several possible risk factors for mortality due to Typhoon Haiyan. Cases were more likely to be aged 55 years or older (OR = 3.0; 95% CI: 1.7–6.0), unable to swim (OR = 3.5; 95% CI: 1.9–6.5) and living within 50 metres of the sea or ocean (OR = 3.9; 95% CI: 2.1–7.3).
Factors associated with place of refuge during the storm associated with mortality included not going to the designated evacuation centre before the typhoon hit (OR = 21.0; 95% CI: 5.6–132.7) and exiting the house during the storm (OR = 3.6; 95% CI: 1.9–6.8). The material from which the houses were made and whether it was single or two-storey was not associated with death (Table 1).
The multivariate model identified two significant risk factors for death due to Typhoon Haiyan: not going to the designated evacuation centre before the typhoon (adjusted OR [aOR] = 10.0; 95% CI: 3.8–29.1) and exiting the house during the storm (aOR = 3.6; 95% CI = 1.9–7.1).
According to the proxy interviews, all cases knew the storm was approaching. A large percentage of interviewees (89%) stated that although the cases were warned about the storm surge they did not understand what this meant. Eighty per cent of cases were first informed about the storm surge through television and 10% by announcements from local officials using an outdoor speaker. Most (90%) reported that the cases did not know that staying in their place of residence was unsafe; 56% knew the designated place of evacuation, but most (98%) did not evacuate.
According to the interviewees, 76% of cases did not know about pre-existing village disaster plans. However, 58% reported that the cases had prepared for the storm, including 44 cases who stored food and water and eight who packed bags for evacuation. Among those who did not evacuate (n = 98), and who provided a reason (n = 74), it was reported that 55 cases were surprised by the magnitude of the storm, 19 stayed due to anxiety about the security of their home and belongings and 10 believed that their houses were sturdy enough to withstand the storm.
Evacuation is an integral part of disaster management and can minimize deaths and property damage.2 According to our study, not evacuating one’s home before the storm, despite official recommendations, was the greatest risk factor for mortality during Typhoon Haiyan. In a study in the Philippines during Typhoon Bopha in 2013, a risk factor was no knowledge of the coming storm (MJ Zapanta, Department of Health, personal communication, 2013). Some villagers reported not vacating their residence due to anxiety about safeguarding their home and belongings. Other studies have also found that a desire to keep one’s belongings secure is a common reason for not evacuating.3 Evacuation orders for this kind of major storm should be compulsory, and warnings should emphasize that storms of this magnitude can cause death or injury.
Although it was reported that messages about the coming storm were received, it was also reported that the message to evacuate was not understood. The term “storm surge” was used to warn the public before Typhoon Haiyan, but many did not understand what this meant. Local officials tried to persuade people to evacuate through radio, television and personal roaming even during the arrival of the storm, but they kept using the words storm surge. Those who tried to explain it, described it as a “tsunami-like” effect of the sea. It would have been better if the term used was from the local dialect and a comprehensive description of what happens was provided.
Other studies have found flood-related deaths can be attributed to risk-taking behaviour during disasters.4 Leaving the house during the typhoon likely exposed people to dangerous winds and water. Swimming inability was a risk factor for increased mortality among females in the 2004 Indian Ocean Tsunami5 and after a tsunami in Indonesia.6 We did not identify swimming as an independent risk factor in our study; however, 68% of cases compared with 38% of controls, were not able to swim.
Other factors associated with death during disasters include age, gender, physical and mental health history, co-morbidities and activity and behaviour.7 In this study, we found older age to be a risk factor on bivariate analysis and this increased risk may have been due to underlying medical conditions aggravated during the stressful situation.6 Another study reported that older people experienced difficulties in receiving and understanding disaster warnings.8 This is consistent with the natural disaster trend where younger and older populations have increased risk of death.9 Being female was identified as a risk factor in the 2004 tsunami affecting Indonesia, India and Sri Lanka10 but not in this study. We hypothesize that since the study area was a fishing village, men were the predominant residents. However, the small sample size of this study may have limited our results.
This study has some limitations. First, we were limited in our control selection and therefore used a family member of the case. We found it difficult to obtain other controls because of the situation post-disaster and the displaced population. Second, the list of deaths was limited to those reported at the Village Affairs Office with possible data varying from the actual number of deaths; it is possible that some deaths had not been documented. Third, cause of death was based on what was written on the medical certificate, and it was not verified if a trauma occurred or if an underlying medical condition was present. Fourth, we only included four villages in the city with the most cases due to limited time, resources and poor accessibility. Therefore, these results may not be representative of other cities affected by the storm or other people who died in the storm. Fifth, using proxy respondents for cases may have affected the accuracy of information due to recall bias or lack of knowledge; however, there was no other way to obtain information on the cases. Despite these limitations, our findings have been verified elsewhere.7
In conclusion, this study identified leaving the house during the typhoon and not evacuating before Haiyan hit as risk factors associated with mortality in Tacloban City. This suggests that these types of deaths could be minimized by reducing these behavioural risks, by using warning messages understood by the population at risk. We recommend that the results from this study be used to develop more effective pre-disaster messages.
None declared.
This study was funded by the Philippine Department of Health.
We are grateful for the support of the Center for Health and Development-Eastern Visayas, Regional Epidemiology and Surveillance Unit of Region 8, local government of Tacloban City and the villagers of Tacloban City. We also thank the participants of the study and Mr Julius Velasquez who assisted in the investigation.
{kind=link}
{kind=link}