a Field Epidemiology Training Program, Epidemiology Bureau, Department of Health, Sta Cruz, Manila, Philippines.
b Department of Health, Sta Cruz, Manila, Philippines.
c Emerging Disease Surveillance and Response Unit, Division of Health Security and Emergencies, World Health Organization Regional Office for the Western Pacific, Manila, Philippines.
Correspondence to John Bobbie Roca (email: bobbie.roca@gmail.com).
To cite this article:
Roca JB et al. Fireworks-related injury surveillance in the Philippines: trends in 2010–2014. Western Pacific Surveillance and Response Journal, 2015, 6(4):1–6. doi:10.5365/wpsar.2015.6.1.014
Analysis of the annual fireworks-related injury surveillance data collected by the Philippines Department of Health (DOH) in 2010–2014 was conducted to describe the profile of such injuries in the Philippines.
Surveillance data were collected from DOH’s Online National Electronic Injury Surveillance System and analysed. A case was defined as any person who had sustained injury from fireworks in any form within the 16-day surveillance period (21 December to 5 January) and had presented to any of the 50 sentinel hospitals.
Of the 4649 cases, there were 4706 fireworks-related injuries involving 5076 anatomic sites in 2010–2014. A significant decrease of cases in 2014 was observed when compared with the previous study years (P = 0.02). The number of cases peaked at public holidays. Males (80%) were more commonly injured, and children aged 5 to 14 years were primarily affected (47%). Ignition of illegal fireworks accounted for half (50%) of the injuries; most injuries (68%) occurred in street settings. The majority of injuries (57%) were sustained by fireworks igniters. The most common anatomic injury sites were hands (44%), legs (21%) and eyes (14%). Illegal fireworks were related to 100% (4/4) of the deaths and 49% (105/214) of the cases who needed amputations.
Fireworks-related injuries declined significantly in 2014. Public awareness campaigns may have contributed to reducing the injury occurrences. As illegal fireworks accounted for all deaths and more than half of the amputations, law enforcement should be directed toward preventing importing, distributing and using illegal fireworks.
Fireworks usage at New Year’s festivities is a tradition in the Philippines. It is believed that fireworks attract good fortune and drive away evil spirits; however, fireworks also result in thousands of injuries every year.1
The establishment of annual fireworks-related injury surveillance in the Philippines started in 1991 involving three sentinel hospitals.2 In 2010, the online National Electronic Injury Surveillance System (ONEISS) was set up3 and hospital staff from 50 selected sentinel hospitals were trained to report fireworks-injury cases upon visit to emergency room.
Despite a national law that bans the private use of fireworks, there are still several fireworks-related injuries across 81 provinces in the country. The purpose of this study is to describe the profile of fireworks-related injuries in the Philippines using the ONEISS surveillance data from 2010 to 2014.
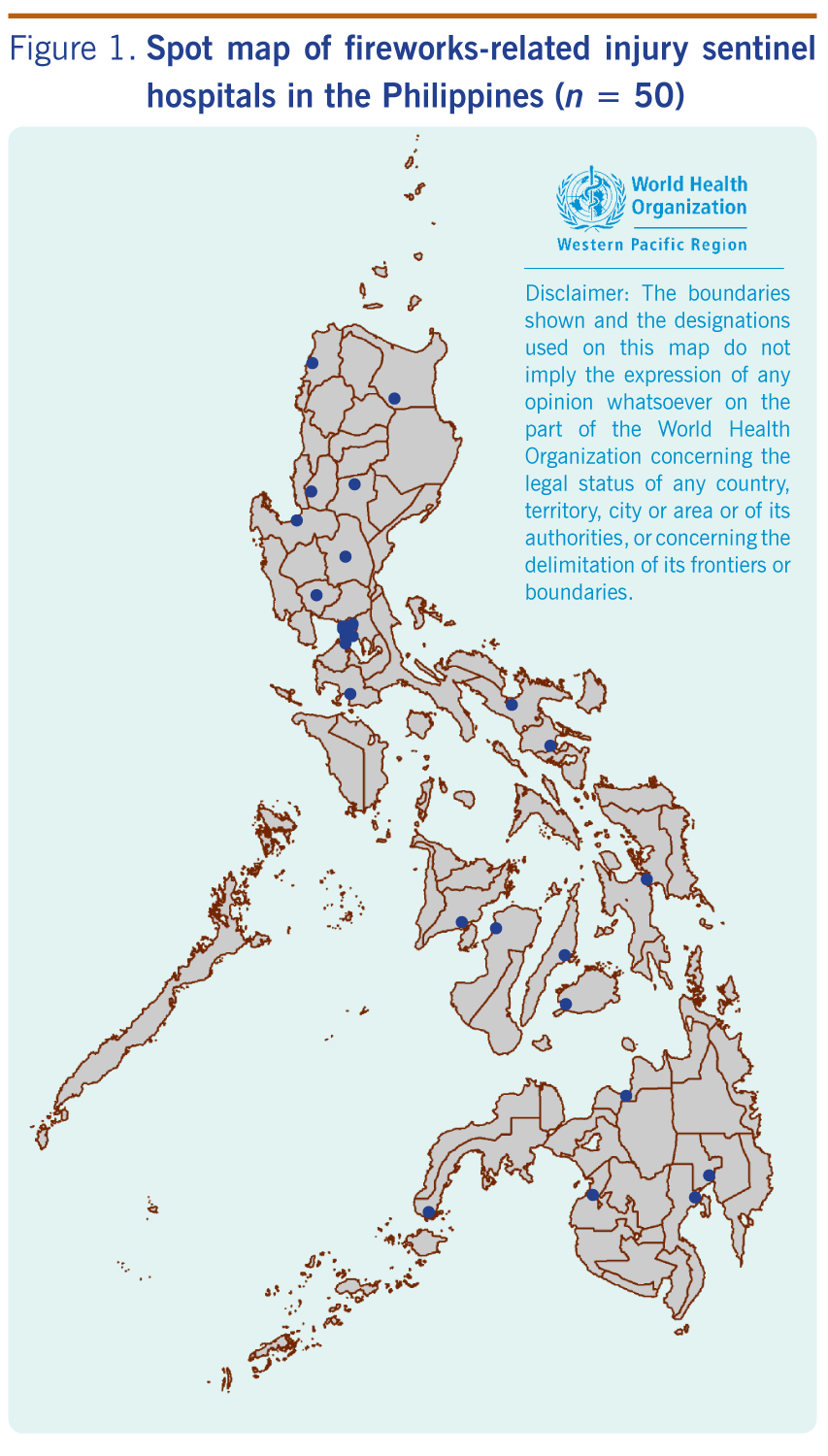
This is a descriptive study investigating fireworks-related injuries using ONEISS surveillance data from 50 sentinel hospitals in the Philippines between December 2010 and January 2015. This includes 33 hospitals of the Philippines Department of Health, four local government hospitals and 13 private hospitals (Figure 1).
For our study, a case of fireworks-related injury was defined as any person who sustained injury from fireworks in any form in the 16-day surveillance period (21 December to 5 January of the next year) and presented to any one of the sentinel hospitals. Recorded case data included demographics (e.g. age and sex); injured body part(s); location of incident; date of injury; and type of fireworks used.
Two-sided t-test with a significance level of 0.05 was used to compare the surveillance data trends over time. Notification rate by city/municipality was computed based on the 2010 population census data from the Philippine Statistics Authority.4 Analysis was performed using Stata/SE 12.0 for Windows (StataCorp LP, Lake Drive, TX, USA).
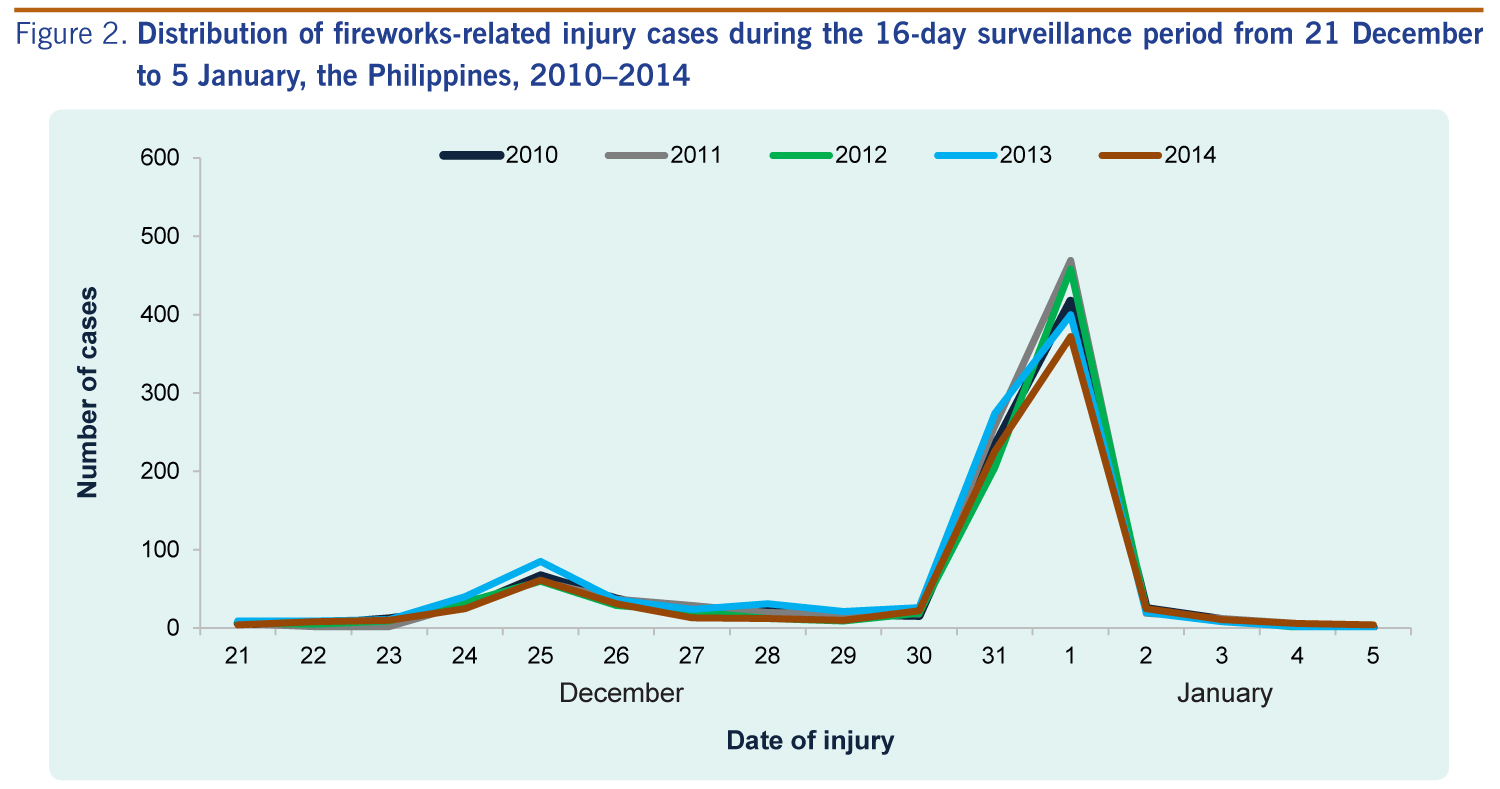
There were 4706 fireworks-related injuries in 4649 cases, involving 5076 anatomic sites in total. The number of fireworks-related injuries in 2014 (n = 840) was 12% less than the four-year mean (n = 953) of the period 2010–2013. This decrease was statistically significant (P = 0.02). A bi-modal peak in injury cases was shown during the 16-day annual surveillance periods. A small peak on 25 December and a sharp peak over a two-day period between 31 December and 1 January of the next year were observed. This trend was consistent for all five study years (Figure 2).

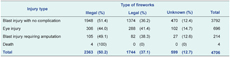
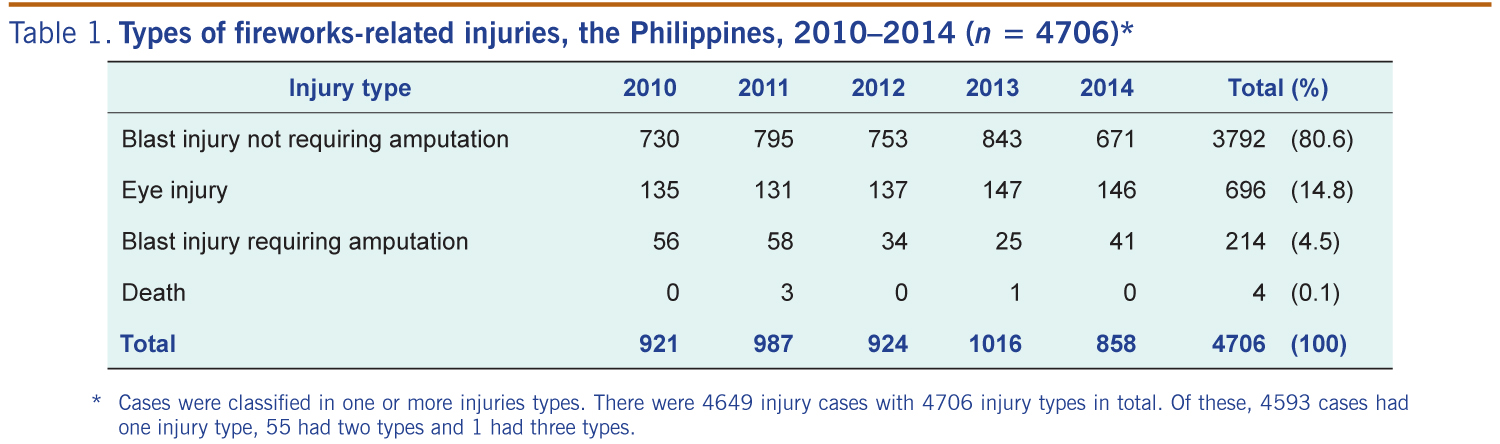
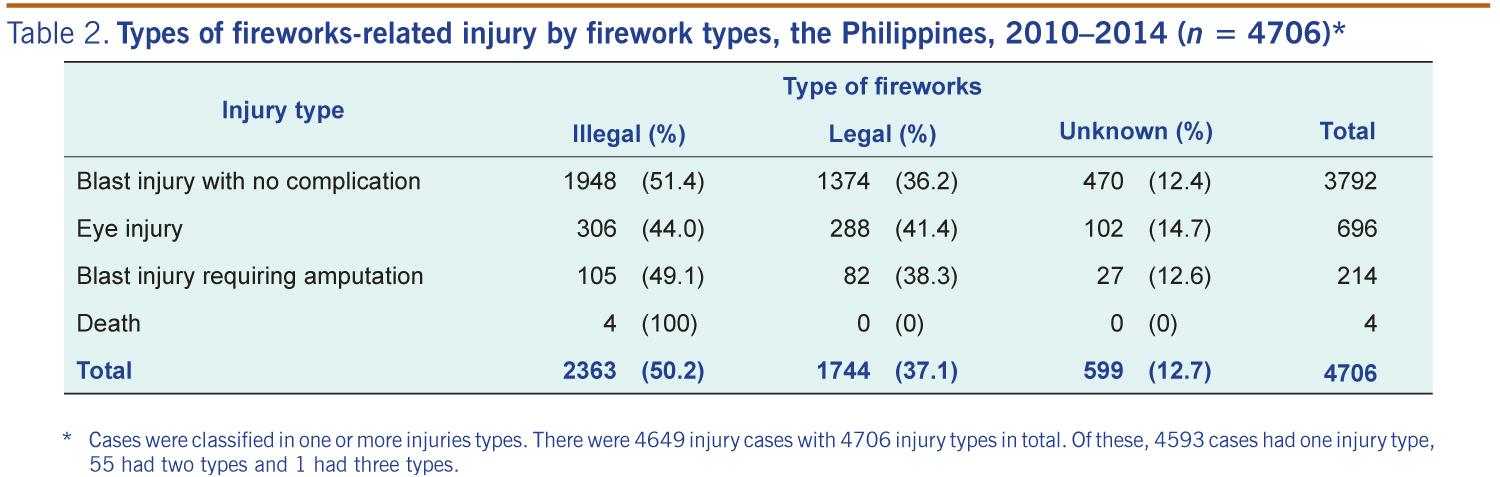
During the study period, blast injuries not requiring amputation accounted for 80.6% (3792/4706) of the total injuries. A total of 696 (13.7%) eye injuries were also reported. Amputation was required for 214 (4.5%) of the injuries. Four fireworks-related deaths were reported (case fatality ratio: 4/4649, 0.086%) (Table 1). Ignition of illegal fireworks accounted for 50.2% (2363/4706) of injuries. Most of the severe injuries (amputations and eye injuries) were due to illegal fireworks ignition. This included 100% (4/4) of deaths and 49.1% (105/214) of amputations. (Table 2).
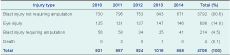
* Cases were classified in one or more injuries types. There were 4649 injury cases with 4706 injury types in total. Of these, 4593 cases had one injury type, 55 had two types and 1 had three types.
* Cases were classified in one or more injuries types. There were 4649 injury cases with 4706 injury types in total. Of these, 4593 cases had one injury type, 55 had two types and 1 had three types.
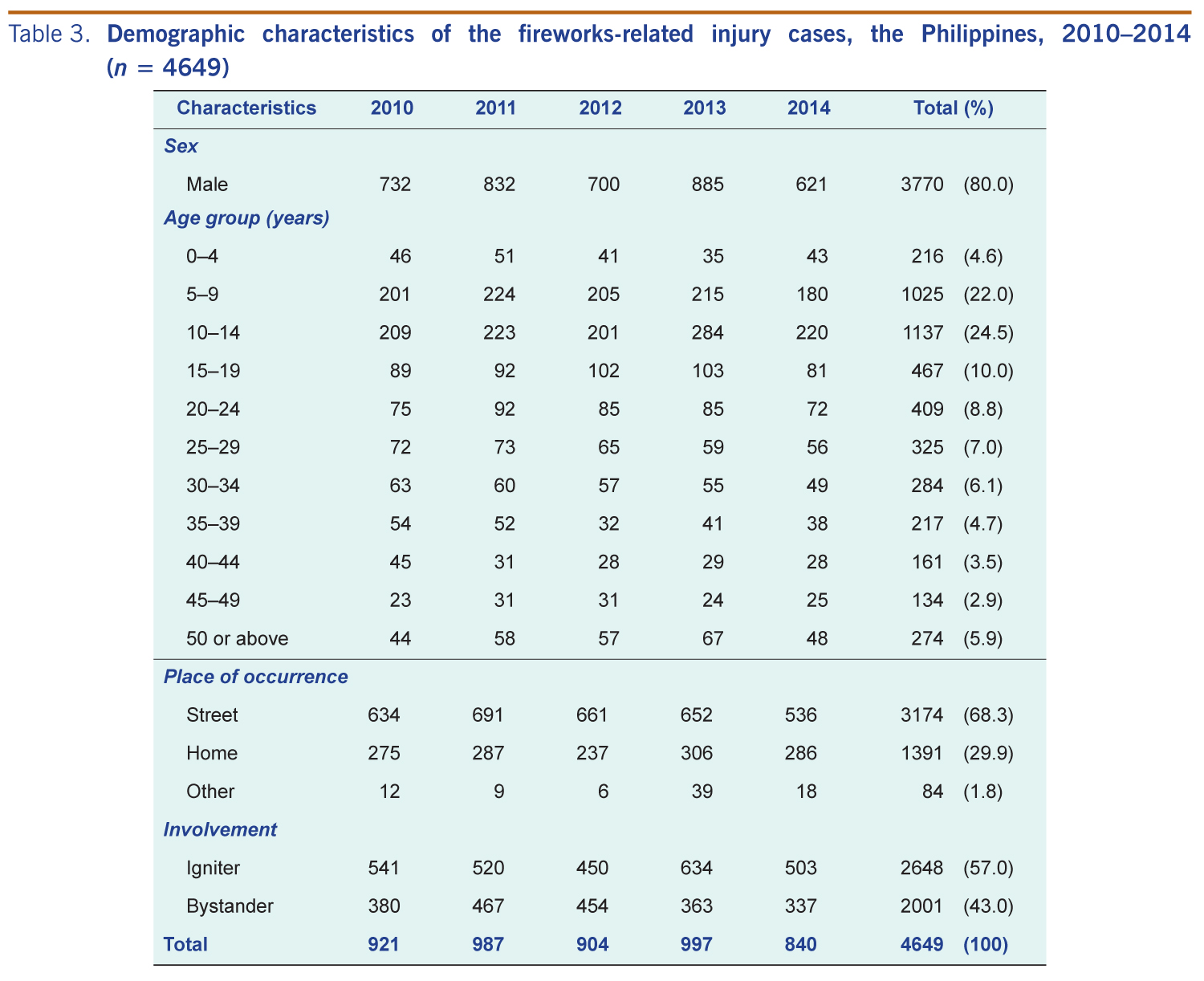
The number of fireworks-related injury cases was higher in males than females (80.0% in males versus 20.0% in females). Children aged 10–14 years old (24.5%) and 5–9 years old (22.0%) accounted for almost half of the cases (Table 3).
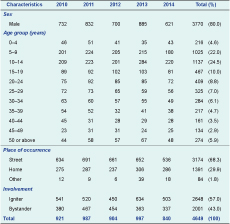
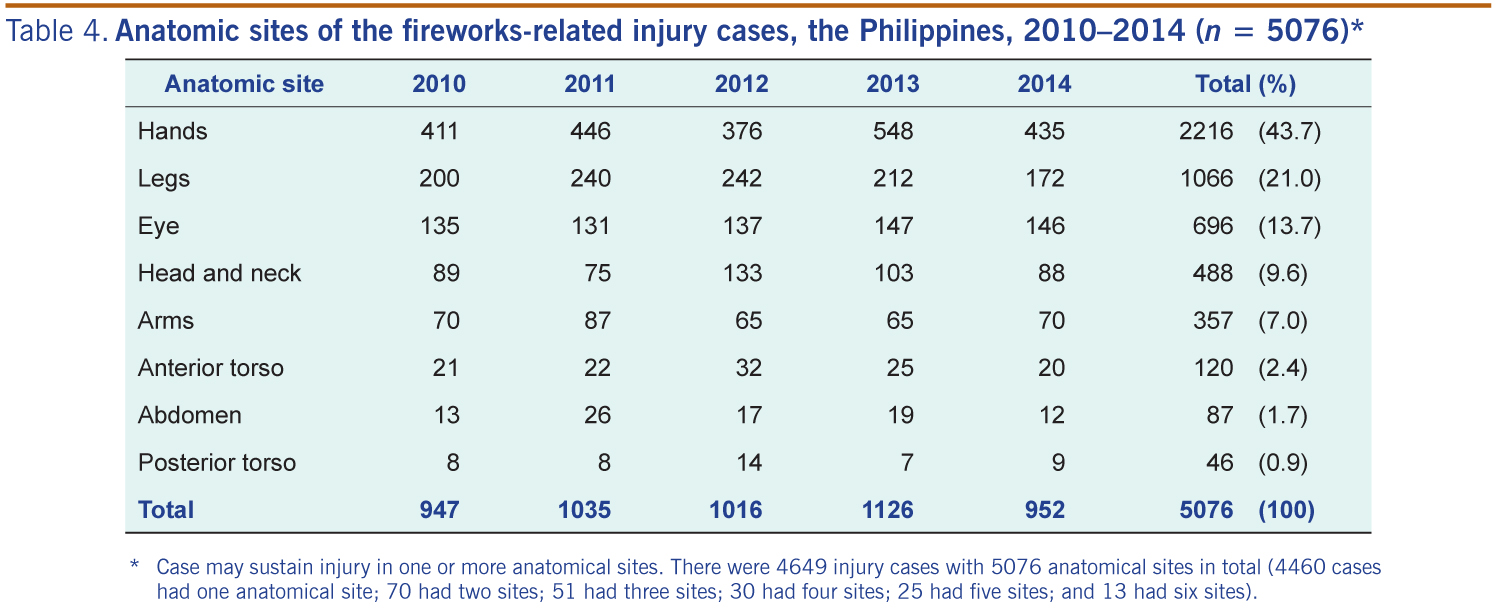
Most of the reported injuries (68.3%) occurred on streets and (57.0%) were sustained by fireworks igniters (Table 3). The most common anatomic sites of injury were hands (43.7%), legs (21.0%) and eyes (13.7%) (Table 4).
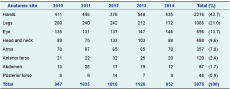
* Case may sustain injury in one or more anatomical sites. There were 4649 injury cases with 5076 anatomical sites in total (4460 cases had one anatomical site; 70 had two sites; 51 had three sites; 30 had four sites; 25 had five sites; and 13 had six sites).
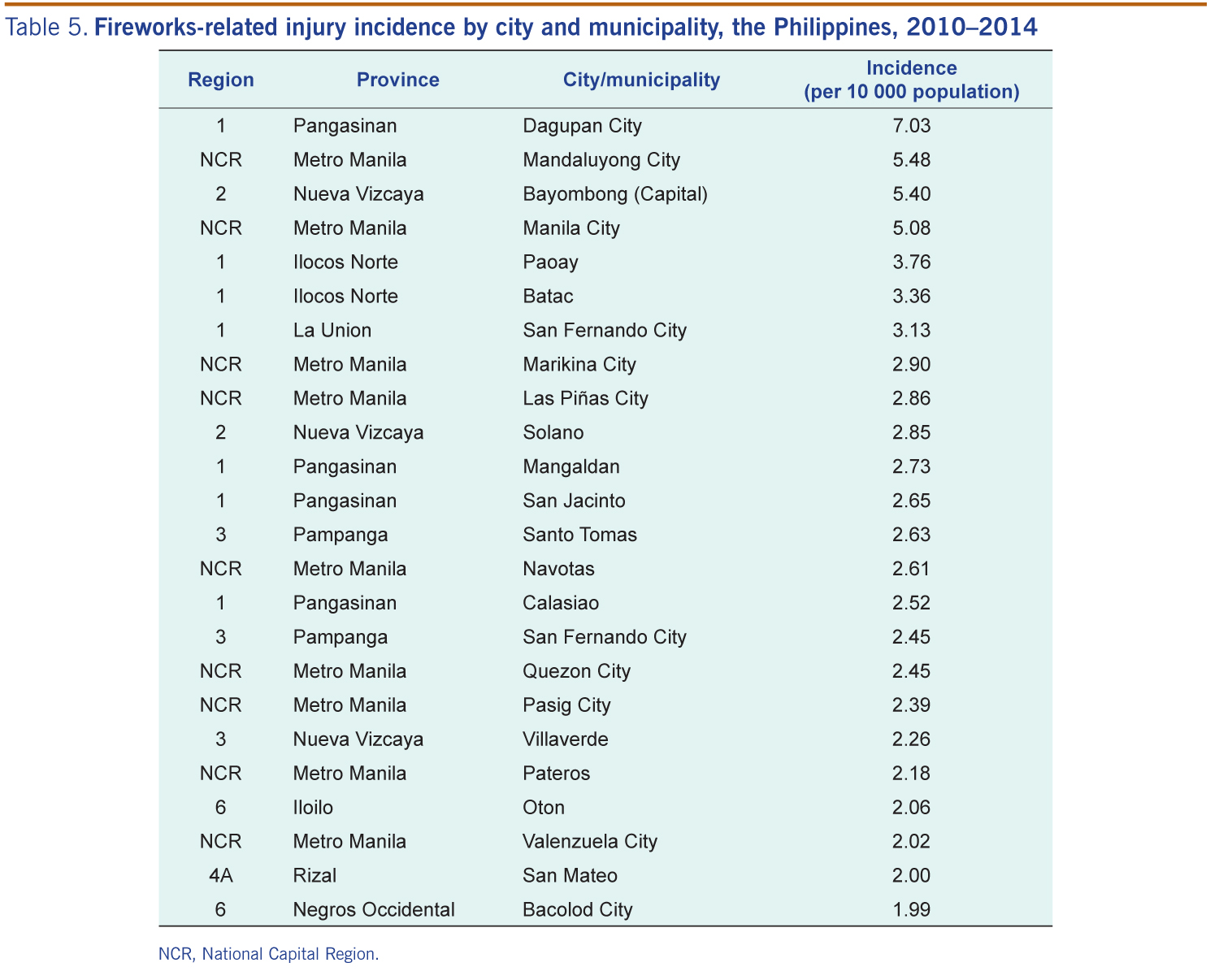
The notification rate of fireworks-related injuries was highest in the Dagupan City (7.03 per 10 000 individuals) in Pangasinan province, followed by Mandaluyong City (5.48 per 10 000 individuals) of Metro Manila and the municipality of Bayumbong (5.40 per 10 000 individuals) in Nueva Vizcaya province (Table 5).
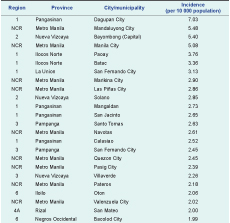
NCR, National Capital Region
The results showed a significant decrease in the overall number of fireworks-related injuries reported in 2014 compared with 2010–2013 in the Philippines. However, the number of more severe injuries that may lead to life-long disabilities5 did not decline (Table 1). This may be due to consistent usage of illegal fireworks that accounted for most of the severe injuries. The results also revealed that death from fireworks-related injury is a rare event in the Philippines. Risk of death by road traffic injury is much higher than that of fireworks in the Philippines.6 Fireworks injuries did not generally cause death in another study.7
The observed sharp peak of injury cases during the New Year’s holiday period were similar to that reported from the United States of America,7 where the celebration of Independence Day accounted for 95% of such injuries. A high percentage of injuries have also been reported elsewhere in association with national holidays such as Charshanbeh Soori in the Islamic Republic of Iran,5 Diwali Festival in India,8 Greek Orthodox Easter in Greece9 and New Year’s celebration in France.10
More cases were observed among males than females. This observation was similar to several previous studies.5,7,8,10,11 More injuries happened on the street than at home, similar to a study from the Islamic Republic of Iran.5 Also, our findings indicate that almost half of fireworks injuries occurs in the group aged 5–14 years, echoing findings in some previous studies.7,11 The number of injury cases was found to be higher in urban than rural areas. More cases in urban areas could be attributed to the higher population density, although we cannot find substantiating evidence in the current published literature. We found the most affected anatomical site of fireworks injuries was hands, which was consistent with previous studies,5,12 although one study showed that eyes followed by hands was most common.13
Despite legislation and awareness campaigns conducted by various government agencies in the Philippines, the main cause of firework-related death and severe injuries is illegal fireworks. This is similar to some previous studies.5,10 In a previous study in the United States of America, stricter law enforcement for restricting firework usage led to a sevenfold decrease in injury rates.13 Legislation enforcement to restrict the distribution and use of fireworks should be considered.
There were imitations in this study. Only hospitalized patients were captured by the sentinel surveillance system. Mild cases who did not require hospitalization were missed. Also, the sentinel sites cover only 24 out of 81 provinces. The notification rate estimates do not represent the national fireworks-related injury burden; they only reflect the situation within these hospital catchment areas. As this study focused more on the surveillance data analysis, evaluation for the surveillance system was not included. Future studies are needed to reveal the system’s performance.
The overall number of fireworks-related injuries declined in 2014. However, the number of severe injuries did not decline. Public awareness campaigns should target preventing the use of illegal fireworks since they account for the majority of fireworks-related deaths and severe injuries. Law enforcement efforts should be directed toward eliminating importing, distributing and use of illegal fireworks.
None declared.
None.
We appreciate the cooperation and support of the 50 sentinel hospitals together with the DOH-ONEISS team during the surveillance period. We also thank Ms Rowena Capistrano, Dr Althea De Guzman and Mr Ray Justin Ventura of the Philippine Field Epidemiology Training Program for collecting the data in 2010–2013.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}