
a Epidemiology Bureau, Department of Health, Sta Cruz, Manila, Philippines.
Correspondence to Flor D’ Lyn Gallardo (email: peachiegallardo@gmail.com).
To cite this article:
Gallardo FDL et al. An assessment of the case notification system 16 months after Typhoon Haiyan, Region 8, the Philippines. Western Pacific Surveillance and Response Journal, 2015, 6(Suppl 1):71–75. doi:10.5365/wpsar.2015.6.2.HYN_002
Introduction: The Philippines Department of Health uses the Philippine Integrated Disease Surveillance and Response (PIDSR) system to monitor 25 diseases and syndromes that have the potential to cause outbreaks. The focus of this system is to strengthen the capacity of local government units for early detection and response to outbreaks. After Typhoon Haiyan, routine disease surveillance activities were suspended at the Epidemiology and Surveillance Units (ESUs) at the city and provincial levels, as well as laboratory services; surveillance resumed as soon as local conditions allowed.
Method: We conducted an assessment of PIDSR in March 2015, 16 months post-Haiyan, in Region 8, the most heavily affected region. We used key informant interviews and a review of data from the system to assess the core surveillance and support functions.
Results: All ESUs reported they were performing all surveillance core functions, although laboratory confirmation needed to be strengthened at the regional reference laboratory. Access to working communication equipment also needed improvement as did timeliness and completeness of reporting.
Discussion: Assessment of surveillance activities, resources and quality should be conducted post-disaster. The strength and operations of the disease surveillance system usually requires support from the local, regional and national governments, especially if there are legal mandates and legislation that includes the system in disaster planning. Regular monitoring of the system is recommended to ensure stability, system development, increased outbreak detection and fewer morbidities and fatalities.
Disasters challenge the capacity of surveillance systems in a variety of ways, including damage to communication infrastructure, closure of health-care facilities, unavailability of surveillance staff, loss of laboratory facilities and distractions by other prioritized response activities. Re-establishing disease surveillance and response capacity is an important priority post-disaster.1 In a post-disaster setting, analysis of the role of routine health information systems has been limited.2
The Philippine Integrated Disease Surveillance and Response (PIDSR) system is a nationwide disease surveillance and response system.3 The system monitors 25 diseases and syndromes that have the potential to cause an outbreak and that warrant an immediate response. An outbreak is suspected when there is unexpected clustering of cases in an area within a period of time or the number of cases reported exceeds the expected threshold. The diseases reported to PIDSR are categorized as either Category 1 for immediate reporting (within 24 hours) or Category 2 for weekly reporting. Category 1 diseases are reported using case investigation forms that are disease specific and require immediate notification from city/hospital to province to regional level. Category 2 diseases are all reported on case report forms to a Regional Epidemiology and Surveillance Unit (RESU) every Friday. These forms are usually transmitted through email as metadata. If an Internet connection is not available, hard copies are sent through the mail or hand delivered to RESU for data entry. Feedback from RESU should be done every week, but often it is summarized and reported monthly.
Region 8, the region most affected by Haiyan, is composed of six provinces and eight cities with a population of 4 million. They adopted the PIDRS system in 2007 with Epidemiology and Surveillance Units (ESUs) at the provincial and city levels and sentinel hospitals serving as reporting units.4
In this study, we conducted an assessment of selected ESUs in Region 8 on core surveillance and support functions 16 months post-Haiyan. Using dengue as the representative disease, surveillance indicators such as timeliness and reporting rates in selected ESUs were also assessed for system performance.
A descriptive study using key informant interviews and records review was conducted to gather information on PIDSR operations 16 months after Typhoon Haiyan. The study focused on the support functions of the system – health workforce, communication equipment, access to Internet, availability of PIDSR forms and laboratory logistics. The six core surveillance functions based on WHO guidelines were assessed: case detection, case registration, reporting, confirmation, analysis and feedback.5 Timeliness and reporting rate were also assessed using data obtained from January to February 2015 as per the Centers for Disease Control and Prevention guidelines for evaluating public health surveillance systems.6
Seven ESUs and two sentinel hospitals (9 of 14 [64%]) from Region 8 were selected for this assessment. The ESUs comprised the RESU, four Provincial ESUs (PESUs) and two City ESUs (CESUs). Face-to-face interviews using a guided questionnaire were conducted among surveillance staff, the head of the RESU, the chief of hospital (n = 1) and the director of PESUs (n = 3). Interviewees were asked to comment on the present status of PIDSR support functions.
PIDSR metadata were obtained from six reporting units to determine case detection and the timeliness of data entry post-Haiyan. These were PESUs from Biliran, Eastern Samar, Western Samar and Leyte and disease reporting units from the Eastern Visayas Regional Medical Center (EVRMC) and Leyte Provincial Hospital. Dengue notification reports from 1 January to 28 February 2015 were obtained. Dengue was chosen as the representative disease as vector-borne diseases remain a perennial problem in the area, and cases were expected to increase after Haiyan.7 Timeliness was defined as the number of weekly reports received by the RESU from each PESU and CESU divided by eight (the total number of expected reports for the eight-week period of study). The reporting rate was defined as the number of dengue files received at RESU from the ESUs divided by the total number of disease reporting units that regularly submit weekly reports. The target for both surveillance functional indicators was above 80%.
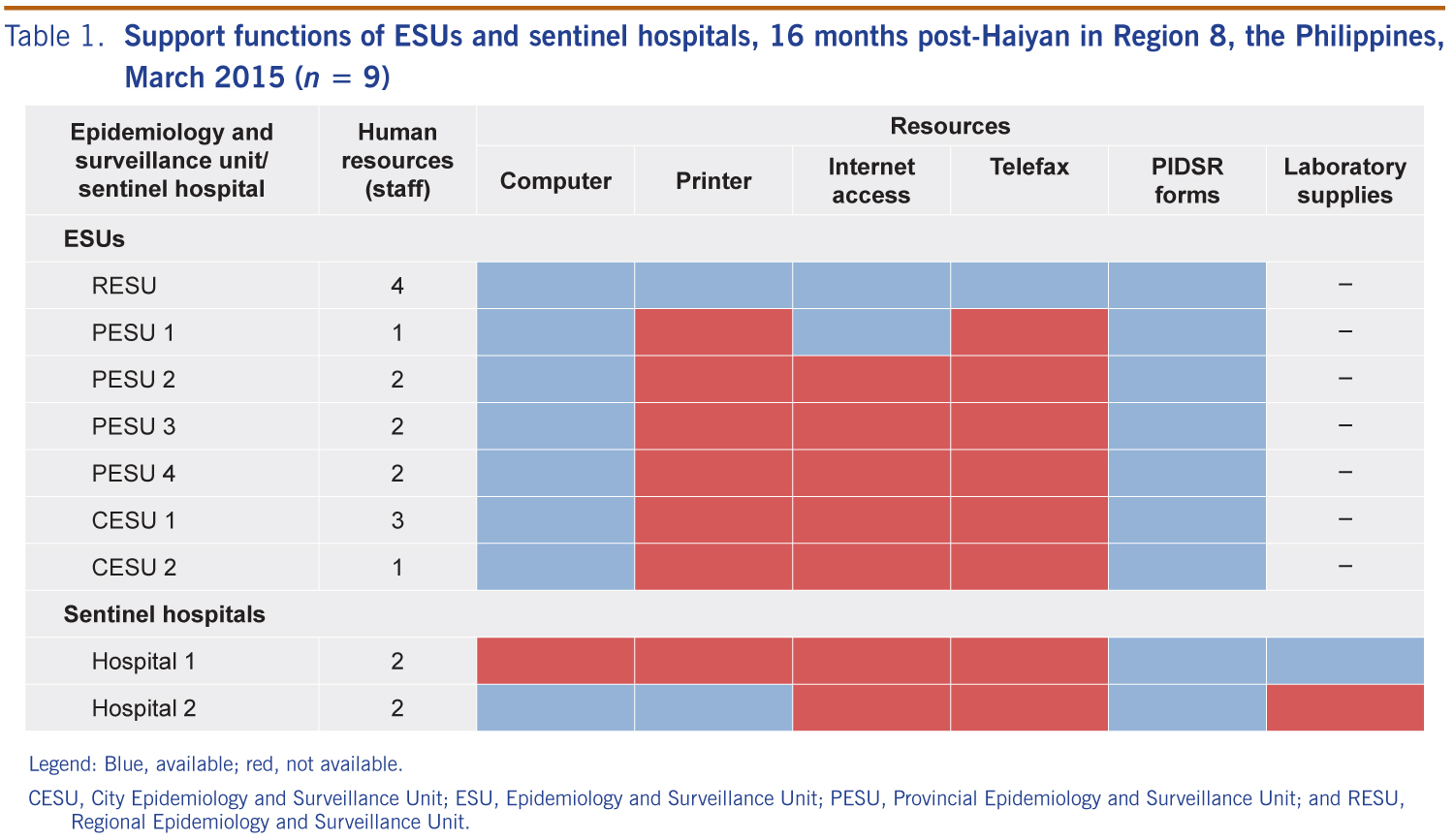
At the time of the study, 16 months post-Hiayan, all seven ESUs and the two hospitals had diseases surveillance officers and most (8/9, 89%) had adequate information technology equipment for data management. However, seven (78%) did not have printers for report generation, seven (78%) reported having unstable and limited Internet access and eight (89%) reported that sending and receiving surveillance reports was challenging. All ESUs and hospitals had PIDSR forms available (Table 1).
Legend: Blue, available; red, not available.
CESU, City Epidemiology and Surveillance Unit; ESU, Epidemiology and Surveillance Unit; PESU, Provincial Epidemiology and Surveillance Unit; and RESU, Regional Epidemiology and Surveillance Unit.
Of the two hospital laboratories, one could do bacterial culture and hepatitis A IgM by ELISA detection (Table 1).
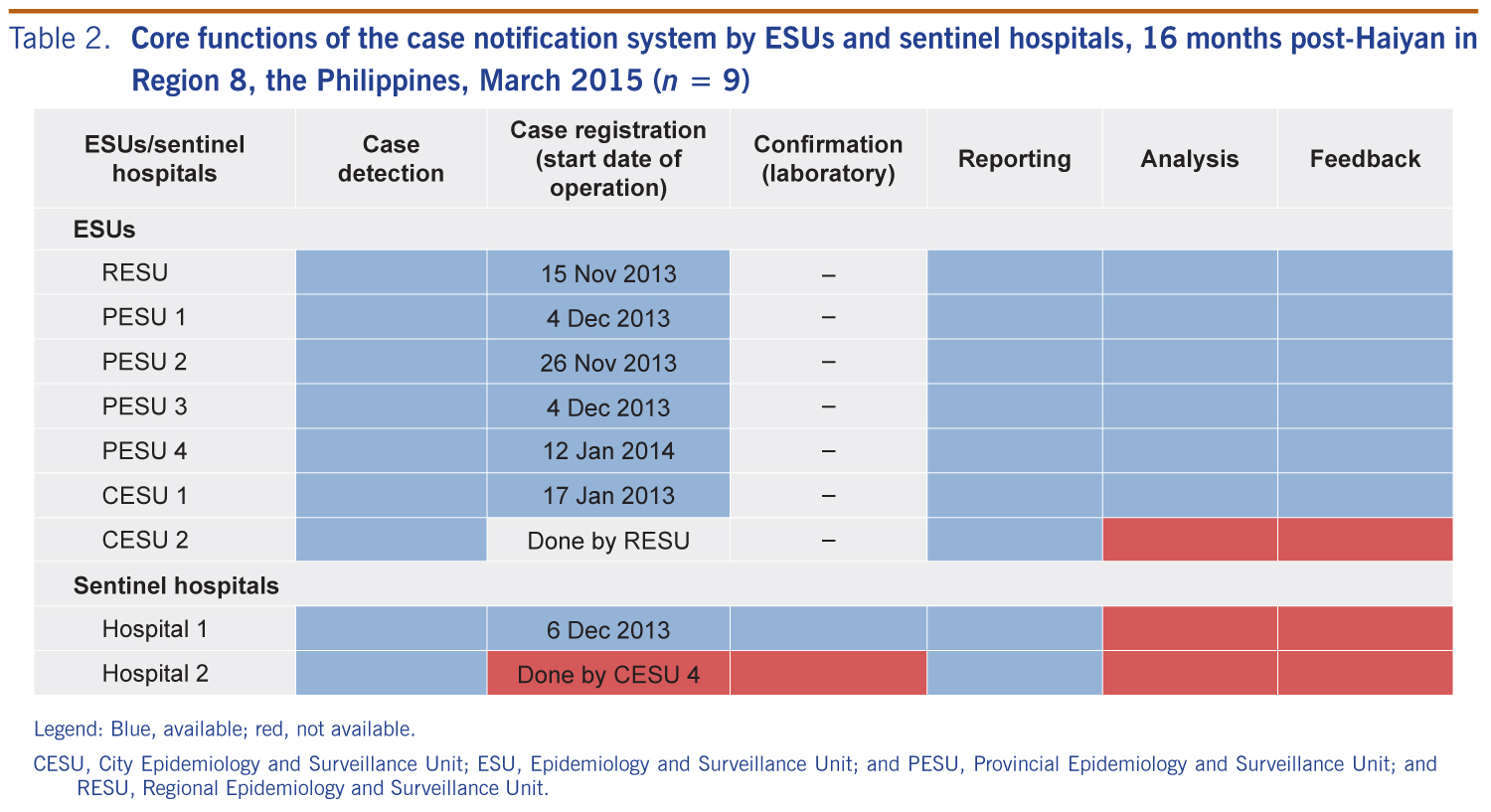
All reporting units were able to conduct case detection activities. One CESU and one hospital reporting unit were unable to do data entry from case forms due to other health service delivery tasks and rapid changes of health services delivery roles. Data entry was done by RESU staff for these reporting units.
Data transmission from the PESUs to the RESU varied 16 months post-Haiyan: case report forms from one PESU were hand-delivered, two were sent by email and one actively collected by RESU staff. The earliest data entry post-Haiyan was on 15 November 2013 at the RESU. This was seven days post-disaster; case registration resumed after one to 10 weeks at the provincial and city levels (Table 2).

Legend: Blue, available; red, not available.
CESU, City Epidemiology and Surveillance Unit; ESU, Epidemiology and Surveillance Unit; and PESU, Provincial Epidemiology and Surveillance Unit; and RESU, Regional Epidemiology and Surveillance Unit.
RESUs did the routine analysis and dissemination of data to stakeholders through written or verbal feedback. No outbreaks were detected in these analyses and feedback.
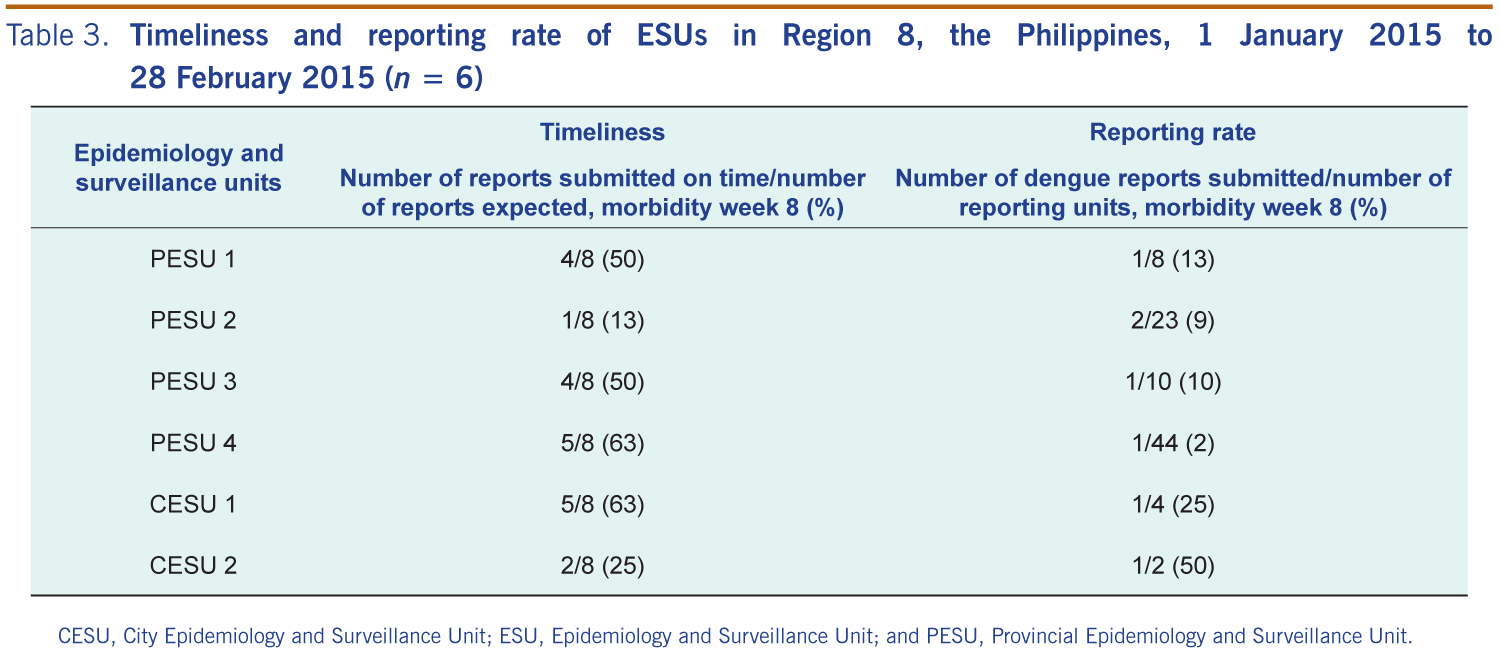
For the eight-week reporting period in January and February 2015, none of the four PESUs or two CESUs met the target of 80% for timeliness and reporting for dengue notifications; timeliness ranged from 13% to 63% and reporting from 2% to 50% (Table 3).

CESU, City Epidemiology and Surveillance Unit; ESU, Epidemiology and Surveillance Unit; and PESU, Provincial Epidemiology and Surveillance Unit.
This study shows that the re-establishment of PIDSR in Region 8 was slow after Typhoon Haiyan. Reasons for this included the massive destruction to health infrastructures, loss of human lives and resources, lack of electricity, impassable roads, non-functional telecommunication systems and severely damaged data management equipment. Also, as in the Great Japan Earthquake,8 many health workers were victims themselves and were unable to deliver health services. Directly after Haiyan, there were many difficulties in collecting vital health data and data for disease surveillance, thus monitoring disease trends became impossible.
The ESUs reported resuming surveillance activities one to 10 weeks post-Haiyan. Although this assessment showed that surveillance core functions were routinely being conducted, there was poor quality on timeliness and reporting rates observed in the surveillance reports submitted by ESUs. Reporting rates for support core functions were also variable due to lack of equipment for report generation. Better telecommunication and Internet access would have resulted in improved report transmission. While case detection, case registration and reporting of disease surveillance activities were reported as being stable, the analysis and feedback component of the surveillance system needed to be strengthened.
There also were no outbreaks detected through PIDSR in the time between Haiyan and this study. As PIDSR is an indicator-based surveillance system, the detection of outbreaks requires stable reporting and monitoring of the number of cases against a threshold. Thresholds are indicators of when the level of disease occurrence has been reached as an early warning for epidemics (alert threshold), and when the level of disease occurrence is above the expected range (outbreak threshold).9 As there was irregular reporting in the indicator-based surveillance system after Haiyan, it was not surprising that no outbreaks were detected. There were outbreaks of measles, dengue and acute gastroenteritis reported through the Philippines event-based surveillance and response system post-Haiyan, suggesting that event-based surveillance might be more useful in the post-disaster setting.
Laboratory capacity was also limited in the study area 16 months post-Haiyan, with only one hospital that could perform laboratory confirmation testing (e.g. bacterial culture). Most samples were sent to the Research Institute for Tropical Medicine in Manila for testing. Additional health facilities that can conduct laboratory procedures or mobile laboratories would be useful for future response efforts as adequate surveillance relies on laboratory testing being available. Enhancing laboratory capacity for disasters can be achieved through training more laboratory personnel and having surge capacity when disasters occur.10
This study had limitations. As it purposely selected those ESUs most affected by Haiyan, the results are biased towards a non-functioning surveillance system and may not be representative of all cities and hospitals. Also, surveillance functional indicators such as timeliness and reporting rate data pre-disaster were unavailable and therefore unable to be compared to our results. Other limitations are that some of the results rely on self-reporting which may lead to bias, that a full evaluation of all components of the surveillance system was not included and that the sample size was small (only two CESUs).
In this post-Haiyan assessment, the re-establishment of PIDSR in Region 8 was slow and hampered by the impact of Haiyan. Communications support was not optimal; staff, when available, had other competing tasks; laboratory testing was done in one hospital and the subnational reference laboratory and the timeliness of reporting and reporting rates for dengue were low. Although case detection activities were being conducted in all reporting units, some data entry was being referred to RESU staff.
The operation of indicator-based surveillance systems, such as PIDSR, greatly depends on the support of the local, regional and national governments coupled with legal mandates and legislations. Based on this study, we recommend regular monitoring and evaluation of PIDSR to determine specific surveillance activity gaps and to review surveillance functionality. This should occur routinely at the regional, provincial and city levels and also post-disaster to assess how the system has recovered.
None declared.
None.
We are grateful for the Epidemiology Bureau of the Department of Health (DOH) for allowing us to conduct this study. The authors would also like to thank the Regional Ofice of the DOH in Region 8 particularly Mr Boyd Roderick Cerro, disease surveillance officers, PIDSR coordinators and ESU heads of Eastern Visayas for providing the information and data. We would also like to thank Dr Michael O’Reilly and Mr John Bobbie Roca for making this study possible.
{kind=link}
{kind=link}
{kind=link}