a Department of Emergency Response, Wenzhou Center for Disease Control and Prevention, Wenzhou 325000, People’s Republic of China.
b Department of Preventive Medicine, Wenzhou Medical University, Wenzhou 325000, People’s Republic of China.
c Department of Medical Records, The Second Affiliated Hospital of Wenzhou Medical University, Wenzhou 325000, People’s Republic of China.
Correspondence to Zhou Zu-Mu (email: zhouzumu@126.com).
To cite this article:
Zhou ZM et al. Risk factors of neonatal tentanus in Wenzhou, China: a case-control study. Western Pacific Surveillance and Response Journal, 2015, 6(3). doi:10.5365/wpsar.2015.6.1.020
Introduction: Neonatal tetanus is a major cause of neonatal mortality in many developing countries and remains a major public health problem. This study aimed to determine risk factors associated with neonatal tetanus in Wenzhou, China.
Methodology: Medical records of neonatal tetanus cases from 17 hospitals over a 13-year period (2000–2012) were reviewed for potential risk factors. Controls were selected from neonates with diseases other than tetanus who were admitted to the same facility during the same period. The potential risk factors of the neonatal tetanus group were compared with the control group using univariate analysis and an unconditional logistic regression model.
Results: A total of 246 neonates with tetanus and 257 controls were included in this study. Univariate analysis showed that the odds of having untrained birth attendants, home delivery, an unsterile method of delivery and being a migrant to Wenzhou were significantly different between the two groups (P < 0.001). Logistic regression analysis revealed that having an untrained birth attendant, home delivery and an unsterile method of delivery were significantly higher in the tetanus group than the control group (odds ratio: 1371.0; 95% confidence interval: 206.0, 9123.5).
Conclusion: This study identified that the main risks of neonatal tetanus in cases from Wenzhou were having an untrained birth attendant, home delivery and an unsterile method of delivery. Preventive measures directed to these risk factors may reduce the occurrence of neonatal tetanus in the studied area.
Tetanus is acquired through exposure to the spores of the bacterium Clostridium tetani, which is universally present in the environment. The organism usually prevails in dirty wounds or for neonatal tetanus, in the umbilicus following unsterile delivery.1,2 Neonatal tetanus is a major cause of neonatal mortality in many developing countries and remains a major public health problem.1,3,4 The World Health Organization (WHO) estimates that 58 000 newborn infants died from tetanus in 2010.5 Although this estimate is a 93% reduction in deaths from the late 1980s,5 the disease continues to occur in developing countries as well as in certain economically disadvantaged regions of China.6,7 The deaths predominantly occur in low- and middle-income countries, mostly in Asia and Africa.8,9
The incidence and mortality of neonatal tetanus differ between regions and countries and between urban and rural areas within countries.8,10 The incidence of neonatal tetanus in China has dramatically decreased from 0.2 cases per 100 000 population in 2005 to 0.05 cases per 100 000 population in 2012.11
Neonatal tetanus has many determinants, and many international and national efforts are aimed at eliminating neonatal tetanus.5,7 In some resource-poor settings of the world, unsterile deliveries and poor post-natal hygiene compound the risk of neonatal tetanus.12–15 The cultural diversity of childbirth practices and cord management, untrained birth attendants, uneducated parents, poor antenatal care and lack of immunization against tetanus have also been associated with the disease.4,5,16,17 Furthermore, seasonality, geographical location, climate, prevalence of C. tetani and a rural agricultural population are also related to the incidence of neonatal tetanus.18
Wenzhou is a prefecture-level city in south-eastern Zhejiang province, China and comprises three municipal districts and eight counties with a total land area of 11 784 km2. The population of Wenzhou area is 9 122 102, which includes 2 842 241 migrants from other areas within China; these migrants account for 31.2% of the total population.19
In the wake of urbanization and industrialization in China, domestic migration will be increasingly frequent. There were 230 million domestic migrants in China in 2011, accounting for 17% of the total population.20 The migrant population ratio in Wenzhou is higher than for all of China, and 87.7% of migrants in Wenzhou are people from the economically disadvantaged provinces of Guizhou and Yunnan.19 In Guizhou province, the number of cases of neonatal tetanus decreased from 276 in 2005 to 29 in 2012 and in Yunnan province from 189 cases in 2005 to 64 in 2012. These neonatal tetanus cases represent the highest number of cases at the provincial level in China.11
As the number of domestic migrants has been increasing in Wenzhou in recent years and the risk factors for neonatal tetanus are not well known in this area, this study aimed to determine the risk factors for neonatal tetanus in Wenzhou, China.
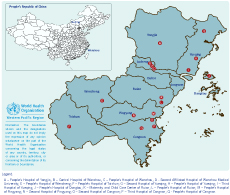
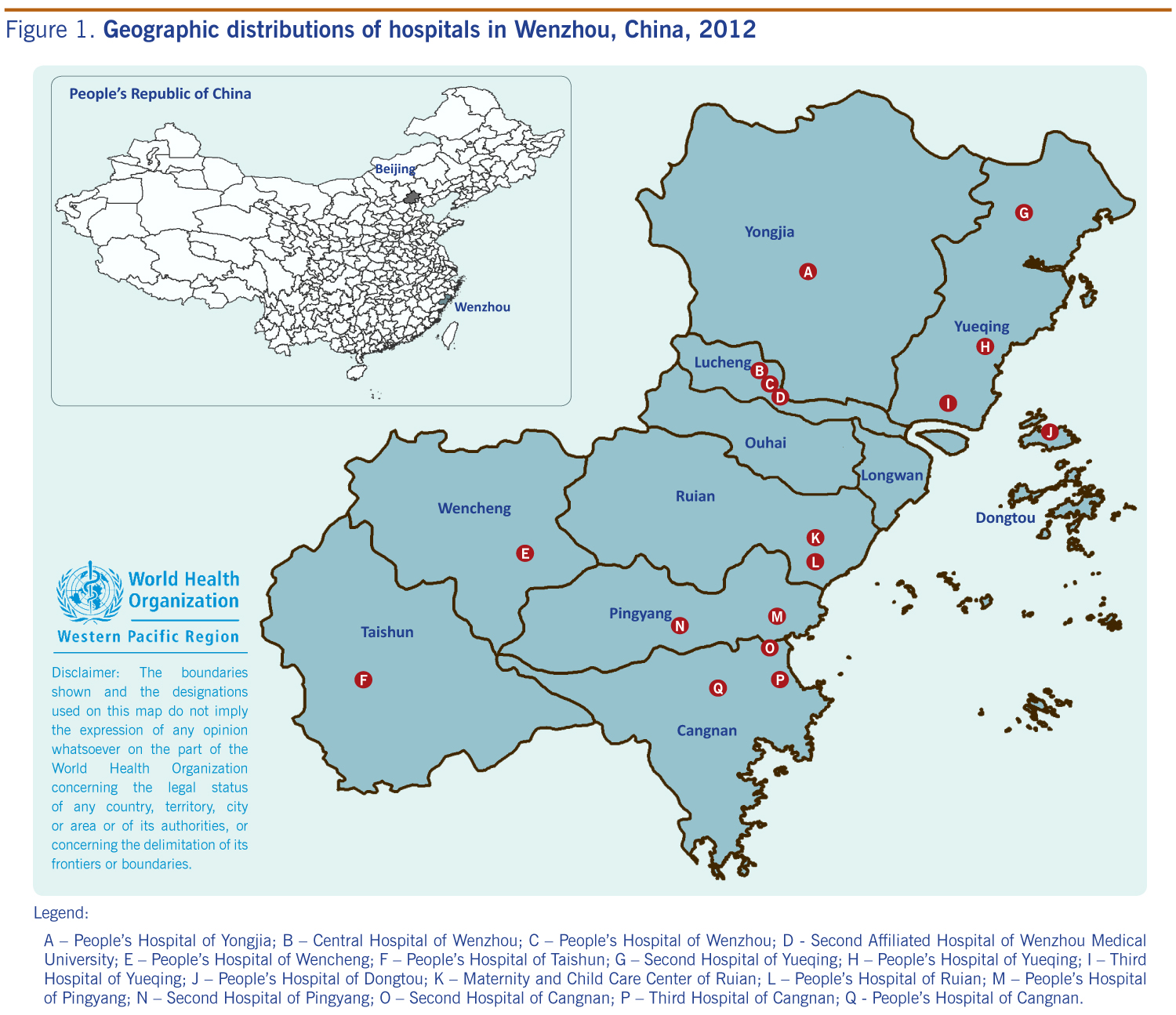
A case-control study was conducted in 17 of 24 hospitals with paediatric wards in Wenzhou, China (Figure 1). These hospitals are located in 11 counties and districts of Wenzhou. Neonatal tetanus cases diagnosed between 1 January 2000 and 31 December 2012 were identified from the medical records departments; all diagnoses were made and recorded by clinical doctors from the hospitals. The cases were verified against neonatal tetanus cases reported in the national disease surveillance information system for the same time period.
Legend:
A – People’s Hospital of Yongjia; B – Central Hospital of Wenzhou; C – People’s Hospital of Wenzhou; D - Second Affiliated Hospital of Wenzhou Medical University; E – People’s Hospital of Wencheng; F – People’s Hospital of Taishun; G – Second Hospital of Yueqing;
H – People’s Hospital of Yueqing; I – Third Hospital of Yueqing; J – People’s Hospital of Dongtou; K – Maternity and Child Care Center of Ruian; L – People’s Hospital of Ruian; M – People’s Hospital of Pingyang; N – Second Hospital of Pingyang; O – Second Hospital of Cangnan; P – Third Hospital of Cangnan; Q - People’s Hospital of Cangnan.
The WHO case definition for neonatal tetanus was used: a confirmed case was defined as any neonate with the normal ability to suck and cry during the first two days of life, and who between three and 28 days of age could not suck normally, or became stiff or had convulsions or both.21 Cases not meeting this case definition were excluded.
Controls were selected from the same medical records departments. Using either the patient registry or computer records, neonates with other diseases (such as pneumonia, congenital heart disease, gastroenteritis, neonatal jaundice, etc.) admitted to the same facility during the same time period as the cases were selected as controls.
Information about cases and controls was collected from medical records, and data on risk factors for neonatal tetanus were entered into an Excel database designed for the study. The data included age at presentation, gender, maternal age and parity, gestational age, type of inhabitants (local inhabitants, migrants from other areas in Zhejiang province or migrants from other provinces), method of delivery (sterile or unsterile), location of delivery and whether the birth attendants were trained or untrained. An unsterile delivery was defined as delivering a baby at home by untrained attendants or cord managed by a non-health care provider. Births in a hospital, health centre or clinic were categorized as births at a health facility. As three of the variables (method of delivery, place of delivery and training of birth attendants) were correlated, a new variable for overall delivery was created where category 1 was birth at a health facility with a trained attendant in a sterile environment; category 2 was either of the following – home birth, or untrained birth attendant or unsterile birth; and category 3 was a home birth with an untrained attendant in an unsterile environment. The data were entered into the database twice, and any discrepancies corrected.
Potential risk factors (including method of delivery, training of birth attendants, place of delivery, type of inhabitants, parity of the mother, neonatal gender, maternal age and neonatal weight) were compared between the cases and controls using chi-square tests or categorical data and Student t test for continuous data, i.e. maternal age variable. Variables significant (P < 0.05) in univariate analysis were included in an unconditional logistic regression model. For all analyses, a significance level of 5% and 95% confidence interval (CI) was considered. Statistical analysis was conducted with SPSS Statistics 14.0 software (IBM, Shanghai, China).
The Wenzhou Center for Disease Control and Prevention ethical committee approved this study (No 201301).
A total of 246 neonatal tetanus cases and 257 controls were included. Maternal age (the mean ± standard deviation among the case group was 27.2 ± 4.8 years compared with 27.4 ± 4.8 years for the control group, and this was not significantly different (P = 0.58). The gender of the neonates was also not significantly different between the two groups (P = 0.14).
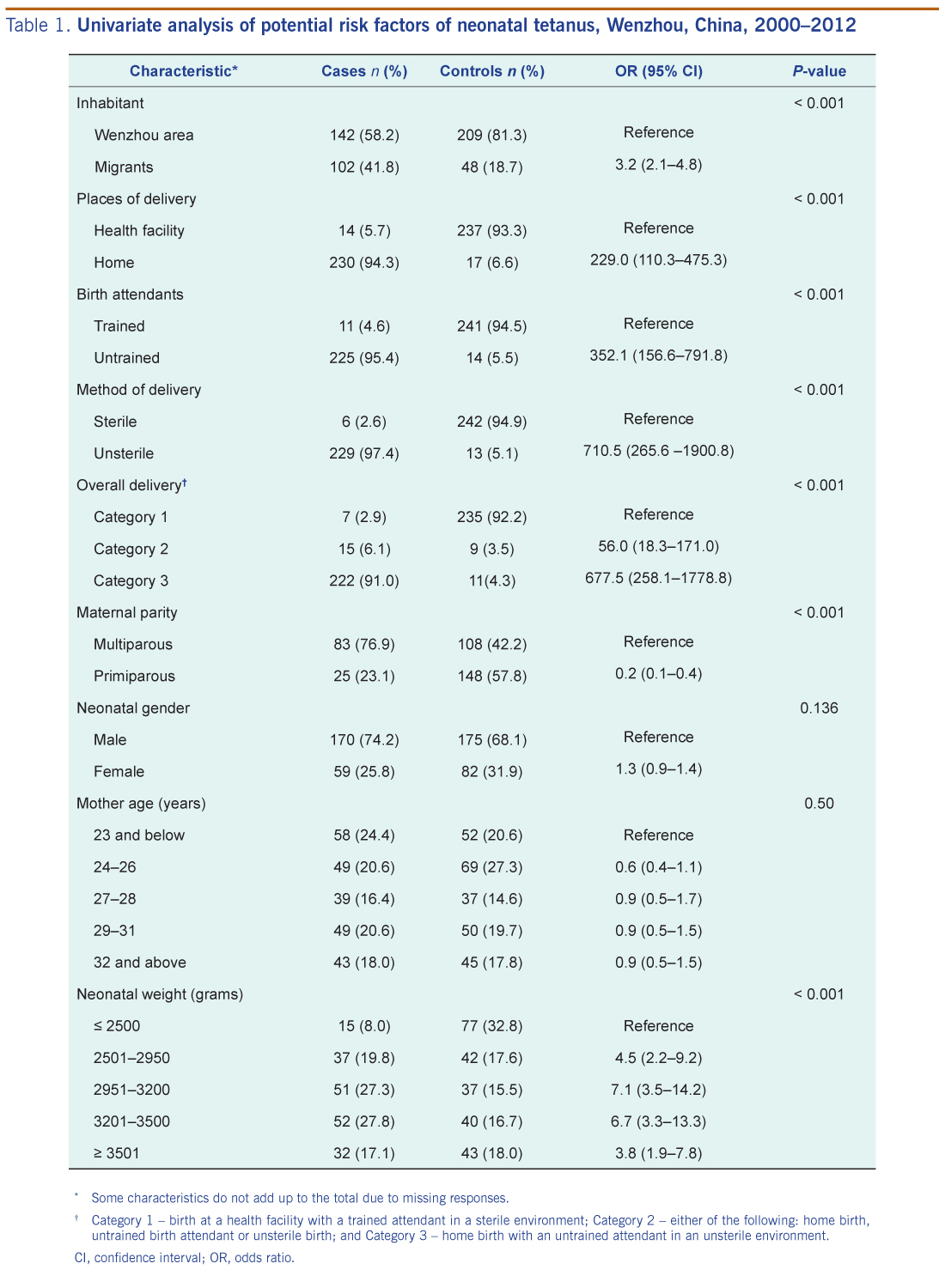
Factors significant at the univariate level included being a migrant, having a home birth, untrained birth attendants, unsterile deliveries, increasing neonatal weight and having a multiparous mother (Table 1). For overall delivery, having one of three factors (a home birth, untrained birth attendants or unsterile delivery) had a high risk of neonatal tetanus (odds ratio [OR]: 56.0; 95% CI: 18.3–171.0), while having all three factors had a much higher risk of neonatal tetanus (OR: 677.5; 95% CI: 258.1–1778.8) (Table 1). Stratified analysis showed that the influence of neonatal gender, maternal parity, type of inhabitant, maternal age and neonatal weight on the three risk factors (home deliveries, untrained birth attendants, unsterile deliveries) was not significant.
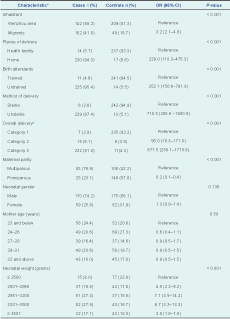
* Some characteristics do not add up to the total due to missing responses.
† Category 1 – birth at a health facility with a trained attendant in a sterile environment; Category 2 – either of the following: home birth, untrained birth attendant or unsterile birth; and Category 3 – home birth with an untrained attendant in an unsterile environment.
CI, confidence interval; OR, odds ratio.
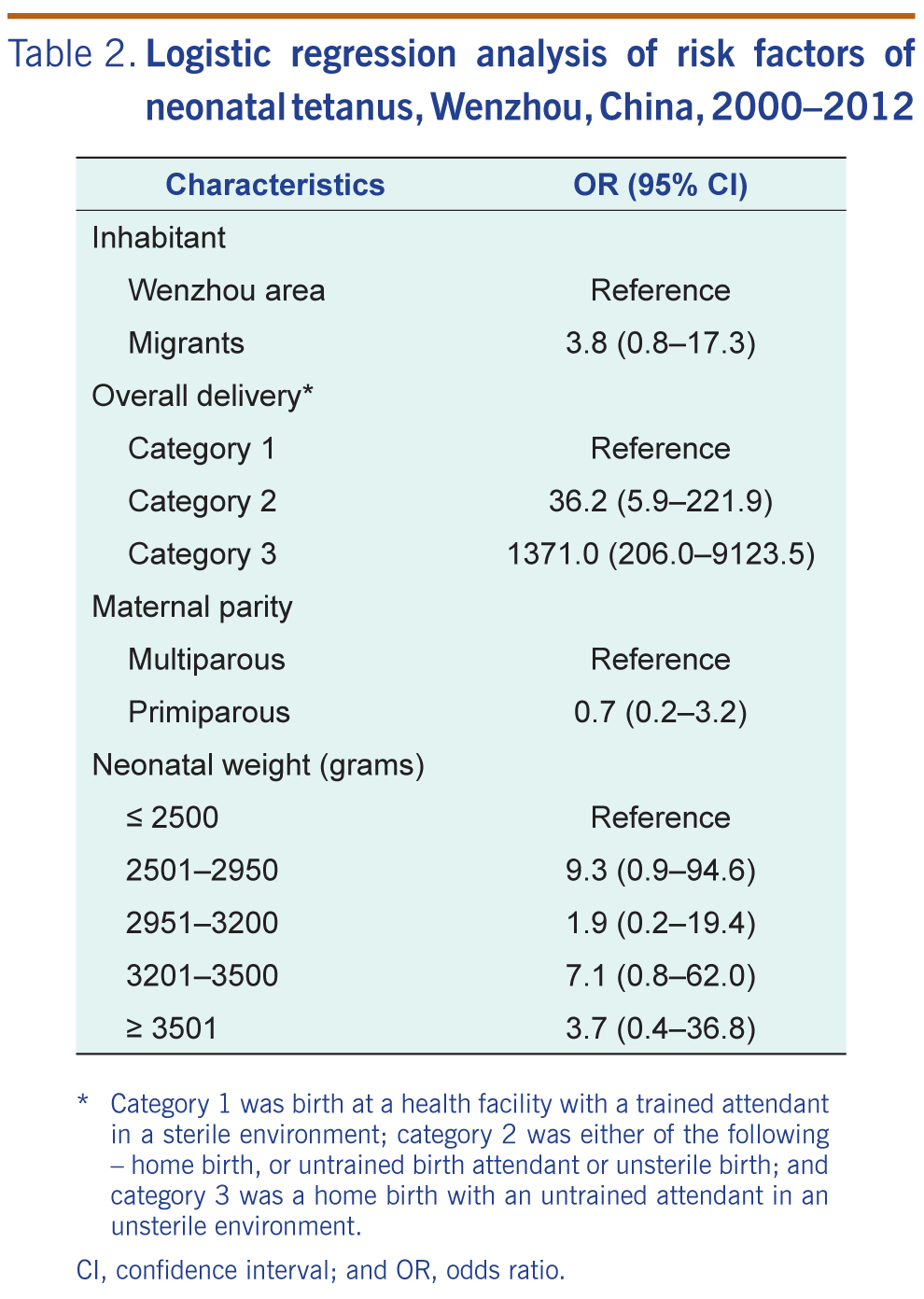
In the multivariate model, having one of the three birthing factors – a home birth, untrained birth attendants or unsterile delivery – and having all three remained as significant risk factors for neonatal tetanus (OR: 36.2; 95% CI: 5.9–221.9 and OR: 1371.0; 95% CI: 206.0–9123.5, respectively) (Table 2).
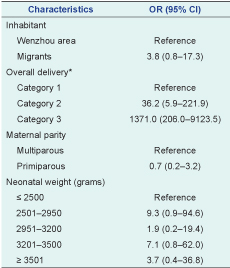
* Category 1 was birth at a health facility with a trained attendant in a sterile environment; category 2 was either of the following – home birth, or untrained birth attendant or unsterile birth; and category 3 was a home birth with an untrained attendant in an unsterile environment.
CI, confidence interval; and OR, odds ratio.
This study identified delivery by untrained attendants, home births and unsterile deliveries as risk factors for neonatal tetanus in Wenzhou city in south-eastern Zhejiang province, China, similar to that previously reported.12–15 Poverty, low maternal and paternal education, rural residence, young maternal age, cultural restrictions on access to health services for pregnant women from resource-poor regions associated with unhygienic practices, low antenatal care attendance and inadequate vaccination with tetanus toxoid have all been recognized as risk factors for neonatal tetanus.2,6,15,22,23
Untrained birth attendants often lack knowledge about sterilization and therefore use unsterile delivery appliances. The practice of cutting the cord with unsterile instruments by birth attendants is highly prevalent in the migrant population from Yunnan and Guizhou provinces;8 traditionally, birth attendants throw a bowl onto the ground and use a piece of the broken porcelain to cut the umbilical cord.24 During this investigation, this practice was recorded in the records of some pregnant migrant women. It is these unhygienic birthing practices that favour infection by C. tetani causing neonatal tetanus. Therefore, it is critical to target the migrant population for health promotion efforts to reduce neonatal tetanus, using interventions such as improved antenatal care, tetanus toxoid immunization of mothers, promotion of hygienic delivery, postpartum cord-care and relevant health education.8,25,26
There were some limitations in this study. Some known risk factors of neonatal tetanus, including the education level of the parents and immunization against tetanus were not recorded in the medical records and, hence, could not be assessed. The sample size was small, resulting in large confidence intervals. Using controls selected from hospital records also has the potential for bias as they may not represent the total population. This, as well as the location of our study and demographics of participants, suggests that the results obtained may not fully be representative of other areas or countries with different backgrounds. However, the risk factors identified in this study have all been documented before.4,5,12–17
The present study identified having an untrained birth attendant, home birth and unsterile deliveries were risk factors for neonatal tetanus in Wenzhou, China. To eliminate neonatal tetanus in this area, targeted measures that focus on improving the skills of birthing attendants as well as promoting hospital deliveries, tetanus immunization of pregnant mothers and health education are all recommended.
None declared.
This work was supported by a grant from the National Natural Science Foundation of China (grant no. 61373005) and the Wenzhou Science and Technology Project (grant no. Y20120006).
{kind=link}
{kind=link}
{kind=link}