
a Emerging Disease Surveillance and Response Unit, Division of Pacific Technical Support, World Health Organization, Suva, Fiji.
b The University of Newcastle, Callaghan, New South Wales, Australia.
c Office of the WHO Representative, Papua New Guinea Country Office, Port Moresby, Papua New Guinea.
Correspondence to Eric J Nilles (e-mail: nillese@wpro.who.int).
To cite this article:
Craig AT, et al. Risk posed by the Ebola epidemic to the Pacific islands: findings of a recent World Health Organization assessment. Western Pacific Surveillance and Response Journal, 2015, 6(2):45–50. doi:10.5365/wpsar.2015.6.1.009
Objective: To assess the public health risk posed by the ongoing Ebola virus disease (EVD) epidemic in West Africa to Pacific island countries and areas and to highlight priority risk management actions for preparedness and response.
Method: The likelihood of EVD importation and the magnitude of public health impact in Pacific island countries and areas were assessed to determine overall risk. Literature about the hazard, epidemiology, exposure and contextual factors associated with EVD was collected and reviewed. Epidemiological information from the current EVD outbreak was assessed.
Results: As of 11 March 2015, there have been more than 24 200 reported cases of EVD and at least 9976 deaths in six West African countries. Three EVD cases have been infected outside of the West African region, and all have epidemiological links to the outbreak in West Africa. Pacific island countries’ and areas’ relative geographic isolation and lack of travel or trade links between countries with transmission means that EVD importation is very unlikely. However, should a case be imported, the health and non-health consequences would be major. The capacity of Pacific island countries and areas to respond adequately varies greatly between (and within) states but in general is limited.
Discussion: This risk assessment highlights the needs to enhance preparedness for EVD in the Pacific by strengthening the capacities outlined in the World Health Organization Framework for Action on Ebola. Priority areas include the ability to detect and respond to suspected EVD cases quickly, isolation and management of cases in appropriately resourced facilities and the prevention of further cases through infection prevention and control. These efforts for Ebola should enhance all-hazards public health preparedness in line with the International Health Regulations (2005).
Ebola virus disease (EVD) – previously known as Ebola haemorrhagic fever – is a severe, often fatal illness of humans. The disease first appeared in 1976 in two simultaneous outbreaks in South Sudan (formerly part of Sudan) and the Democratic Republic of Congo (formerly Zaïre).1 The origin of the virus is unknown, but fruit bats are considered the likely reservoir of the Ebola virus.2,3 Initial symptoms include fever, fatigue, muscle pain, headache and sore throat followed by vomiting and diarrhoea. EVD can result in hepatic damage, renal failure, terminal shock and multiorgan dysfunction.2,4,5 The case fatality rate associated with previous EVD outbreaks has been between 25% and 90%;2,3,6–12 the rate associated with the current outbreak in West Africa – the largest ever recorded – is estimated to be 60–70%.12 Children aged less than five years, the elderly and pregnant women are particularly vulnerable.5 Appropriate clinical management has been shown to improve survival.13
The Pacific covers almost one third of the earth and comprises approximately 11.4 million people (excluding Australia and New Zealand). Of these, 8.2 million reside in Papua New Guinea with the remaining 3.2 million dispersed over many hundreds of islands and atolls that make up the other 20 Pacific island countries and areas. Eight Pacific island countries and areas have populations of less than 25 000, three have populations of less than 10 000; Niue and Tokelau each have populations of approximately 1200 people. Fourteen Pacific island countries are States Parties to the International Health Regulations (IHR 2005), and seven are territories or administrative areas for which IHR (2005) responsibilities are delegated to their metropolitan country. The majority of the Pacific island countries and areas are considered to be lower-middle income.14
Risk assessment is a systematic process for gathering, documenting and assessing information about the public health risk posed by a threat to inform actions based on the level of risk, resource availability, competing health priorities and other context considerations.15 The objective of this risk assessment was to estimate the likelihood of EVD importation into Pacific island countries and areas and to assess the magnitude of public health and societal impact should a case be imported.
This paper reports the risk assessment conducted by the World Health Organization (WHO) Division of Pacific Technical Support in Suva, Fiji as at March 2015. Pacific island countries and areas included American Samoa, Cook Islands, Fiji, French Polynesia, Guam, Kiribati, the Marshall Islands, the Federated States of Micronesia, Nauru, New Caledonia, Niue, the Commonwealth of the Northern Mariana Islands, Palau, Papua New Guinea, the Pitcairn Islands, Samoa, Solomon Islands, Tokelau, Tonga, Tuvalu, Vanuatu, and Wallis and Futuna. The assessment of the likelihood of EVD importation and its impact on public health follow the WHO guidance for undertaking risk assessments of acute public health events.15
The risk assessment was conducted by experienced specialists in public health surveillance and response, epidemiology and virology; all have experience in public health in Pacific island countries and areas. This includes experience in monitoring IHR (2005) core capacities in the Pacific.14 Their findings were reviewed by a broader group of WHO experts with expertise in laboratory methods, epidemiology, infectious diseases, risk communication and emergency planning.
Scientific literature about the epidemiology of the Ebola virus and the current Ebola epidemic was collected from co-authors, WHO situation reports and through MEDLINE.
EVD is a severe, often fatal, illness readily transmitted from an infected human if adequate personal protective measures are not in place; it is believed there is no risk of transmission before symptom onset.2 The incubation period for EVD is two to 21 days.12,16
Human-to-human transmission of EVD is usually by direct contact (through broken skin or mucous membranes) with the blood, secretions, organs or other body fluids of a symptomatic EVD case or person who has died of EVD.3,17 Indirect exposure through contact with surfaces or materials (e.g. bedding, patients’ clothes) contaminated with these fluids is possible, although not common. Fomite-mediated transmission in a clinical setting, where surface decontamination occurs frequently, is unlikely.18 People with direct exposure to infected cases or their blood or body fluids, such as health-care workers without appropriate personal protective equipment (PPE), other caregivers in hospitals or home settings, or persons handling bodies of deceased EVD cases are at high risk of Ebola virus exposure and infection.3,12,19–21
The Ebola virus is detectable at low levels in the blood of an infected case at the time of symptom onset; however, it may take up to three days of illness for virus levels to reach reliably detectable levels. The viral load increases logarithmically during the acute phase of illness and decreases during clinical recovery. Bodies of deceased EVD patients remain highly viraemic and hence are highly contagious. Ebola virus has been detected in other body fluids such as semen, breast milk and saliva during the acute and convalescent phase of illness.22
As of March 2015 the EVD outbreak was contained in West Africa with only three EVD cases having being infected outside of this region. All cases infected in non-West African countries had clear epidemiological links to the outbreak in West Africa.19,23
Importation of EVD into the Pacific would require an infected traveller to arrive in the Pacific undetected. There is very limited travel and/or trade links between West Africa and the Pacific, suggesting that the likelihood of a traveller, let alone a traveller who has been in direct contact with the blood or body fluids of an EVD-infected case, arriving in the Pacific is very low. There is no direct flight from West Africa to the Pacific; passengers are required to transit a minimum of three major international airports. Therefore an infected traveller would have to pass through several airport and airline EVD surveillance procedures undetected before reaching the Pacific islands. Airport-based and airline EVD surveillance includes collecting information about travellers’ health (to detect potential symptomatic EVD-infected travellers) and their recent travel history (to identify travellers who have been to an EVD-affected country and may have been exposed regardless of symptom status). Patients travelling for medical care are unlikely to choose a route that passes through the Pacific, rather seeking care in countries within direct flight reach (i.e. United States of America, European or African countries).
Health-care workers, including medical and nursing staff, laboratory scientists, ancillary health staff and volunteer carers of EVD cases in West Africa, have an elevated risk of exposure to the Ebola virus.12 Members of this group, if travelling to the Pacific within the disease’s incubation period, pose a potential importation risk to the Pacific. At the time of writing there were approximately 90 aid and military personnel from Pacific island countries and areas and neighbouring countries serving in EVD-affected countries. These included 27 Fijian United Nations peace keepers and one New Zealand health worker in Liberia, one New Zealand water engineer, one New Zealand security guard and 10 New Zealand and 50 Australian health workers in Sierra Leone (V Biaukula, WHO Division of Pacific Technical Support, personal communication, 18 December 2014; J Mansour, Australia Department of Health, personal communication, 17 December 2014; and S Gilbert, New Zealand Ministry of Health, personal communication, 17 December 2014). According to national health agency protocols in Australia, New Zealand and Fiji, all returning health workers (whether symptomatic or asymptomatic) will perform daily home-based health screening and be monitoring for 21 days (the maximum incubation period for the virus) after leaving an EVD-affected country (V Biaukula, WHO Division of Pacific Technical Support, personal communication, 18 December 2014).17,24,25
Context assessment examines setting-related factors that influence the vulnerability of the population to health impacts associated with a hazard.15 For EVD, capabilities to implement prevention, preparedness and control measures to decrease the level of risk are pertinent. The assessment was undertaken in the context of the broader global public health response to the EVD epidemic and the resulting protective influence these actions have on risk of EVD importation into Pacific island countries and areas.
While the likelihood of a symptomatic or asymptomatic EVD-infected person arriving in the Pacific and evading all screening mechanisms on route is very low, it is possible. The capacity of Pacific island countries and areas to detect and respond to EVD in the community and to undertake the associated community-based public health control measures required (e.g. contact tracing, risk communication) varies between states but in general is limited. All Pacific island countries and areas are enhancing preparedness for EVD; however, existing resource and workforce limitations, geographic isolation and limited communication infrastructures, and logistic constraints pose major barriers to achieving event readiness in a short time frame.
Results of a survey of Member States in the WHO Western Pacific Region (of which 14 are Pacific island countries) conducted in October 2014 aimed to assess states’ preparedness to respond to EVD. The survey highlighted that achieving the necessary core capacities in Pacific island countries (and areas) is difficult. The survey found that four (31%) of the 13 Pacific island countries that responded reported not yet having a health care facility designated to isolate suspected or confirmed cases of EVD. Further, only two (15%) reported having adequate supplies of PPE in country for EVD rapid response and containment operations. The survey reported that awareness of the EVD situation was high and that the governments of all Pacific island countries were monitoring the global situation; however, few (n = 4; 31%) had conducted country-specific risk assessments. Nine (69%) surveyed Pacific island countries self-reported having adequate early warning surveillance systems to detect potential EVD; however, only four (31%) reported having EVD-specific investigation protocols developed or having trained rapid response teams in EVD response procedures.26
Globally, governments, airlines and major international travel hubs are conducting surveillance for EVD (including exit health screening in affected countries) in a concerted effort to stop the global spread of the disease. International airports in the Pacific have introduced EVD-specific health and travel history declaration cards to screen arriving passengers, have EVD risk communication messages displayed in airport arrival halls, and have mechanisms in place to isolate and interview sick travellers. Such efforts further reduce the risk of importation of EVD into the Pacific.
Access to laboratory facilities able to test for EVD is limited in Pacific island countries and areas. The closest laboratories able to test for EVD are the Victorian Infectious Diseases Reference Laboratory in Melbourne, Australia (preliminary testing only) and the WHO Collaborating Centre Laboratory at the United States Centers for Disease Control and Prevention in Atlanta, USA (definitive testing).27 The time required to transport specimens to these facilities range from one to seven days; therefore, health authorities will need to initially act based on a clinical diagnosis.
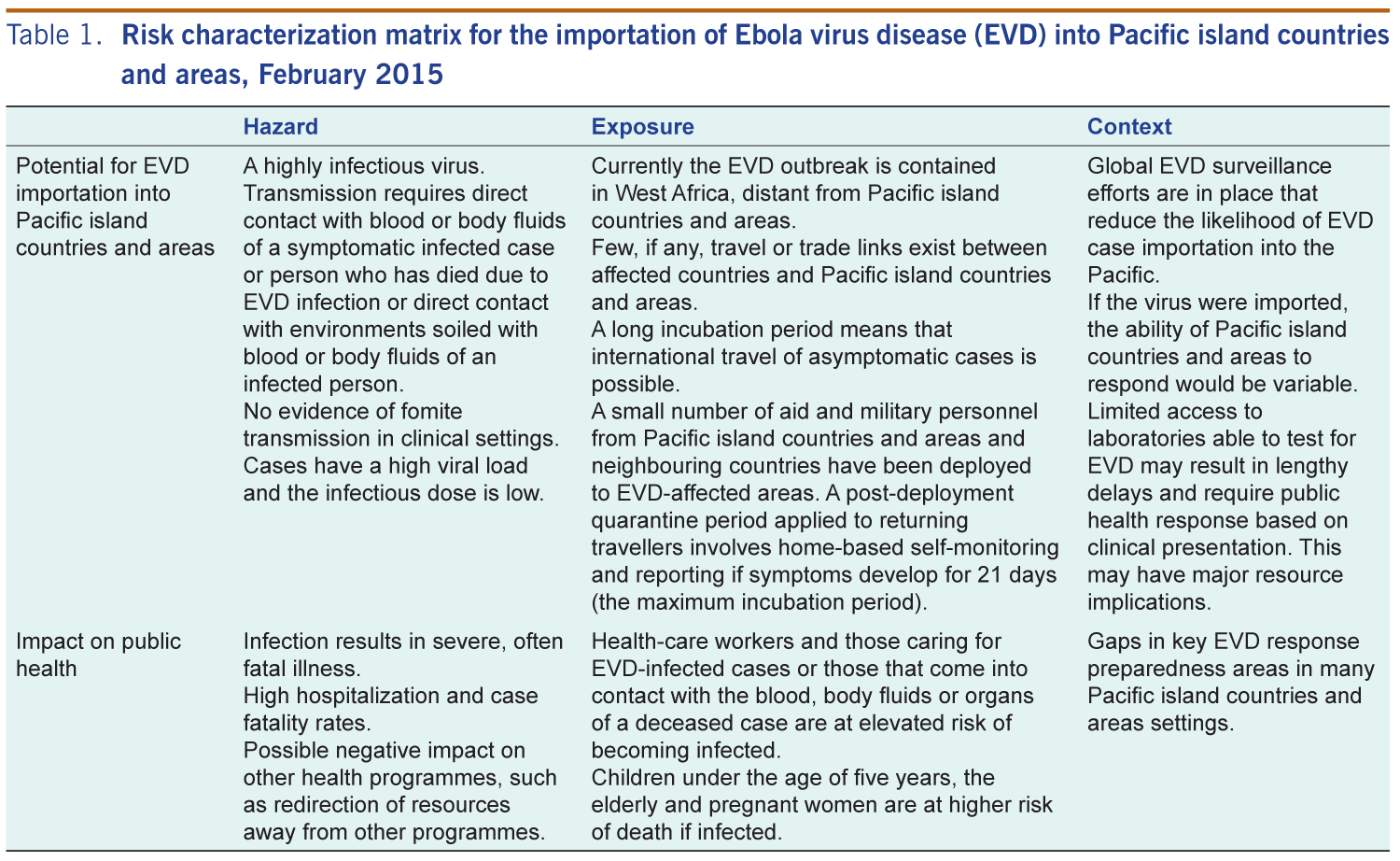
The information from the risk characterization (summaries in Table 1) suggests that the likelihood of EVD importation into the Pacific is very low, especially as the outbreak Guinea, Liberia and Sierra Leone is stabilizing. However, if it were to occur, the existing gaps in surveillance, response and infection prevention and control capacity in many Pacific island countries and areas would mean that both the public health and broader societal consequences could be major. Building core IHR (2005) and EVD-specific capacities in surveillance, infection prevention and control and outbreak response is warranted and will help to strengthen all-hazards alert and response capacities in the Pacific region.
Although the likelihood of EVD importation into the Pacific is low, this risk assessment highlights that Pacific island countries and areas need to assess and enhance their core public health capacities to be able to effectively detect and respond to suspected or confirmed EVD cases. EVD preparedness should focus on the capacities outlined in WHO’s Framework for Action on Ebola,28 which include: command and control, surveillance, risk assessment and response, laboratory, clinical management and infection prevention and control, public health interventions (including those at international points of entry) and risk communication. As these capacities are required for most public health emergency responses, efforts for an EVD-specific threat should have long-term value by enhancing an all-hazards approach to public health preparedness in line with the IHR (2005).
While it is important to address all capabilities in the Framework for Action on Ebola, an immediate priority for Pacific island countries and areas is to ensure suitable isolation facilities are identified to accommodate and treat suspected and confirmed EVD cases. These facilities need to be adequately resourced with staff trained in the clinical management of EVD and EVD-related infection prevention and control, appropriate stock of PPE and systems for timely deployment and mechanisms for safe management of clinical and human waste.
This risk assessment has some limitations. As it was defined by the epidemiological and contextual situation at one point in time (in this case March 2015), it will need updating as the situation evolves or new information surfaces. The assessment applies to the Pacific region as a whole and did not assess variability in risk or capacity to respond for individual Pacific island countries or areas. Pacific islands are encouraged to build on this risk assessment by further exploring their jurisdictions’ specific level of exposure, vulnerability and resilience to EVD. Finally, risk assessments, by their nature, are subjective; therefore, other risk assessments may have different outcomes.
None declared.
None.
We acknowledge the ongoing support provided by the WHO Regional Office for the Western Pacific Ebola Emergency Support Team. We acknowledge and thank Professor David Durrheim and Dr Beverly Paterson of the University of Newcastle (Australia) for reviewing this risk assessment and for their valuable contributions.
{kind=link}