a Surveillance and Epidemiology Branch, Centre for Health Protection, Department of Health, Hong Kong Special Administrative Region.
b Field Epidemiology Training Programme, Hong Kong Special Administrative Region.
Correspondence to Poon Kwok-ming (e-mail: mo_fetp1@dh.gov.hk).
To cite this article:
Poon et al. International Health Regulations (2005) facilitate communication for in-flight contacts of a Middle East respiratory syndrome case, Hong Kong Special Administrative Region, 2014. Western Pacific Surveillance and Response Journal, 2015, 6(1):62–65. doi:10.5365/wpsar.2015.6.1.008
The International Health Regulations (IHR) (2005) require World Health Organization Member States to notify events fulfilling two of four criteria: (1) serious public health impact; (2) unusual or unexpected event; (3) significant risk of international spread; or (4) significant risk of international travel or trade restrictions.1 In-flight transmission of infections like severe acute respiratory syndrome is well documented.2 With the enormous amount of air travel today, the risk of increasing in-flight transmission and subsequent international spread of infections are increasing. Prompt notification and information sharing under the IHR mechanism is critical for effective contact tracing and prompt control measures. We report on a case of in-flight exposure to an infection with significant public health risks that was successfully resolved using IHR (2005) guidelines.
The government of the Hong Kong Special Administrative Region launched the Preparedness Plan for Middle East Respiratory Syndrome (MERS) in June 2014, upholding established principles of rapid control of disease transmission and responsive risk communication.3 It sets out a multidisciplinary disease control framework involving the Department of Health, Hospital Authority, the travel industry and airlines, etc. Under the plan, the Centre for Health Protection of the Department of Health developed protocols for case and contact management. Its risk-based classifications of “close” and “other” contacts determine subsequent public health actions, including quarantine/travel restrictions for close contacts, medical surveillance, referral, isolation and laboratory investigation.
On 2 October 2014, the World Health Organization (WHO) Western Pacific Regional Office informed through the IHR mechanism of Hong Kong Special Administrative Region that a Chinese national, whose point of origin was Hong Kong Special Administrative Region, sat near a MERS case on a flight from Qatar to Austria. Subsequent investigations revealed that a Hong Kong Special Administrative Region tour group of 42 members was on the same flight. We report investigations and public health measures for these in-flight contacts while they were still on their journey in Europe.
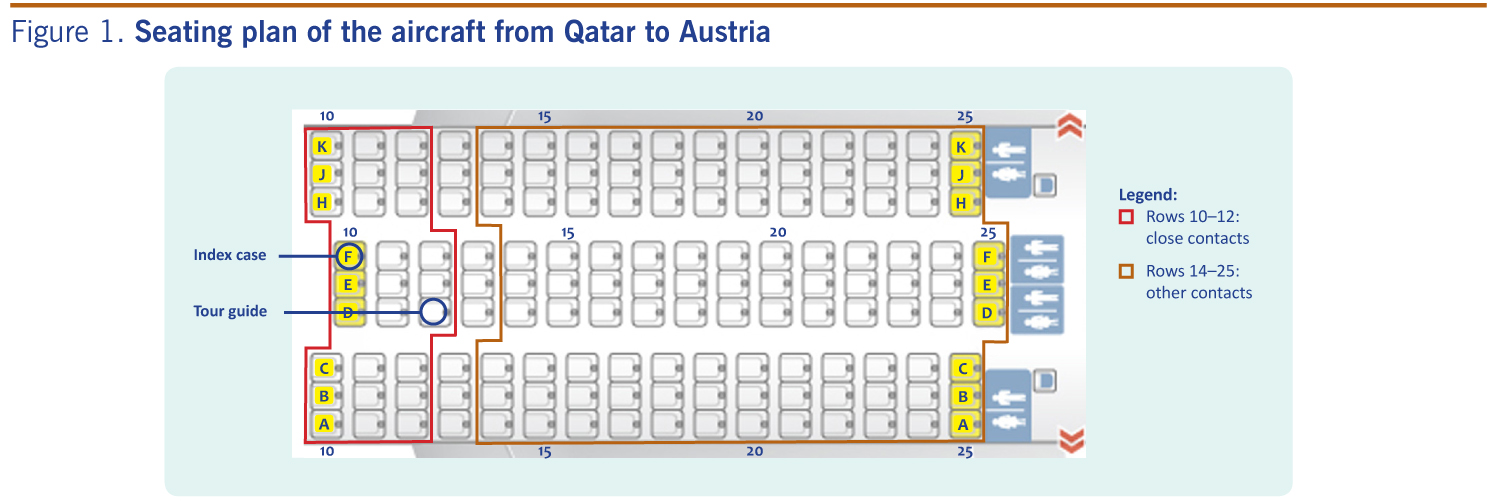
We obtained information on the index case and a passenger list detailing points of origin and seat numbers from the WHO Regional Office through IHR communications. Contact tracing was performed according to the Preparedness Plan for MERS whereby “close contacts” were defined as passengers seated in the same row or up to two rows in front of/behind the case, and “other contacts” as other passengers seated in the same cabin or passengers from the same tour group. The airline provided the aircraft seating plan, and the travel agency provided a tour member list. We crosschecked the tour member list with the list provided by the WHO Regional Office and the aircraft seating plan. The health conditions of all contacts were ascertained over the phone and health advice was provided. Using the International Health Regulations (IHR) mechanism, we informed relevant overseas health authorities of our epidemiological findings and collaborated with them to implement control measures for the contacts. We continued medical surveillance after the contacts had returned to Hong Kong Special Administrative Region and provided risk communications to Hong Kong Special Administrative Region general public.
The index case was a citizen of Saudi Arabia who had symptoms of upper respiratory tract infection and fever from 17 September 2014. She was still symptomatic when she travelled on a flight from Qatar to Austria on 22 September. Austrian health authorities confirmed she was a case of MERS on 29 September. On 2 October, the WHO Western Pacific Regional Office informed through the IHR mechanism of Hong Kong Special Administrative Region that a Hong Kong Special Administrative Region citizen who had been seated within two rows of the index case on the flight. The passenger list included an additional 42 passengers with Hong Kong Special Administrative Region as their points of origin.
We classified the Hong Kong Special Administrative Region citizen (seat 12D) as a close contact (within two rows of index case: seat 10F); he was the tour guide of the 42 other Hong Kong Special Administrative Region passengers. Twenty of these passengers were seated in the same cabin as the index case, however all 42 tour members were managed as other contacts (Figure 1). All contacts were travelling through Europe and had reached Poland on 1 October. On 2 October (Day 10 of last exposure from the flight), we ascertained that none had been sick since 22 September. We advised the tour guide to minimize contact with the group and for the whole group to wear face masks during their journey. We issued a press release on 2 October.
We alerted Poland health authorities on 2 October to the whereabouts of the tour group. The return flight of the tour guide was postponed to 6 October (Day 14 – maximum incubation period of MERS) to avoid potential risk to other travellers in case the tour guide developed symptoms during his flight back to Hong Kong Special Administrative Region. Poland health authorities conducted medical surveillance of the tour guide who voluntarily stayed in a hotel in Poland until 6 October. He did not develop symptoms.
The 42 tour members boarded the scheduled return flight departing from Poland on 3 October. With assistance from the airline, we arranged for them to sit at the back of the aircraft and stay on board after arrival at Hong Kong Special Administrative Region for health screening. All were asymptomatic upon return to Hong Kong Special Administrative Region. Their health status was monitored by telephone interview until 20 October (Day 28 – twice the maximum incubation period of MERS) with good compliance. A tour member who reported respiratory symptoms on 6 October was promptly isolated; she tested negative for MERS. Through the IHR mechanism, we communicated our actions to Poland and Austria health authorities and other IHR colleagues in Europe.
International air travel of a symptomatic MERS case constitutes a potential risk of international spread of MERS-coronavirus and sufficient criteria for IHR notification.1 With the successfully triggered IHR mechanism, the WHO Regional Office informed through IHR mechanism of Hong Kong Special Administrative Region within three days of diagnosis of the case. This communication facilitated effective contact tracing and prompt implementation of control measures and was timely in preventing the tour guide from boarding the return flight.
Communication under the IHR mechanism has been widely adopted and used in the Western Pacific Region since the endorsement of IHR in 2007, especially regarding information on emerging infectious diseases. The Hong Kong Special Administrative Region has been active regarding notification and information exchange with WHO.4 The IHR mechanism has facilitated contact tracing for infectious diseases among Member States in the past.4 Well-established channels of communication under IHR have also enabled efficient collaboration between health authorities across continents. In this case, smooth implementation of control measures required a great deal of international coordination. While Poland’s health authorities took charge of necessary local measures, we helped to reschedule the tour guide’s return flight. This efficient collaboration and timely arrangement stopped him from boarding another international flight, reducing the potential risks if he had in-flight onset of symptoms.
Under the Preparedness Plan for MERS, the response was based on risk-based contact management. Only the tour guide’s return flight was postponed until Day 14; the other tour members travelled back to Hong Kong Special Administrative Region as scheduled. The multidisciplinary disease control framework among the Department of Health, the travel industry and airlines allowed for smooth communications and precautionary travel arrangements for the tour members on their return flight and the subsequent return of the tour guide. The preparedness plan also resulted in immediate referral, isolation and testing of the symptomatic tour member after their return, relying on coordinated efforts among the Department of Health, Hospital Authority and the ambulance centre under the Fire Services Department.
Although there are international risk assessment guidelines regarding aircraft transmission of various infectious diseases,5 guidelines for emerging infections like MERS are still evolving and differ by country. For instance, the Public Health Agency of Canada considers passengers in the same row and up to three rows in front of/behind as priority, recommending all passengers should be followed up when feasible;6 the Health Protection Agency in the United Kingdom defines close contacts as those sitting in the same row and up to two rows in front of/behind.7 WHO defines close contacts as those travelling together with a MERS case in any kind of conveyance.8 Such variations result in different management of contacts among countries. Despite the small risk to the 42 tour members on board, we took a precautionary approach and managed them all as other contacts, taking into account the uncertainties of unrecognized in-flight exposure in the same cabin and the common practice of seat swapping among tour group members.
We also adopted a more stringent approach than most international guidelines for the length of contact tracing. WHO recommends that close contacts should be monitored for the appearance of respiratory symptoms for 14 days after last exposure;9 we decided to extend health monitoring to 28 days, taking into account the potential risks of hidden chains of transmission within the tour group and the availability of our resources. We acknowledged the inter-organizational differences in risk assessment and extent of information sharing and adhered to our protocol. We extended our scope of contact tracing and identified additional contacts by combining all sources of information from WHO, the airline and the tour member list obtained from the travel agency. Fortunately, all other contacts were from the same tour group, greatly facilitating investigation and control measures.
Three lessons were learnt from this public health event. First, timely information sharing and communications under IHR mechanisms greatly facilitated our contact tracing and management by allowing efficient collaboration with overseas health authorities and the WHO Regional Office. Second, effective contact tracing enabled prompt control measures for flight rescheduling and precautionary travel arrangements to minimize further disease transmission. Third, a well-established preparedness plan, including a protocol for contact management, ensured efficient management of in-flight contacts of an overseas MERS case.
None declared.
None.
We would like to thank all staff of the Hong Kong Special Administrative Region Surveillance and Epidemiology Branch of the Centre for Health Protection who contributed in the investigation and control of this outbreak. We would also like to thank Dr Alain Moren and Dr Marta Valenciano for their advice in report writing.
{kind=link}