
a School of Public Health and Primary Care, College of Medicine, Nursing and Health Sciences, Fiji National University, Suva, Fiji.
b Fiji Ministry of Health, Suva, Fiji.
c Australian Volunteer for International Development, Suva, Fiji.
d Fiji Centre Communicable Diseases Control, Ministry of Health, Suva, Fiji.
e Ba Medical Subdivision, Western Health Services, Suva, Fiji.
Correspondence to Aneley Getahun (e-mail: aneley.getahun@fnu.ac.fj).
To cite this article:
Getahun A et al. Hepatitis A outbreak in Ba subdivision, Fiji, October–December 2013. Western Pacific Surveillance and Response Journal, 2015, 6(2):32–36. doi:10.5365/wpsar.2014.5.4.006
Objective: A cluster of suspected hepatitis A cases was notified to the Fiji Ministry of Health on 22 October 2013. An outbreak investigation team was mobilized to confirm the existence of an outbreak of hepatitis A and advise appropriate public health interventions.
Methods: A case definition for the outbreak investigation was established, and standardized data collection tools were used to collect information on clinical presentation and risk factors. An environmental assessment was also conducted.
Results: There were 160 clinical cases of hepatitis A of which 15 were laboratory-confirmed. The attack rate was 349 per 10 000 population in the Nukuloa nursing zone; there were no reported deaths. Residents of the Nukuloa settlement were 6.6 times more likely to present with symptomatic hepatitis A infection (95% confidence interval: 3.8–12.6) compared with residents of another village with a different water supply.
Discussion: This is the first significant hepatitis A outbreak documented in Ba subdivision and possibly in Fiji. Enhanced surveillance of hepatitis A may reveal other clusters in the country. Improving the primary water source dramatically reduced the occurance of disease in the affected community and adjacent areas.
Fiji is an archipelago in the South Pacific consisting of over 300 islands with an estimated population of 837 000 comprised of 58% Indigenous Fijians and 35% Fijians of Indian descent.1 There is a paucity of information on the epidemiology of hepatitis A virus (HAV) in Fiji. The only published study on HAV seroprevalence was reported in 1976–1978 when about 84% of samples were positive for HAV-specific antibodies. The age-specific prevalence of anti-HAV was 13% in children under 5 years, 60% among 6–10 year olds and 90% by the age of 20.2 There have been a few anecdotal or unpublished reports of hepatitis A in Fiji but no reported community outbreaks of significance.3,4 Hepatitis A cases have been associated with Kava (a plant-based sedative) drinking among tourists returned from Fiji.5
Hepatitis A is one of the communicable diseases under routine surveillance in Fiji; it is also mandatory for an outbreak or cluster of suspected cases to be reported within 24 hours to the Ministry of Health and the Fiji Centre for Communicable Diseases Control (FCCDC).6
The study area for this investigation is Ba subdivision, an agricultural centre situated on the north-western side of Viti Levu, Fiji’s main island. According to the Ba hospital, the estimated population of Ba subdivision is 55 805 with Fijians of Indian descent (72%) making up the largest proportion. The Ba subdivision has three health centres: Ba town, Balevuto and Nailaga. The Balevuto medical area consists of two nursing zones: Nukuloa and Moto, and the hospital estimated a population of 6255 of which 68% are Fijians of Indian descent.
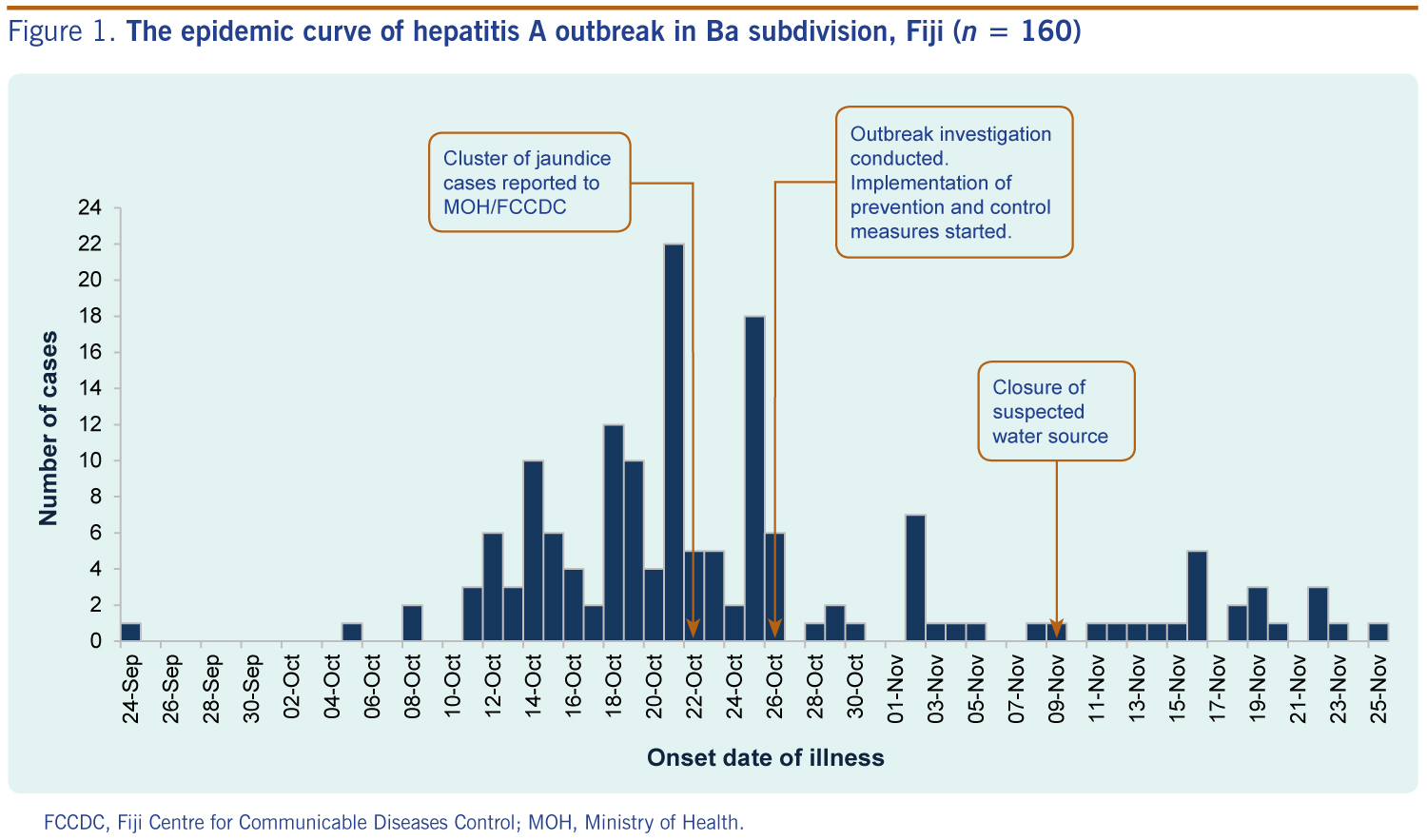
On 22 October 2013, a cluster of eight cases of jaundice and fever was reported to FCCDC from the Balevuto medical area. A joint team from FCCDC and the Fiji National University conducted an investigation and recommended public health measures to control the outbreak and prevent further spread.
The outbreak investigation followed FCCDC outbreak response guidelines.6 The investigation team was mobilized within 24 hours after the report of the jaundiced cases.
A suspected case of hepatitis A was defined as a patient presenting with an acute illness with two or more of the following symptoms: fever, headache, malaise, anorexia, nausea, vomiting, diarrhoea, abdominal pain and either jaundice or elevated serum aminotransferase between 8 October and 2 December 2013. A confirmed case was a suspected case with positive anti-HAV IgM or an epidemiological link with a laboratory-confirmed case.7 A line list of patients who presented with jaundice and other related symptoms was obtained from the Ba subdivisional hospital and the Balevuto health centre, and the team conducted house-to-house visits for active case finding and health promotion activities.
A structured questionnaire that included demographics, clinical presentation, food, water, other risk factors and exposure history for the two to six weeks before onset was used. Risk and exposure factors collected as part of the outbreak investigation included history of eating raw/undercooked shell fish, contact with a jaundice patient or a confirmed hepatitis A patient, history of travel, and attending public/private gatherings two to six weeks before the onset of illness. Blood samples were collected for biochemistry (liver function and renal function tests), full blood counts, dengue and leptospirosis serology testing; 14 serum samples were sent to Suva Private Hospital for anti-HAV IgM testing using the ElecsysAnti-HAV IgM test (Roche Diagnostics, Germany).
An environmental assessment was conducted to determine potential sources of infection. Drinking-water samples were collected from the main water source and from selected households for analysis at the FCCDC public health laboratory. Coliform and Escherichia coli counts by the most probable number per 100 ml of sample were conducted to determine the level of contamination.
Data were entered and analysed using Microsoft Office Excel 2007. An epidemic curve used the date of onset of illness; if this was unknown, the date of blood sample collection. Attack rates and relative risk for exposure variables were calculated by medical areas. A spot map was used to assess cases by geographical areas.
There were 160 suspected cases of hepatitis A of whom 18 were confirmed (15 by serology and 3 by epidemiological link). The majority of cases were men (66%), and Fijians of Indian descent accounted for 93%. The mean age was 31 years with 46% aged between 10 and 29 years (range: 3–80 years). The attack rates were 246, 5 and 0.3 per 10 000 population in Balevuto, Nailaga and Ba medical areas, respectively. Within the Balevuto medical area, the attack rate for Nukuloa was 349 per 10 000 population, and 52 per 10 000 population in Moto.
Common symptoms included fever (86%), jaundice (85%), anorexia (69%), malaise and/or nausea (65%), abdominal pain (63%) and vomiting (53%). Other less common symptoms included headache, body pain and dark urine. The mean serum aspartate transaminase (AST) and alanine transaminase (ALT) were 1165 and 1575 μ/L, respectively. There were no deaths.
The epidemic curve shows that about 30% (n = 48) of cases were reported within four days between 18 and 21 October (Figure 1). The index case was a 59-year-old female resident of the Nukuloa settlement area whose illness began on 24 September. Her initial symptoms included fever, vomiting and nausea followed by yellowish discoloration of the eyes. Her serum sample was insufficient for HAV serology test; her liver function had an AST of 2550 μ/L and ALT of 2610 μ/L. She had no history of travel outside of Ba or contact with a jaundiced patient.
FCCDC, Fiji Centre for Communicable Diseases Control; MOH, Ministry of Health.
Data on exposures and risk factors were collected from 50 cases. A total of 18 cases (36%) reported a history of contact with jaundiced patients, mainly another family member. Approximately one quarter (24%) of cases attended social gatherings, public functions or family gatherings where food was served. All visited houses had toilets and there was no report of open defecation.
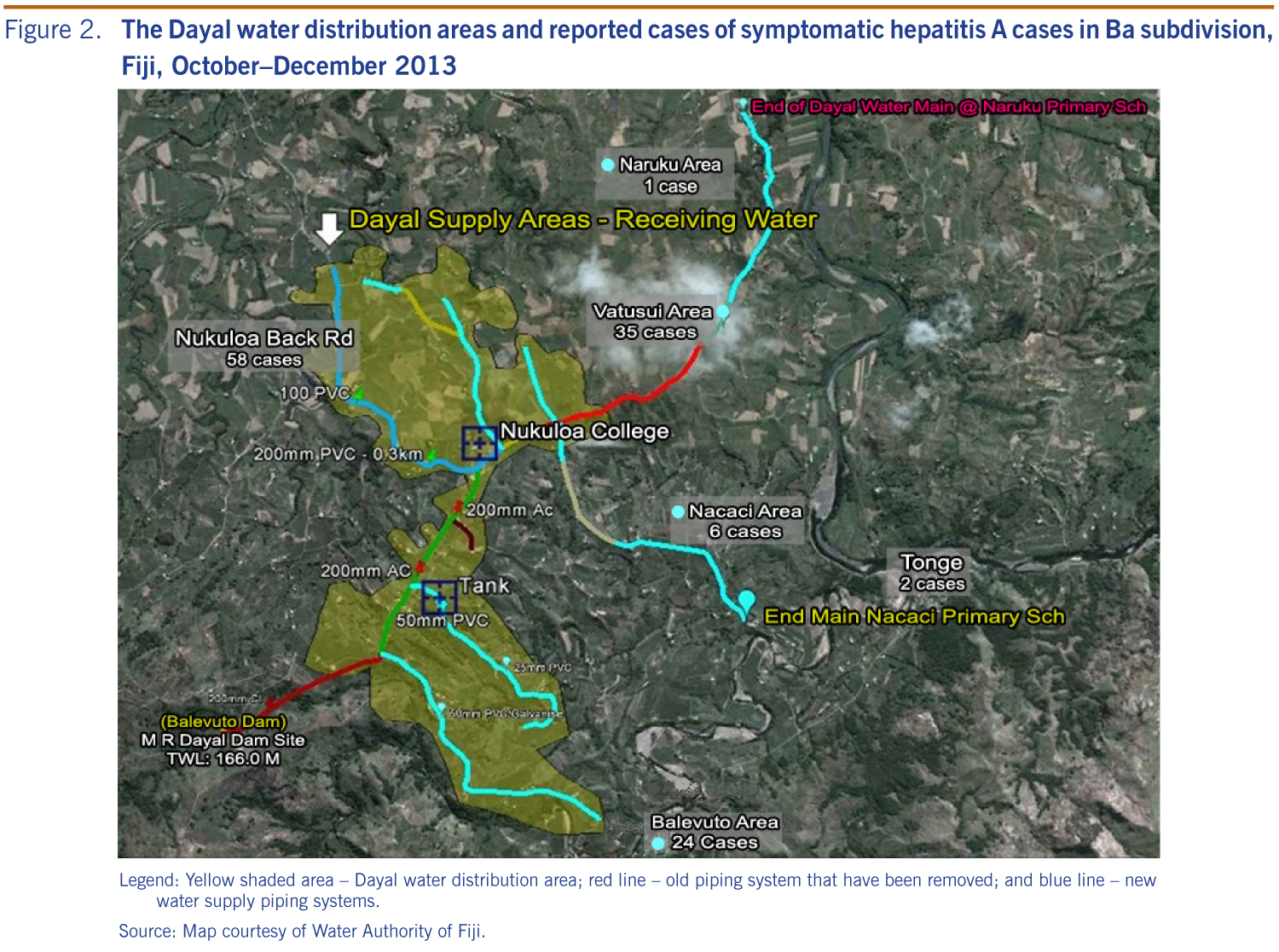
Ba town has access to a treated reticulated water supply provided by the Water Authorities of Fiji (WAF). However, most of the affected community of the Nukuloa settlement used the privately owned Waica dam (Dayal) (Figure 2), which was inspected by the outbreak investigation team. The Waica dam does not have a reservoir for treatment purposes and draws water directly from the river. At the time of the assessment, the water source had no surrounding barrier to prevent human or animal access to the dam. Water samples collected from the dam showed a high level of contamination with human or animal excreta (coliform: 43–153; E. coli: 5–43/100 ml) compared to samples taken from WAF water supply (coliform: < 3/100 ml; E. coli: nil). The relative risk of HAV infection for Nukuloa residents was 6.6 times more than those who reside in Moto who have a different water source (surface water) (95% confidence interval: 3.8–12.5).
Legend: Yellow shaded area – Dayal water distribution area; red line – old piping system that have been removed; and blue line – new water supply piping systems.
Source: Map courtesy of Water Authority of Fiji.
A taskforce was established to coordinate the outbreak response in Ba subdivision. Initial outbreak control measures included health promotion activities through mass media and community visits (schools, settlements and villages) with emphasis on boiling water, hand washing with soap, personal hygiene and food and water safety. Water purification tablets, water filters and hand sanitizers were also distributed to households in the Nukuloa settlement and schools. A health education pamphlet on hepatitis A was developed by the Ministry of Health and widely distributed to the affected areas. Outbreak-related information was posted on PacNet listserv in weeks 43 and 45.8
Health facilities in the affected areas were provided with additional medical supplies for supportive management of patients with hepatitis A. Outpatient department nurses conducted active triage to identify suspected cases for prompt review and management.
The taskforce continued with the recommended community interventions and actively lobbied with landowners and government administration to ensure safe drinking-water was supplied to affected households. As a result, on 9 November 2013, the Waica dam was temporarily closed while WAF undertook major upgrading work to the dam and water system. This later included a chlorination treatment plant and replacement of the old water piping system thus providing clean treated water to 600 households in the area.9
This is the first documented community outbreak of hepatitis A to occur in Ba, Fiji. The outbreak was most likely associated with a supply of untreated water to the Nukuloa settlement. There was geographic clustering of cases to areas that receive water from the Waica dam. Significant contamination of water (E. coli and coliform) taken from the dam on two occasions and the epidemic curve revealed a continuous source outbreak where cases increased over an extended period of time, approximately two weeks from 12 to 26 October.
Although about 30% of cases presented in four days, the epidemic curve does not exhibit the classic point source outbreak with significant clustering of cases in a short period of time. This is more compatible with a continuous source outbreak which could be attributed to prolonged common source exposure such as contaminated water. Community-based hepatitis A outbreaks from contaminated water have been reported in China and India.10,11 The propagated nature of the outbreak indicates person-to-person transmission which is likely to have contributed to sustaining the outbreak as well as spreading the infection to other parts of the subdivision, resulting in sporadic cases observed in the two adjacent medical areas.
The significant majority (93%) of hepatitis A cases were Fijians of Indian descent. The occurrence of symptomatic infection with HAV in older age groups in this outbreak suggests no prior exposure to the virus. The prevalence studies in the 1970s estimated the majority of infections were acquired at an early age, and disease prevalence was found to be equal among the two main ethnic groups.2 The findings from this outbreak investigation may indicate a change in the epidemiology of HAV in this subpopulation in Fiji.
This report is the first to document a hepatitis A outbreak at the community level in Fiji; however, it is limited in scope. It does not extensively examine the exposure and risk factors among the various communities, nor does it explain the difference in attack rates between the two ethnic groups. Detailed information on food eaten was not collected because of a long incubation period and recall bias concerns. Therefore, a foodborne cause cannot be ruled out. HAV surveillance in Fiji is from the passive detection of symptomatic patients mainly by public health facilities and does not include all patients treated in private health facilities or outside the Ba region. This may have underestimated the magnitude of the outbreak.
This is the first significant hepatitis A outbreak documented in Ba subdivision and possibly in Fiji. Improving surveillance for hepatitis A may reveal other clusters in the island. After improving the primary water source there was a reduction in cases in the affected community and adjacent areas.
None declared.
None.
The authors would like to thank all the medical officers, nurses, laboratory staff and health inspectors in Ba subdivision for their support throughout the outbreak investigation process. We would like to thank the FCCDC team for their technical and laboratory support.
{kind=link}
{kind=link}