a Infectious Disease Surveillance Center, National Institute of Infectious Diseases, Tokyo, Japan.
b Department of Virology, National Institute of Infectious Diseases, Tokyo, Japan.
c Department of Medical Entomology, National Institute of Infectious Diseases, Tokyo, Japan.
Correspondence to Yuzo Arima (e-mail: arima@niid.go.jp).
To cite this article:
Arima Y et al. Ongoing local transmission of dengue in Japan, August to September 2014. Western Pacific Surveillance and Response Journal, 2014, 5(4):27–29. doi:10.5365/wpsar.2014.5.3.007
In late August 2014, three autochthonous dengue cases were reported in Japan. Since then, as of 17 September 2014, a total of 131 autochthonous cases have been confirmed. While cases were reported from throughout Japan, the majority were linked to visiting a large park or its vicinity in Tokyo, and the serotype detected has been serotype 1. We report preliminary findings, along with the public health response activities, of the first documented autochthonous dengue outbreak in Japan in nearly 70 years.
Dengue is an acute, mosquito-borne febrile illness caused by a flavivirus found widely in the Asia-Pacific region, particularly in South-East Asia. While the most competent mosquito species for dengue virus transmission is believed to be Aedes aegypti, Aedes albopictus is also a competent vector present in much of Japan during the warmer months. Infection with dengue virus may cause fever, headache, muscle pain and/or rash but may also be mild or asymptomatic. While there is no specific treatment, with early and appropriate medical care, the likelihood of infections resulting in severe forms or death is rare.
In Japan, dengue has been a notifiable disease since April 1999. Physicians are required to report demographic, clinical and exposure history information of laboratory-confirmed cases to the local public health centre that are then reported to the Ministry of Health, Labour and Welfare (MHLW) and the National Institute of Infectious Diseases (NIID).1
In recent years, approximately 200 imported cases of dengue (those that had onset after returning to Japan following overseas travel) have been notified through national surveillance, the majority from South-East Asia.2,3 While the last reported local transmission of dengue was during the 1940s,4 given the growing number of imported cases and the recent emergence of dengue in areas such as the United States of America,5 France6 and Portugal,7 the re-emergence of dengue in Japan had been a concern in recent years. A travel-associated German case was suspected to have been infected with dengue serotype 2 while in Japan in summer 2013,8 and Japan’s MHLW and NIID have since been preparing guidelines to manage response activities in case of local transmission.
On 27 and 28 August 2014, three autochthonous dengue cases, with no overseas travel, were reported from Tokyo and Saitama prefectures. All three reported that they had visited Yoyogi Park, a large (54 hectare) forested park in the centre of metropolitan Tokyo and were bitten by mosquitoes there; illness onset was on 18, 20 and 24 August. MHLW alerted local public health authorities of the autochthonous cases and called for vigilance and timely reporting by clinicians; awareness also increased among the general public via both official MHLW and unofficial media channels.
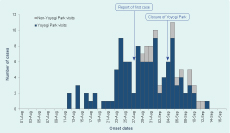
As of 17 September 2014, a total of 131 autochthonous cases have been reported; including cases that occurred before the initial three cases were detected (Figure 1). While cases were reported from 17/47 Japanese prefectures, the majority of cases (112/131 [85%]) were linked to Yoyogi Park or its vicinity. Of the 131 cases, 74 (56%) were male and 57 (44%) female. The median age was 26 years (range 4–77). Among both males and females, a large proportion were adolescents or young adults, with 42 (32%) in their 20s and 28 (21%) aged 10–19 years. Among children and the elderly, the distribution was skewed towards males: 4/5 children under 10 years of age were boys and 10/11 persons aged 60 years and over were men. At the time of reporting, the majority had mild symptoms such as fever, myalgia and arthralgia. No fatalities have been reported. Sequence analysis of viral genomes presented high similarity with dengue serotype 1 viruses circulating in South-eastern Asia.9
* Yoyogi Park visits, n = 112; non-Yoyogi Parks visits, n = 16.
Dengue virus has also been detected from mosquitoes collected in Yoyogi Park. After enhancing vector surveillance following the reporting of the initial cases, dengue virus was detected from mosquitoes captured on 3 September 2014 from 4/10 collection sites in the park.10 This finding was a first since the Tokyo Metropolitan Government began testing mosquitoes captured from 16 collection sites in the Tokyo metropolitan area in 2004. Subsequently, dengue virus was also detected from a mosquito captured in Shinjuku Gyoen, a large park 2 km from Yoyogi Park, on 19 September; however, this park was already closed on 7 September.11
Local and national public health authorities have been responding to the ongoing domestic transmission. Risk communication messages have been disseminated via the Internet and traditional means (e.g. public notices at the affected sites, newspapers, television), focusing on personal protection (reducing exposed areas of skin when outdoors and applying insect repellent) and on elimination of mosquito breeding sites. MHLW is actively providing such information12 and coordinating with local government counterparts in timely information collection. Updated guidelines for clinical management of dengue have also been disseminated. NIID, in coordination with partners, is providing technical support regarding virus testing and vector control, conducting risk assessments, epidemiological investigations and enhancing dissemination of information based on surveillance data. In addition, the Tokyo Metropolitan Government enhanced vector surveillance, increasing collection sites in Yoyogi Park,10 and also temporarily closed the park on 4 September. Vector control by adulticide application was carried out at Yoyogi and several other parks in Tokyo; investigations indicated mosquito populations in most parks were lower after vector control activities (unpublished data).
There are important limitations, and it is unknown to what degree the magnitude of the current outbreak is due to enhanced awareness, surveillance, testing and/or reporting. It is also unknown when dengue emerged locally. While enhanced surveillance activities detected cases that occurred before the initial three cases, all cases detected so far have had onset since mid-August 2014, indicating that virus introduction may have taken place fairly recently. Regardless, the confirmation of more than 100 domestically acquired dengue cases linked with a single urban park in Japan, within a period of a month, is remarkable. Another important potential limitation is ascertainment bias, such that clinically suspect cases who visited Yoyogi Park may have been more likely to be tested, as the initially reported cases were all linked to the park. Later, cases with no link began to be detected (Figure 1), indicating perhaps wider geographic circulation of the virus.
While the situation is still evolving, the detection of dengue virus-positive mosquitoes from Yoyogi Park has major public health, social and economic implications. Already, an Australian traveller who had visited Yoyogi Park has been reportedly confirmed with dengue infection in September 2014, following his return from Japan.13 The unexpected magnitude and future concerns require ongoing monitoring, risk assessment and epidemiologic and entomologic studies. As Aedes albopictus is active only until November in most of Japan, notifications of autochthonous cases should soon start to decline. However, re-entry of the virus in the following year is possible via a dengue virus-infected mosquito(es) or person(s) who are viremic upon entry into the country. As the 2020 Summer Olympics are to be held in Tokyo, there are also significant international public health implications requiring effective surveillance and clear and routine communications of findings to regional and global partners and stakeholders.
None declared.
None.
We thank the staff at local public health centres and prefectural and municipal public health institutes, notifying physicians and other public health and medical staff who have been responding to the ongoing situation. We appreciate the rapid laboratory diagnosis and reporting by the prefectural and municipal institutes of public health that have allowed for rapid assessments and response. Lastly, we would like to thank the Ministry of Health, Labour and Welfare and the Tokyo Metropolitan Government for their active response activities and timely information-sharing.
{kind=link}