
a Health Protection Service, Australian Capital Territory Health, Canberra, Australia.
b OzFoodNet, Communicable Disease Control Section, Health Protection Service, Australian Capital Territory, Canberra, Australia.
c Master of Philosophy (Applied Epidemiology) Program, National Centre for Epidemiology and Population Health, Australian National University, Canberra, Australia.
d Population Health Division, Australian Capital Territory Health Directorate and Australian National University Medical School, Australian Capital Territory, Australia.
e Department of Microbiology and Infectious Diseases, Canberra Hospital and Health Services, Canberra, Australia.
Correspondence to Ranil Appuhamy (e-mail: ranil.appuhamy@act.gov.au).
To cite this article:
Appuhamy R et al. Hepatitis E in a food handler – a rapid risk assessment to guide the public health response. Western Pacific Surveillance and Response Journal, 2014, 5(4):1–4. doi:10.5365/wpsar.2014.5.3.003
Objective: The Australian Capital Territory Health Directorate was notified of a food handler with hepatitis E virus (HEV) infection. To guide the public health response, a rapid risk assessment was undertaken to determine the risk of transmission of HEV from the infected food handler to restaurant patrons.
Method: The literature on HEV was reviewed and expert advice sought from clinical and public health specialists. This was supplemented by results of a site investigation and a case interview. The risk rating was determined to be the product of the likelihood of transmission and the consequence of the infection.
Results: The food handler was likely to have been infectious at the time he was working at the restaurant. He had handled high-risk foods, and the site inspection revealed potential opportunities for transmission. HEV is not common in Australia and it was assumed that the population was non-immune and hence susceptible to the disease. Therefore, there was a low but possible likelihood of transmission of HEV. If infected, HEV has the potential for major consequences in vulnerable populations especially among women who are pregnant. The overall level of risk was considered to be very high.
Discussion: The general public and health practitioners were alerted to enable early identification of symptoms and prompt disease management. There were no secondary cases of HEV associated with this event. In the absence of published guidelines and limited evidence, a risk assessment framework was a useful tool to inform public health decision-making.
In early 2011, the Communicable Diseases Control Section (CDC) of the Australian Capital Territory Health Directorate (ACT Health) in Canberra was notified of a food handler who was diagnosed with hepatitis E virus (HEV) infection. He had recently returned from an overseas trip to a country where there is known HEV activity and had presented to hospital with abdominal pain and jaundice. His liver function tests were abnormal (markedly elevated liver enzymes and high bilirubin) and serology showed a positive HEV IgM and a negative IgG. The clinical, epidemiological and laboratory features fit the case definition for HEV infection.1 He was admitted to the hospital where he received symptomatic treatment. He worked at a restaurant and was involved in all aspects of food preparation.
The transmission of hepatitis A virus (HAV), a very similar disease, from food handlers to restaurant patrons has been demonstrated,2,3 and national guidelines exist in Australia to guide the public health response.4 However, there is less evidence and no guidelines available to guide public health decision-making when a food handler is infected with HEV. Although HAV and HEV share similarities, there are differences in disease characteristics, transmissibility and outcome that make the applicability of HAV guidelines less useful in this scenario.
In this paper, we describe and discuss a rapid risk assessment that was undertaken to guide the public health response for managing the HEV-infected food handler. The question we sought to answer was: what was the risk of transmission of HEV from the infected food handler to patrons at the restaurant? We describe the methods and results of our rapid risk assessment and the subsequent public health actions.
To inform the risk assessment, published literature on HEV was reviewed. Additional information and expert advice was sought from specialists in the fields of public health, infectious diseases and gastroenterology. The results of a site investigation of the restaurant where the case worked, conducted by environmental health officers, and information obtained by interviewing the case also informed the risk assessment.
The risk assessment took into account the likelihood of transmission of the virus from the food handler to restaurant patrons and the consequence of the infection to determine the level of risk. The risk rating was the product of the likelihood of transmission and the consequence of the infection.
The first component of the risk assessment was to evaluate the likelihood of transmission and the potential for exposure of the restaurant patrons to the virus. The potential infectivity of the food handler, the transmissibility of the virus, the handling of high-risk foods, environmental factors that would facilitate spread of the disease and the susceptibility of the population were taken into account when assessing how likely it was that the patrons were exposed to the disease.
The infectious period of HEV is not known.5 However, virus particles have been detected in stools 14 days after the onset of jaundice and approximately four weeks after the ingestion of contaminated food or water.5 Given that the food handler worked at the restaurant up to four days before the onset of jaundice, it was very likely that he was infectious during the time that he worked there.
Transmission of HEV occurs predominantly via the fecal–oral route with contaminated water being the source of large epidemics.6 Parenteral and perinatal routes have also been implicated.6 Although person-to-person transmission is not thought to be common or to contribute significantly to morbidity in epidemics, it may occur.7,8 Opportunities described for transmission of HEV from person to person were thought to include the use of common drinking, hand-washing and eating vessels.8
The food handler was responsible for the preparation of all foods at the restaurant including raw salads that were not further cooked before being served. The food handler stated that he used gloves when preparing these foods.
Environmental health officers from ACT Health inspected the restaurant, and some deficiencies (the lack of a dedicated hand-washing facility) in the food preparation area were observed. This might have provided opportunities for transmission of the disease.
The context of the risk assessment was the ACT population. Hepatitis E is an uncommon disease in Australia (notification rates 0.1–0.2 per 100 000).9 In the ACT, from 2006 there had been only six cases of HEV notified, all overseas acquired. Similar to other notifiable diseases, it is possible that this is an underestimate due to asymptomatic cases or lack of testing; however, it was reasonable to assume that the underlying incidence is extremely low. Therefore, it was assumed that the ACT population was susceptible to HEV infection.
The next step in the risk assessment was to determine the potential consequences of infection with HEV if transmission did occur. Hepatitis E is an RNA virus, a major cause of waterborne hepatitis in tropical and subtropical countries and of sporadic disease in industrialised countries.6 Typical signs and symptoms include jaundice, anorexia, hepatomegaly, abdominal pain, nausea and vomiting and fever.6,7 Although the clinical course of HEV infection is similar to that of HAV infection, HEV has been associated with greater severity (protracted coagulopathy and cholestasis) and higher mortality.10
HEV infection can range in severity from subclinical to fulminant disease. The disease is particularly severe for those with chronic liver disease and in pregnancy where the mortality rate can be 15–20%. Other complications during pregnancy include fetal death, premature delivery or death of the infant soon after birth.6 There is no vaccine available in Australia or chemoprophylaxis for the prevention of the disease.
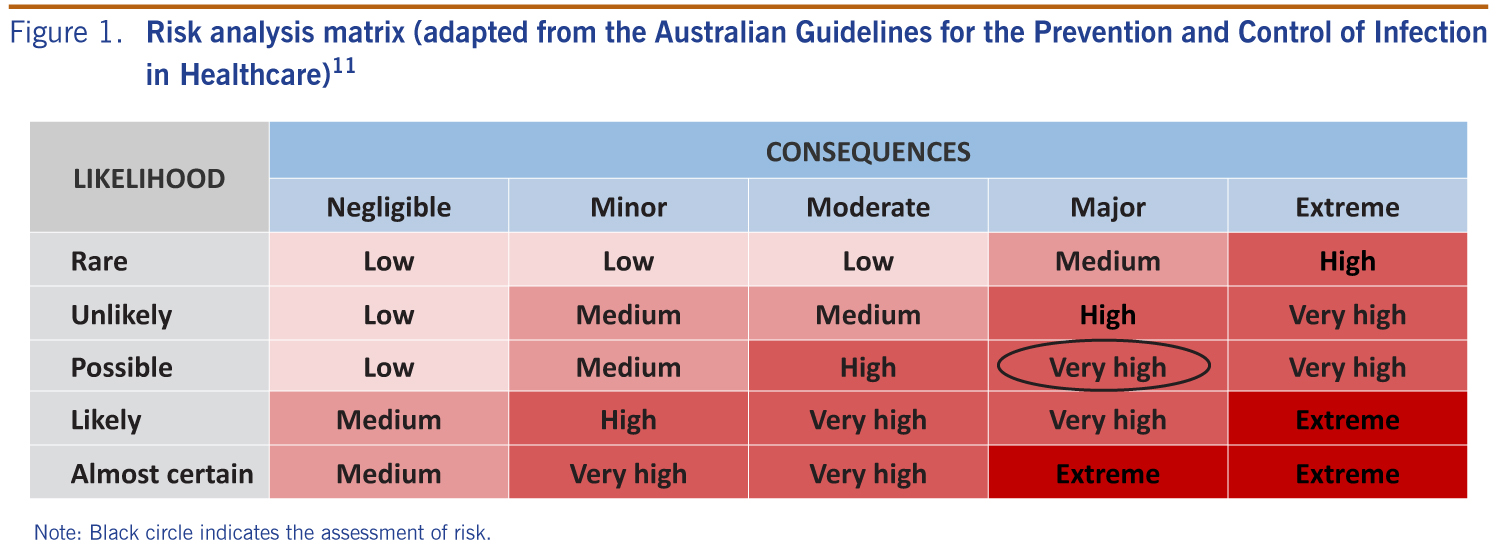
The likelihood of transmission and the consequence of the infection were assessed. It was highly likely that the food handler was infectious at the time he was working at the restaurant. He had handled high-risk (uncooked) food, and the site inspection had revealed potential opportunities for transmission of the disease. There is however limited evidence of the transmissibility of the virus, and although person-to-person transmission is not common, it may occur. The concern was that there could be transmission of the virus from the food handler to the restaurant patrons either via food or through plates or cutlery. Taking these factors into consideration, there was a low but possible likelihood of transmission. If transmission occurred however, the consequence of infection with HEV was considered to be major, especially in pregnant women and those with chronic liver disease. As there was no way to identify if there were high-risk patrons at the restaurant who had consumed meals made by the infected food handler, the overall level of risk was assessed to be very high (Figure 1).
Note: Black circle indicates the assessment of risk.
The main limitation of this risk assessment was the limited literature and guidelines on transmission of hepatitis E. With the information and evidence available, and using a precautionary approach, the recommendation of the risk assessment was to provide advice to patrons who may have eaten at the restaurant during the time the food handler had worked there while potentially infectious. The advice was that there was a small risk of acquiring HEV infection, the symptoms to be aware of and the importance of seeking early medical treatment, especially those at high risk. Given that the restaurant had no booking lists and there was no way to identify those who were at higher risk, the public was alerted by a media release and a health alert that was placed on the ACT Health website. A communicable disease information hotline was available to deal with public inquiries. A letter was sent to all general practitioners and hospital emergency departments in the ACT to alert them of this event to enable the early identification and management of cases.
The decision to name publicly the restaurant was not made lightly and done only after the careful consideration of potential risks to the public. To mitigate adverse effects to the restaurant, a sensitive communication strategy was adhered to, involving restaurant management at all stages of the investigation and public health response. This ensured full cooperation by the restaurant management.
Enhanced surveillance of HEV notifications received by ACT Health after this incident did not find any secondary hepatitis E cases that were linked to the restaurant.
Conducting a rapid risk assessment in a novel situation where limited guidance was available was a useful way to ensure evidence-based decision-making and enabled a timely public health response. This has since been used within the Communicable Diseases Control section of ACT Health for other public health issues.12 The World Health Organization has published guidelines for the rapid assessment of public health events,13 and these are expected to be a useful framework for risk assessment to inform public health decision-making. A guideline for the public health management of hepatitis E would be a useful addition to the Australian Series of National Guidelines.14
None declared.
OzFood Net is funded by the Australian Government Department of Health.
The authors wish to acknowledge the following groups for their assistance with the investigation: staff at the Communicable Diseases Control section at the ACT Health Directorate; environmental health officers at the ACT Health Protection Service; staff at the ACT Government Analytical Laboratory; staff at ACT Pathology; staff at Capital Pathology; and the management and staff of the restaurant.
{kind=link}