a National Institute of Hygiene and Epidemiology, Hanoi, Viet Nam.
b Department of Preventive Medicine, Ministry of Health, Hanoi, Viet Nam.
Correspondence to Le Quynh Mailom9@nihe.org.vn or lom9@hotmail.com).
To cite this article:
Tham CD et al. Seroprevalence survey of avian influenza A(H5N1) among live poultry market workers in northern Viet Nam, 2011. Western Pacific Surveillance and Response Journal, 2014, 5(4):21–26. doi:10.5365/wpsar.2014.5.2.006
Objective: Highly pathogenic avian influenza A(H5N1) is endemic in poultry in Viet Nam. The country has experienced the third highest number of human infections with influenza A(H5N1) in the world. A study in Hanoi in 2001, before the epizootic that was identified in 2003, found influenza A(H5N1) specific antibodies in 4% of poultry market workers (PMWs). We conducted a seroprevalence survey to determine the seroprevalence of antibodies to influenza A(H5N1) among PMWs in Hanoi, Thaibinh and Thanhhoa provinces.
Methods: We selected PMWs from five markets, interviewed them and collected blood samples. These were then tested using a horse haemagglutination inhibition assay and a microneutralization assay with all three clades of influenza A(H5N1) viruses that have circulated in Viet Nam since 2004.
Results: The overall seroprevalence was 6.1% (95% confidence interval: 4.6–8.3). The highest proportion (7.2%) was found in PMWs in Hanoi, and the majority of seropositive subjects (70.3%) were slaughterers or sellers of poultry.
Discussion: The continued circulation and evolution of influenza A(H5N1) requires comprehensive surveillance of both human and animal sites throughout the country with follow-up studies on PMWs to estimate the risk of avian–human transmission of influenza A(H5N1) in Viet Nam.
Highly pathogenic avian influenza A(H5N1) viruses re-emerged in south-eastern Asia in 2003, and these viruses continue to circulate widely among domestic poultry in the region.1 Numerous outbreaks of influenza A(H5N1) viruses have occurred, with limited transmission to humans and as of yet unclear potential for sustained human-to-human transmission. However, the continuing evolution and genetic diversification of influenza A(H5N1) viruses is worrying since as few as four amino acid changes are necessary to render the viruses transmissible between ferrets, reinforcing the ongoing pandemic threat from these viruses.2–4
In Viet Nam, as of July 2014, there have been 127 human cases of influenza A(H5N1) infection with 63 deaths. Since the influenza A(H5N1) epizootic first began in Viet Nam in 2003, three main clades have circulated and been associated with human infections (clades 1, 2.3.4 and 2.3.2.1).1,5 Contact with sick or dead poultry has been consistently identified as a risk factor for human influenza A(H5N1) infection, and live poultry markets have been shown to be important locations for amplifying influenza A(H5N1) virus transmission.6,7 An antibody seroprevalence study conducted among 200 poultry market workers (PMWs) in Hanoi in 2001 detected antibodies against influenza A(H5N1) virus in 4% of subjects,8 suggesting that there were human infections with influenza A(H5N1) before the first case was officially confirmed.9 In addition, subclinical, asymptomatic or mildly symptomatic cases were reported during outbreak investigations.9–11 Similarly, seroprevalence studies have been conducted in Thailand, Cambodia and Indonesia as part of comprehensive outbreak investigations to evaluate key clinical, epidemiological and serological aspects related to human influenza A(H5N1) infections.
To assess if exposure to influenza A(H5N1) viruses among PMWs has changed over this period, we conducted a seroprevalence study among PMWs in three provinces of northern Viet Nam in 2011.
A cross-sectional seroprevelance study was conducted among adult workers at five markets selling live poulty in the provinces of Hanoi, Thaibinh and Thanhhoa in northern Viet Nam. Sample size was estimated based on a reported seropositive rate of 4% among PMWs in Hanoi in 2001,9 with a confidence level of 95% and 1.5% confidence interval (CI) ranging from 2.45% to 5.55%. To account for uncooperative participants and unqualified samples, a total of 600 samples were estimated for this study.
Live poultry markets were eligible if their regular number of poultry sellers exceeded 100 individuals and they were located in a large city with a history of laboratory-confirmed cases of human influenza A(H5N1) infection. With the support of local government, 11 poultry markets were nominated. Five markets from three provinces were then randomly selected. Individual participants were eligible if they were aged 18 years or older, currently a trader or slaughterer of live poultry (including waterfowl) and had worked for a minimum of six months in a live poultry market. We enrolled subjects, sampling market to market, until the required number of participants were recruited.
A questionnaire was used to collect information on demographic characteristics and potential occupational risk factors for exposures to influenza A(H5N1). The variables of age, gender, education history, medical history, province of occupation and poultry-related occupational risk exposures were collected. All participants were interviewed face to face. Data were entered into EpiData v3.1 and analysed using STATA v11. Frequencies were calculated with a 95% CI. Seroprevalence among workers was compared across the potential variables using the Pearson’s chi-squared test or using Fisher Exact test if any observed value was less than five. Mean values were compared using a t-test to assess whether any differences observed were statistically significant at 95% CI.
All participants were asked to provide 5 ml of venous blood to determine serum antibody concentrations against influenza A(H5N1) viruses. Samples were transported by car in ice boxes at 4 °C to the National Influenza Center at the National Institute of Hygiene and Epidemiology (NIHE) in Hanoi within 24 to 48 hours of collection. Sera was used after centrifugation of whole blood at NIHE (2500 rpm for 15 minutes) and were aliquoted and stored at −70 °C until testing.
The participants’ sera were tested for antibodies to influenza A(H5N1) viruses by horse haemagglutination inhibition assay (HHI) and microneutralization assay (MN) at NIHE following the US Centers for Disease Control and Prevention protocols. All three clades of influenza A(H5N1) virus that have cirulated in Viet Nam since 2004 were used because the antigenic diversity of influenza A(H5N1) viruses may alter the sensitivity of assays to detect strain-specific antibodies. The influenza A(H5N1) viruses used were cultured from selected Vietnamese patients with positive reverse transcription polymerase chain reaction (RT–PCR) assays for clade 1 in 2005 (A/Viet Nam/HN30408/2005), clade 2.3.4 in 2007 (A/Viet Nam/HN31244/2007) and clade 2.3.2.1 in 2011 (A/Viet Nam/CM32/2011). Due to the unknown pathogenic potential of avian/human viruses, all tests involving live virus were conducted in animal-biosafety level 3 and biosafety level 3 laboratories.
The HHI assays were performed as described elsewhere12 using reference antisera treated with receptor-destroying enzyme before testing. Serum samples were tested at a starting dilution of 1:10 using eight haemagglutinating units of virus and 1% volume/volume horse erythrocytes. All viruses were inactivated by 1% β propiolactone before use. HHI titres were read up to 60 minutes after the addition of erythrocytes and reported as the reciprocal of the highest serum dilution causing complete inhibition of agglutination. Results were accepted if negative sera and horse erythrocytes cell controls provided the correct non-agglutinated pattern. Samples that were negative by HHI assay in the lowest dilution (1:10) and samples resulting in HHI titres ≥40 were tested against the three influenza A(H5N1) clades by MN assay. MN assays were performed according to World Health Organization (WHO) protocols, using 100 x TCID50 of live viruses as above.12,13 Virus was incubated with twofold serial dilutions of sera starting at 1:10 and then incubated with MDCK cells (Madin-Darby canine kidney cells-American Type Culture Collection-ATCC, United States of America) overnight before virus quantitation by enzyme-linked immunosorbent assay (ELISA) to detect influenza nucleoprotein. The titre was reported as the reciprocal of the highest dilution that reduced infection by at least 50%.
The WHO seropositive criteria for an influenza A(H5N1)-confirmed case in single serum collected at day 14 or later of symptom onset is an HHI titre >160 and an MN titre >80.14 However, this is not appropriate for seroprevalence studies as the participants are not suspected influenza A(H5N1) patients. In fact, the Consortium for the Standardization of Influenza Seroepidemiology has not yet devised positive criteria for influenza A(H5N1) assays.7 For our study, a sample was considered seropositive for influenza A(H5N1) virus antibody if an HHI titre ≥80 and an MN titre ≥20 were obtained in duplicate HHI and MN tests with any influenza A(H5N1) clade. The clades of seropositive samples were classified based on the highest antibody titre by comparison between three clades.13
The study protocol was approved by the institutional review board of NIHE. Participation was voluntary and all subjects provided written informed consent to participate in the study.
A serum sample was collected from 607 PMWs during four months (September to December 2011). Of those, 305 samples (50.3%) were from Hanoi, 169 samples (27.8%) from Thaibinh and 133 samples (21.9%) from Thanhhoa.The mean duration of working in a live poultry market was 7.7 years (95% CI: 7.1–8.2) and ranged from six months to 36 years.
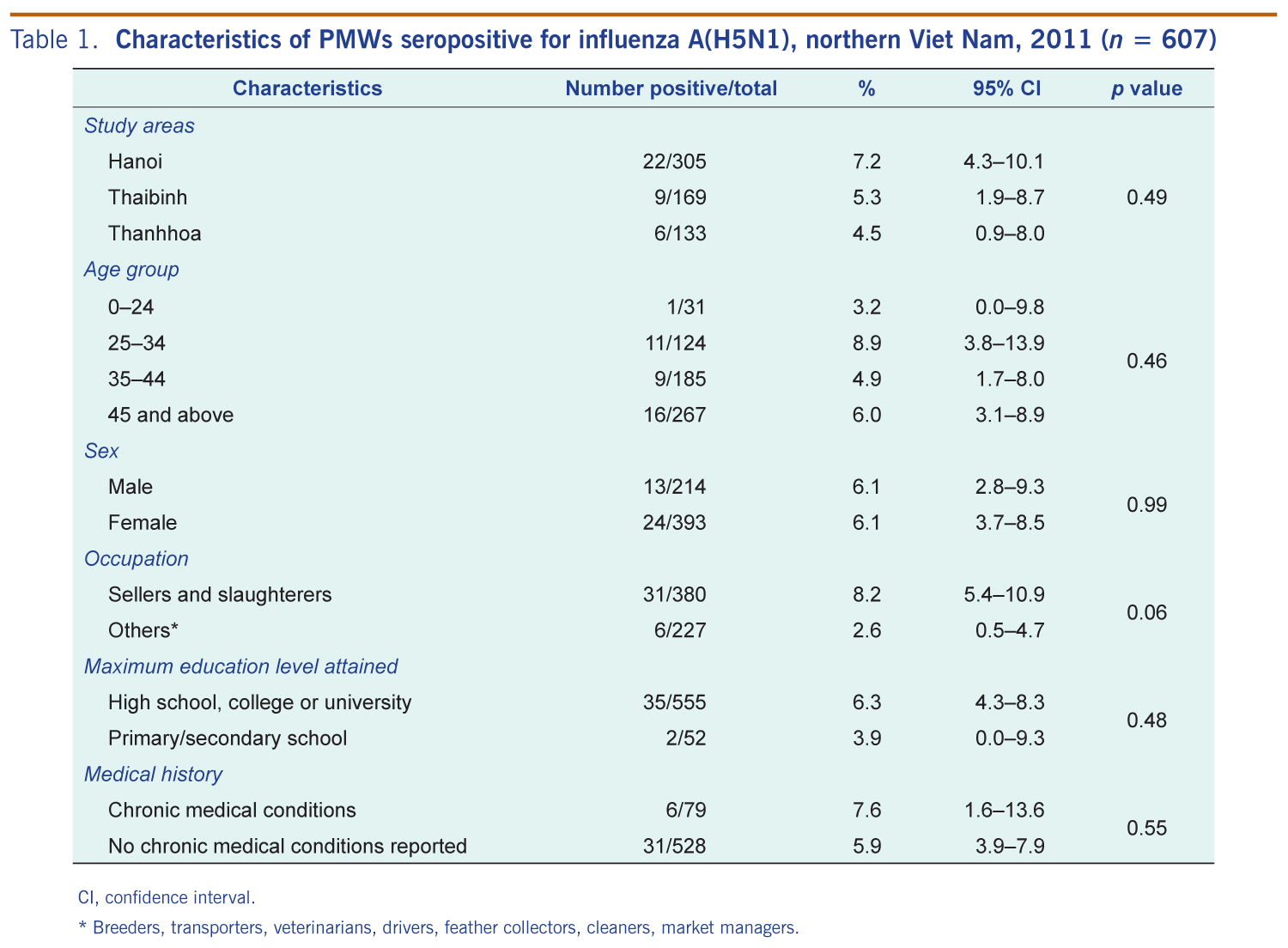
The mean age of participants was 42.3 years (95% CI: 41.4–43.2) with a range of 18 to 74 years, and 214 (35.3%) were male. Almost two thirds (62.6%) reported that they were sellers or slaughterers of live poultry, with 37.4% being breeders, transporters and others (veterinarians, drivers, feather collectors, cleaners and market managers). A total of 79 (13.1%) participants reported having a chronic medical condition (hypertension, diabetes, hepatitis). There were 555 (91.4%) participants who had an education level to high-school standard or higher (Table 1).
CI, confidence interval.
* Breeders, transporters, veterinarians, feather collectors, cleaners and market managers.
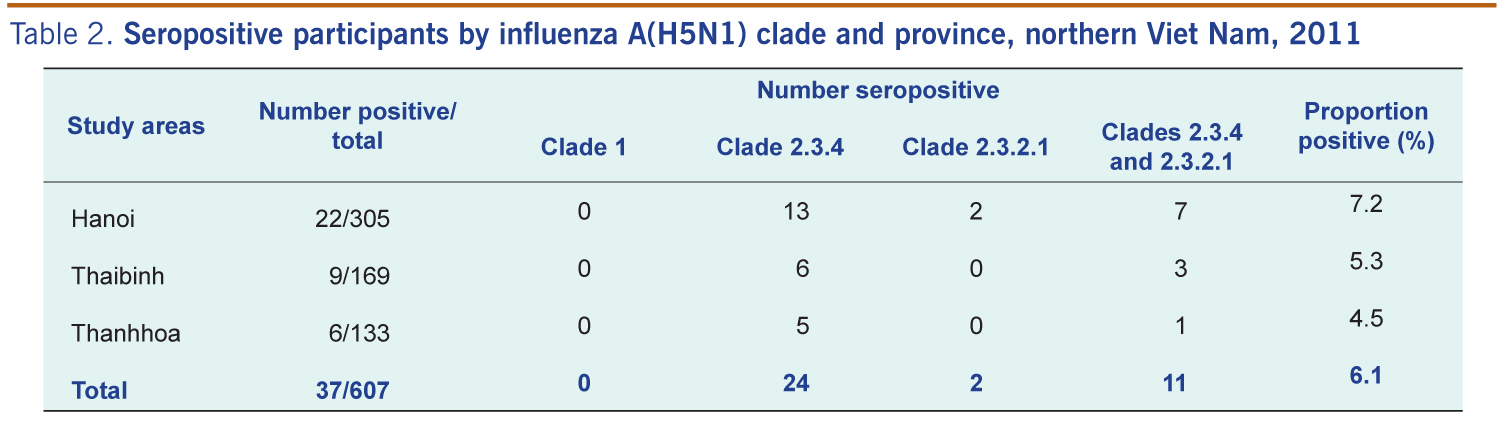
There were 37 participants seropositive for (21.9%), giving an overall seropositive rate of 6.1%; (95% CI: 4.6–8.3). Of the 37 seropositive samples, 24 were seropositive to clade 2.3.4, two were seropositive to clade 2.3.2.1 and 11 were seropositive to both (Table 2). By province, the proportion of seropositives was 7.2% (95% CI: 4.3–10.1) for Hanoi, 5.3% (95% CI: 1.9–8.7) for Thaibinh and 4.5% (95% CI: 0.9–8.0) for Thanhhoa; these differences were not statistically significant (P = 0.49) (Table 1).
By age, the highest proportion of seropositivity was in the 25 to 34 year old age group (8.9%, 95%CI: 3.8–13.9) although there was no statistically significant difference across the four age groups (P = 0.46). There was also no statistically significant difference by sex (P = 0.99), education level (P = 0.48) or chronic medical condition (P = 0.55) (Table 1). By occupation, the proportion seropositive was higher in slaughterers and sellers compared with all others but this was not significant (8.2% compared with 2.6%, P = 0.06) (Table 1).
Our study identified 37 (6.1%) PMWs seropositive for influenza A(H5N1) clade 2.3.4 and clade 2.3.2.1 viruses; these clades were predominant in northern Viet Nam from 2005 to 2013.15–17 While clade 1 also circulated in Viet Nam from 2003 to mid-2005,18 no PMWs seropositive for clade 1 was identified in our study. This was unexpected as some of the workers in our study would have been working when this clade was circulating. Our sample of PMWs were from Hanoi, Thaibinh and Thanhhoa where a large number of human influenza A(H5N1) infections have been reported since 2004.6,18 Although studies conducted in 2004 in Viet Nam and Thailand did not identify contact with healthy poultry as a risk factor of influenza A(H5N1) exposure,6 a study among PMWs in Hanoi in 2001 showed a 4% seroprevalence of influenza A(H5N1) clade A/Goose/Viet Nam/113/2001.8 Circulation of influenza A(H5N1) in healthy ducks in Viet Nam1 demonstrated the possible risk of influenza A(H5N1) infection among persons exposed to healthy poultry in Viet Nam.
In our study population, the working duration of PMWs was an average of 7.2 years (range from six months to 36 years). It is possible then that some of the workers in the study may not have been exposed to the clade 1 virus. That 11 participants were positive for both clade 2.3.4 and clade 2.3.2.1 may have been due to cross-reactivity, coinfections or reinfections since co-circulation of these clades was identified in 2010.12
We found no statistically significant difference in the proportion of seropositive PMWs between the three different geographical study areas, which suggests the working conditions or occupational habits of PMWs are similar in these areas. Our study found a higher seropositive rate among PMWs in Hanoi compared to a seroprevalence study conducted in 2001 (7.2% compared with 4.0%), which might be due to the spread of influenza A(H5N1) in Viet Nam occurring after late 2003.15 We found a higher seropositive proportion in slaughterers and sellers compared with the other occupational groups; this is consistent with studies from China, Thailand and Bangladesh that showed that people who work directly with poultry are more likely to have been exposed to avian influenza A(H5N1).9,15 A 2010 survey of live bird markets in Viet Nam found 3.3% of poultry samples tested were positive for influenza A(H5N1) by RT–PCR (personal communication: John Weaver, Viet Nam Avian and Human Influenza Control and Preparedness Project). A survey of healthy ducks in northern Viet Nam in 2006 concluded that while influenza A(H5N1) viruses were not detected in any throat or cloacal swabs, serological analyses suggested that ducks were infected with influenza A(H5N1) viruses in the absence of any recognized outbreak.11 That our study demonstrated seropositivity to influenza A(H5N1) viruses in all groups of poultry workers suggests that preventive measures such as personal protective equipment and vaccination for PMWs are needed.
Our criteria for seropositivity were modified from the WHO criteria for detection of influenza A(H5N1) infection by serological testing. The WHO criteria are for confirming suspected cases of influenza A(H5N1) and seems not to be practical or sensitive enough for serological surveillance studies since antibody titres against influenza A(H5N1) begin to decrease six to 12 months after exposure and may disappear.20 We selected a seropositive cutoff titre of HHI ≥80 and MN titre ≥20 since MN’s sensitivity is reduced (less than 80%) for adults21 and all PMWs enrolled in our study were at least 18 years old. Previous comparisons have shown that horse red blood cells HHI assays have high reliability and good agreement with MN assays.22 Using our cutoff titre might have resulted in an overestimate of the seroprevalence and these cutoffs should be tested with more seroprevalence studies in control populations where influenza A(H5N1) has not yet been detected. Further development of standard criteria for prevalence of antibodies against influenza A(H5N1) is needed for future studies.7
There may have been some misclassification in the reporting of occupational exposures in this study as PMWs may not have accurately recalled these exposures over a long period of time. It is also possible that participants may have had more than one poultry-related occupation during their exposure period. The results of our study, that 6.1% of PMWs in northern Viet Nam were seropositive for influenza A(H5N1), may not be representative of all PMWs in Viet Nam. Collecting further epidemiological information (using personal protective equipment; contact duration, influenza vaccination) may also be useful. The results of our study would be more convincing if control groups (vegetable, fruit and seafood sellers working in the same market with PMWs) were included or a follow-up study was conducted.
Despite these limitations, our study has shown that 6.1% of PMWs in northern Viet Nam are seropositive for influenza A(H5N1). The continued circulation and evolution of influenza A(H5N1) requires comprehensive surveillance of both human and animal sites throughout the country with follow-up studies on PMWs to estimate the risk of avian–human transmission of influenza A(H5N1) viruses in Viet Nam.
None declared.
None.
We thank the Preventive Medical Center (PMC) of Hanoi, PMC Thaibinh and PMC Thanhhoa. The study was funded by Viet Nam Avian and Human Influenza Control and Preparedness Project, Ministry of Health, Viet Nam.
We would like to thank David Dennis, former officer, Centers for Disease Control and Prevention, Viet Nam for editing this manuscript.
{kind=link}
{kind=link}