a Emerging Disease Surveillance and Response, Division of Health Security and Emergencies, World Health Organization Regional Office for the Western Pacific, Manila, Philippines.
b Emerging Disease Surveillance and Response, World Health Organization China Office, Beijing, China.
* Members of the World Health Organization Event Management Team: Nyka Alexander, Jang Hwan Bae, Joy Rivaca Caminade, Erica Dueger, Xavier Dufrenot, Norikasu Isoda, Frank Konings, Chin-Kei Lee, Ailan Li, Michelle McPherson, Satoko Otsu, Karl Schenkel and Huu Thuan Vo.
Correspondence to Yuzo Arima (e-mail:arimay@wpro.who.int).
To cite this article:
Arima Y et al., World Health Organization Event Management Team. Human infections with avian influenza A(H7N9) virus in China: preliminary assessments of the age and sex distribution. Western Pacific Surveillance and Response Journal, 2013, 4(2):1–3. doi:10.5365/wpsar.2013.4.2.005
Since 31 March 2013, the government of China has been notifying the World Health Organization (WHO) of human infections with the avian influenza A(H7N9) virus,1 as mandated by the International Health Regulations (2005).2 While human infections with other subgroups of H7 influenza viruses (e.g. H7N2, H7N3, and H7N7) have previously been reported,3 the current event in China is of historical significance as it is the first time that A(H7N9) viruses have been detected among humans and the first time that a low pathogenic avian influenza virus is being associated with human fatalities.4 In this rapidly evolving situation, both detailed epidemiologic and clinical data from reported cases are limited—making assessments challenging—however, some key questions have arisen from the available data. Age and sex data, as one of the first and most readily available data, may be an important proxy for gender-specific behaviours/conditions and an entry point for response.5,6 Here, we describe the age and sex distribution of the human cases of avian influenza A(H7N9) to better inform risk assessments and potential next steps.
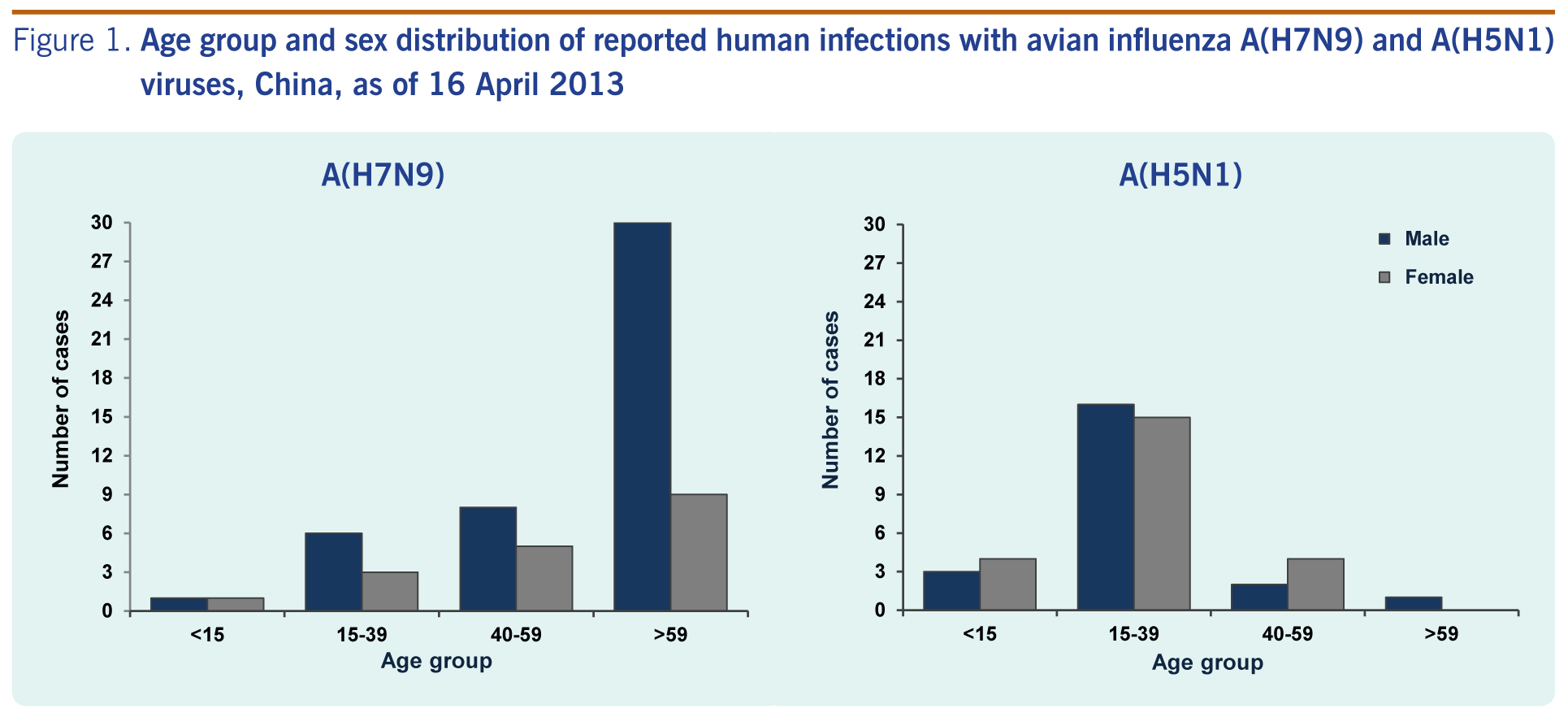
Between 31 March and 16 April 2013, there were 63 reported cases of avian influenza A(H7N9). The median age was 64 years (range 4–87), and 45 cases (71%) were male. Notably, 39 of the 63 cases (62%) were ≥ 60 years of age. When stratified by age and sex, elderly men were the most affected demographic group (Figure 1). This is different to the Chinese population which has a large proportion of young and middle-aged adults and a greater number of women among the elderly.7 Although the case fatality rate (CFR) in all males at 22% (10/45) was similar to females at 22% (4/18), when restricted to elderly cases ≥ 60 years of age, the CFR in males is 20% (6/30) compared to no deaths in females (0/9). The case distribution of current avian influenza A(H7N9) cases is also different to reported avian influenza A(H5N1) cases in China (N=45), where the majority were young working age adults (median: 26 years; range 2–62), with no difference in gender (Figure 1).8 Hence, the question naturally arises – why are we seeing the current age and sex distribution, and what key questions can we ask to allow public health practitioners to respond in an efficient and effective manner?
Three main reasons may be considered for the current case distribution: (1) differential exposure between males and females due to gender-associated practices and norms; (2) biological differences between males and females in the clinical course post exposure/infection; and (3) differential healthcare-seeking/access behaviour between male and females, i.e. surveillance/detection bias.
Determining whether the current distribution is due to differential exposures is difficult to assess. The same is true with many other field investigations of acute outbreaks due to the lack of detailed case-based exposure information. Despite this, limited information among current cases point to poultry-related exposures, such as live bird markets (LBMs) as a potential risk factor.9 LBMs have been the primary site where avian influenza A(H7N9) virus has been detected in poultry and environmental samples in the affected areas,9 although age- and sex-specific LBM visit patterns are unknown.Elderly Chinese men are well-known to be hobbyists of “walking” ornamental pet songbirds and take frequent and extended walks with their caged birds, congregating together in parks.10 As the source and mode of infection remain unknown, control and prevention efforts are difficult. A better understanding of the social norms and behaviours among elderly Chinese men in affected areas may better guide us in the investigation (e.g. by identifying hypotheses for case-control studies).
Biological characteristics particular to elderly men may also be a possible explanation for the observed age and sex distribution. A defining feature of seasonal influenza is its severe morbidity and mortality among the elderly, due to higher biological susceptibility to severe outcomes from influenza infection among this age group.11,12 While poultry exposure appears to be a common risk factor in the current event, the age distribution among reported cases also raises the question why so few young adults (i.e. those of working age exposured to poultry as vendors/LBM workers/breeders/transporters) have been reported. This not only suggests greater exposure among elderly men but also a possible greater biological susceptibility to more severe outcomes. Among the elderly, the number of cases and the CFR is higher among men relative to women (although this may be a function of dose response due to greater or more frequent exposure). While serologic investigations among close contacts and other subpopulations in the area will assist with our understanding regarding the clinical spectrum of this infection, information regarding smoking, underlying medical conditions and other risk factors among the current case series would help to elucidate some of these issues.
Healthcare-seeking behaviour and access also need to be considered as an explanatory factor. If elderly men are more likely to access healthcare, be detected or reported, surveillance bias may occur such that the distribution of the reported cases does not reflect the underlying distribution of disease occurrence in the population. However, given the high severity among the majority of the reported cases to date, the current high awareness level in both the public and the healthcare community and the nation-wide implementation of enhanced influenza-like illness and severe acute respiratory illness surveillance activities, such an artefact where elderly men are being overly selected seems unlikely.
At this time, it is clear that there are more questions than answers. Still, based on the basic age and sex distribution, we identify several critical questions and options to guide the ongoing investigation:
In these situations, it is easy to dismiss preliminary epidemiologic assessments as being too low in numbers or with too few variables of interest. Clearly, there is a need for further case-based information, such as zoonotic exposures and underlying medical conditions. However, for public health workers engaged in rapid response to acute events, it is essential to operate as observational scientists and assess available information to help formulate next steps. Following age and sex distributions closely over time may detect important changes in the epidemiology of this virus and with better understanding, high-risk populations, targeted interventions (e.g. gender-specific risk communication messages), prevention and control measures (e.g. vaccination) and treatment options (e.g. antivirals) may be identified. While this brief and rapid communication cannot offer answers, we hope that public health practitioners involved in such response–at various capacities around the world–may consider these key concerns and questions to help counter against not only the current virus but other emerging infectious threats.
None declared.
None.
{kind=link}