a Infectious Diseases Office, National Center for Disease Prevention and Control, Department of Health, Manila, Philippines.
b United States Agency for International Development’s (USAID) Systems for Improved Access to Pharmaceuticals and Services (SIAPS) Program, Quezon City, Philippines.
Correspondence to Anna Marie Celina Garfin (e-mail:garfinamc@yahoo.com).
To cite this article:
Vianzon R et al. The tuberculosis profile of the Philippines, 2003–2011: advancing DOTS and beyond. Western Pacific Surveillance and Response Journal, 2013, 4(2):11–16. doi:10.5365/wpsar.2012.3.4.022
The Philippines is one of the highest tuberculosis (TB) burden countries in the world with nationwide coverage of directly observed treatment, short-course (DOTS) achieved in 2003. This study reports on the National TB Control Programme (NTP) surveillance data for the period 2003 to 2011. During this period, the number of TB symptomatics examined increased by 82% with 94% completing the required three diagnostic sputum microscopy examinations. Of the 1 379 390 cases diagnosed and given TB treatment, 98.9% were pulmonary TB cases. Of these, 54.9% were new smear-positive cases, 39.3% new smear-negative cases and 4.7% were cases previously treated. From 2008 to 2011, 50 030 TB cases were reported by non-NTP providers. Annual treatment success rates were over 85% with an average of 90%; the annual cure rates had an eight-year average of 82.1%. These surveillance data represent NTP priorities – the large proportion of smear-positive cases reflected the country’s priority to treat highly infectious cases to cut the chain of transmission. The performance trend suggests that the Philippines is likely to achieve Millennium Development Goals and Stop TB targets before 2015.
The Philippines is an archipelago of more than 7107 islands with an area of 300 000 km2 in south-eastern Asia. The country is divided into 17 administrative regions with 81 provinces, 136 cities including 16 highly urbanized centres, 1495 municipalities and 42 008 barangays.1 The population of the Philippines was 92.3 million in 2010 with 33.4% aged between zero and 14 years, 62.3% in the working age group of 15–64 years, and 4.3% being 65 years and older.2 Poverty incidence in the population was 26.5% in 2009.3
Tuberculosis (TB) is the sixth leading cause of morbidity and mortality in the Philippines; the country is ninth out of the 22 highest TB-burden countries in the world and has one of the highest burdens of multidrug-resistant TB. Directly observed treatment, short-course (DOTS)4 strategy for TB control commenced in 1997 and nationwide coverage was achieved in 2003.5 The prevalence of TB in 2007 was 2.0 per 1000 for smear-positive TB and 4.7 per 1000 for culture-positive TB. Compared with 1997, there was a 28% and 38% decline in prevalence for smear-positive and culture-positive TB, respectively.6
The National TB Control Programme (NTP) is managed by a central team at the National Center for Disease Prevention and Control of the Department of Health.4 This team develops policies and plans and provides technical guidance to regional and provincial/city-level NTP management teams, overseeing the implementation of the programme at the municipal and barangay levels based on NTP policies and standards.
Under NTP, TB control services are provided mainly through public primary health care facilities (also called DOTS facilities) operated by local government units in a devolved set-up. There are additional DOTS facilities within the NTP’s network of service providers that either refer diagnosed TB patients for treatment or directly provide TB treatment services using DOTS strategy. These include private outpatient clinics; public and private primary, secondary and tertiary care hospitals; workplaces; clinics under faith-based organizations and community-based nongovernmental organizations (NGOs); and public institutions such as military facilities, jails and prisons. The NTP has also established public–public and public–private partnerships for TB control consisting of public non-NTP providers such as public hospitals, public medical colleges, prisons/detention centres and military facilities; private DOT providers include private physicians, private hospitals, private clinics, private workplaces and NGOs. Nationwide expansion of TB testing in children has been part of NTP since 2005,7 while the programmatic management of drug-resistant TB was mainstreamed into NTP starting in 2008.8
The NTP surveillance system is based on the standardized recording and reporting system used in all DOTS facilities under the NTP network of providers. Reports from rural health units, health centres and other DOTS providers include data for laboratory, case finding and case holding activities. These are reported quarterly and annually to the provincial or city health offices on paper-based, standardized forms. The provincial or city health offices then consolidate these paper-based reports and convert them into an electronic format (in tabular form using Microsoft Excel or Word). These are then forwarded to the respective regional health offices for consolidation and further analysis. The regional electronic-based reports are then forwarded to the central NTP team at the Department of Health.
Modernization of the TB registry was initiated in 2005 with the launching of the electronic TB registry in two regions (National Capital Region and CHD III Central Luzon). However, the initiative was discontinued in 2010 and was replaced by the Integrated TB Information System in 2011. This system is being implemented in phases and is currently used in selected facilities in four of the country’s 17 regions including South Luzon, National Capital Region, Central Luzon and Western Visayas.
The objective of this report is to provide a national summary of TB cases reported to the NTP surveillance system from 2003 to 2011.
Data submitted to the central NTP team for the nine-year period 2003 to 2011 were consolidated and summarized. Descriptive statistics were used to analyse the data. Treatment outcome data are for 2003 to 2010 only; 2011 data are not yet complete and not included in the report.
As case finding and treatment outcome data for drug-resistant TB are not fully integrated into the system, they are not included in this report. Data for pulmonary TB (PTB) cases previously treated were disaggregated by case classification starting only in 2008 and are only reported for 2008 to 2011.
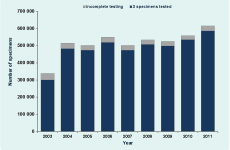
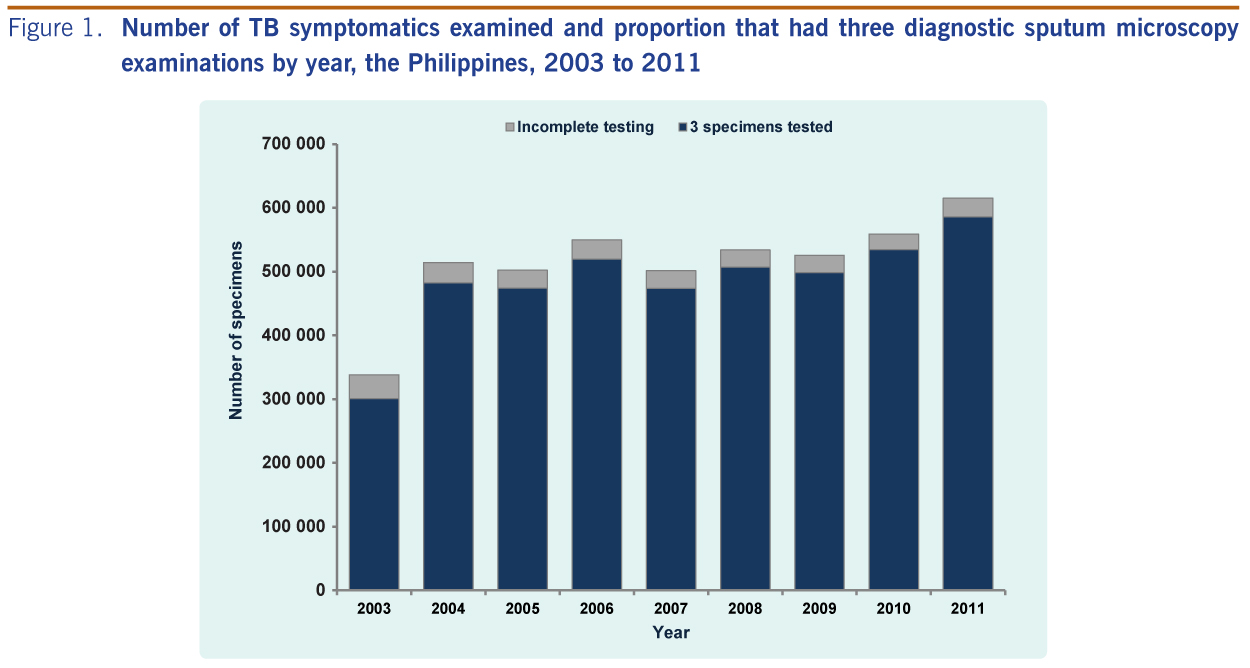
From 2003 to 2011, a total of 4 638 939 TB symptomatics were examined with sputum smear microscopy (Figure 1). On average, 94% of TB symptomatics completed the required three diagnostic sputum microscopy examinations each year. Compared to 2003, the number of TB symptomatics examined increased by 82% in 2011.
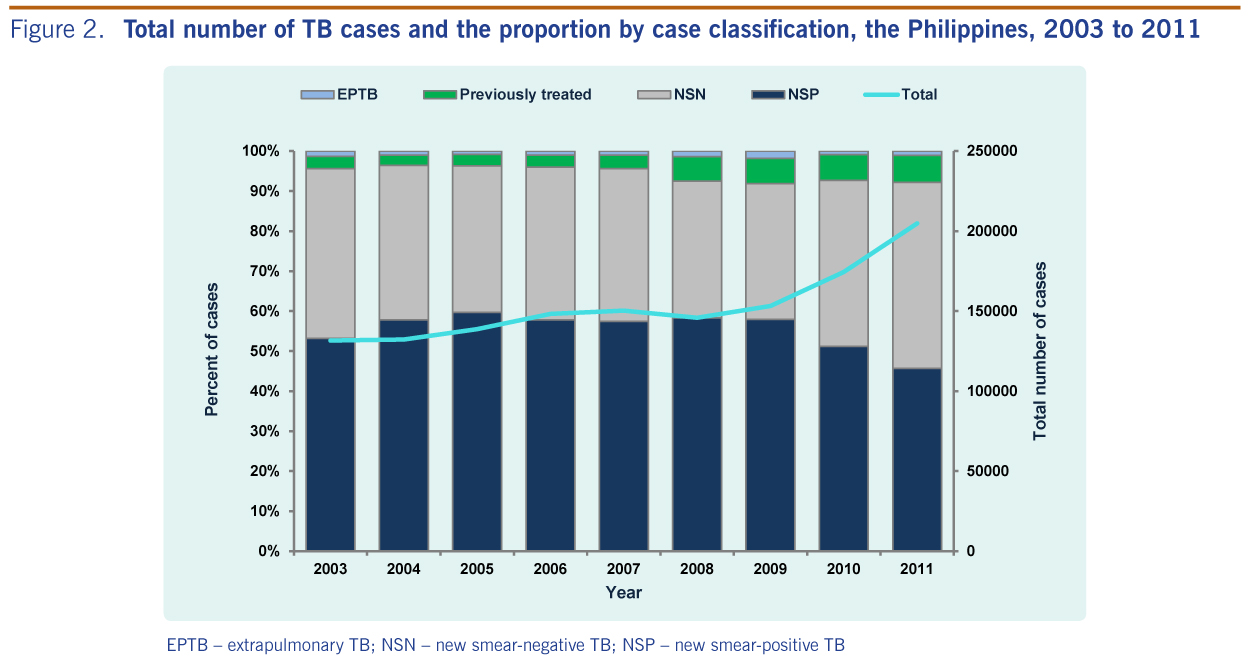
From these, a total of 1 379 390 cases of TB all forms were diagnosed and given TB treatment from 2003 to 2011. PTB comprised 98.9% of all TB cases notified; extra-pulmonary TB (EPTB) made up the remaining 1.1%. The nine-year average proportions of PTB cases are disaggregated as follows: new smear-positive, 54.9%; new smear-negative, 39.3%; and cases previously treated, 4.7% (Figure 2). Compared to 2003, the number of new smear-positive PTB cases increased by 34% in 2011; new smear-negative PTB cases increased by 70%.
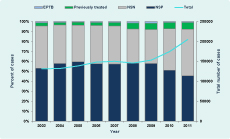
EPTB – extrapulmonary TB; NSN – new smear-negative TB; NSP – new smear-positive TB
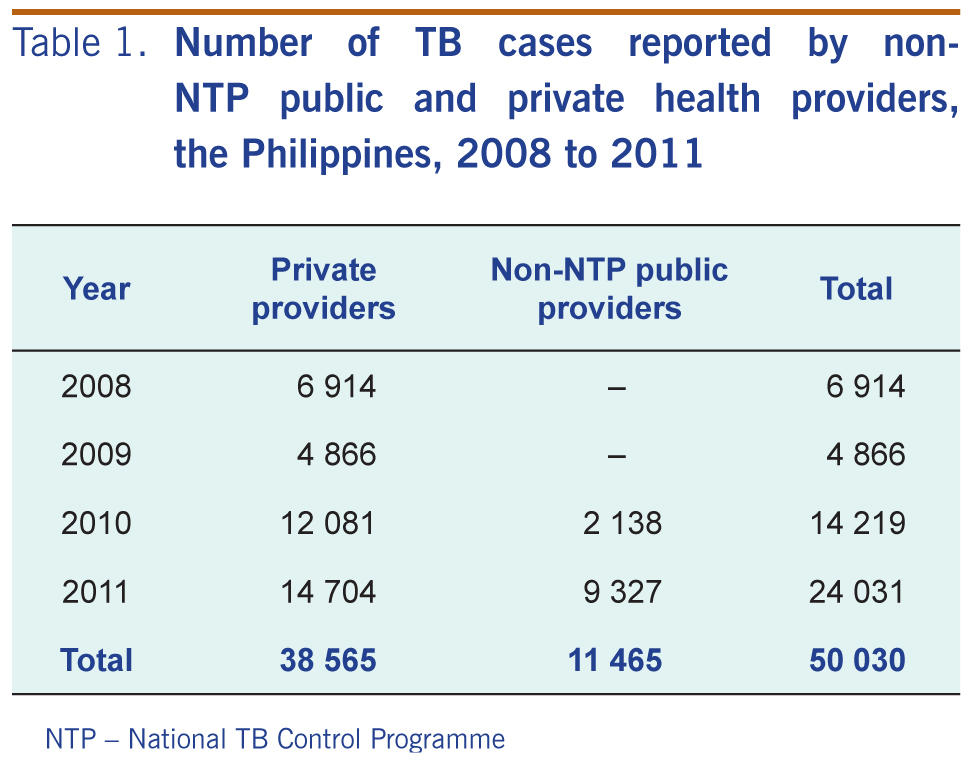
From 2008 to 2011, a total of 50 030 TB cases were reported by non-NTP providers – 7.4% of total cases reported to NTP in this time (Table 1). Most of these were from the private sector (38 565, 77.1%); 11 465 were from public partners (22.9% from 2010 to 2011 only).
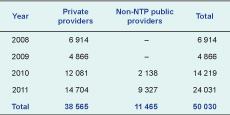
NTP – National TB Control Programme
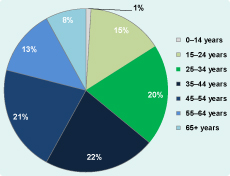
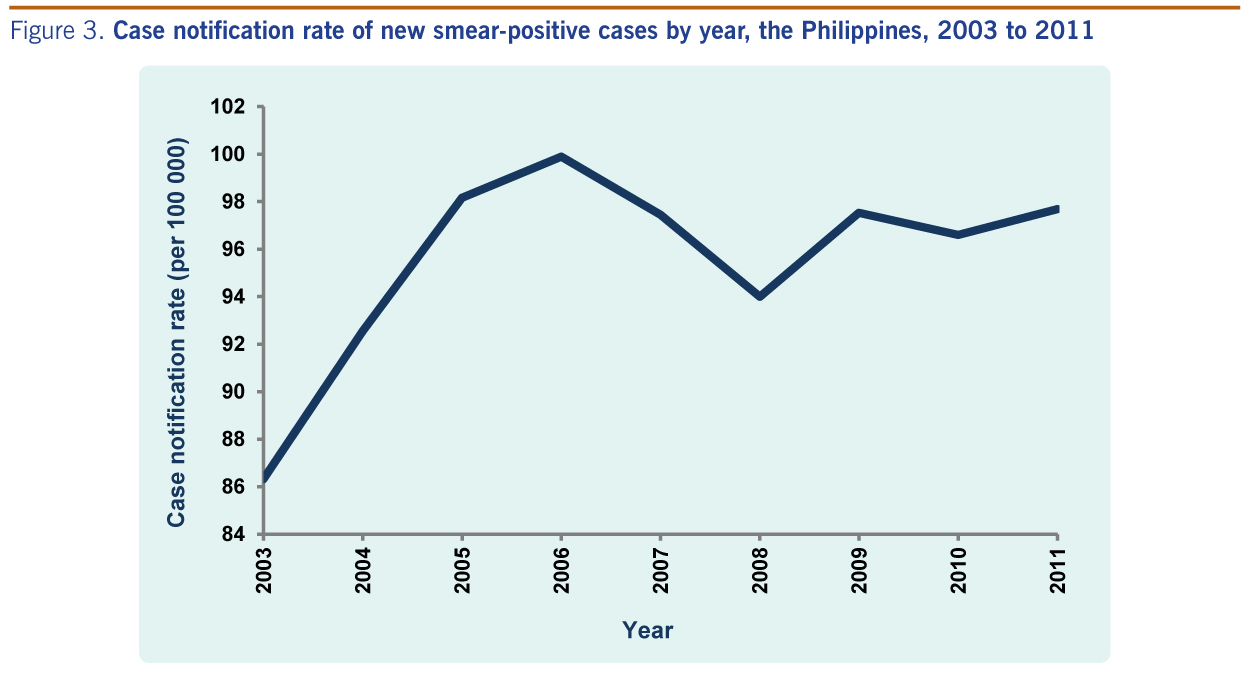
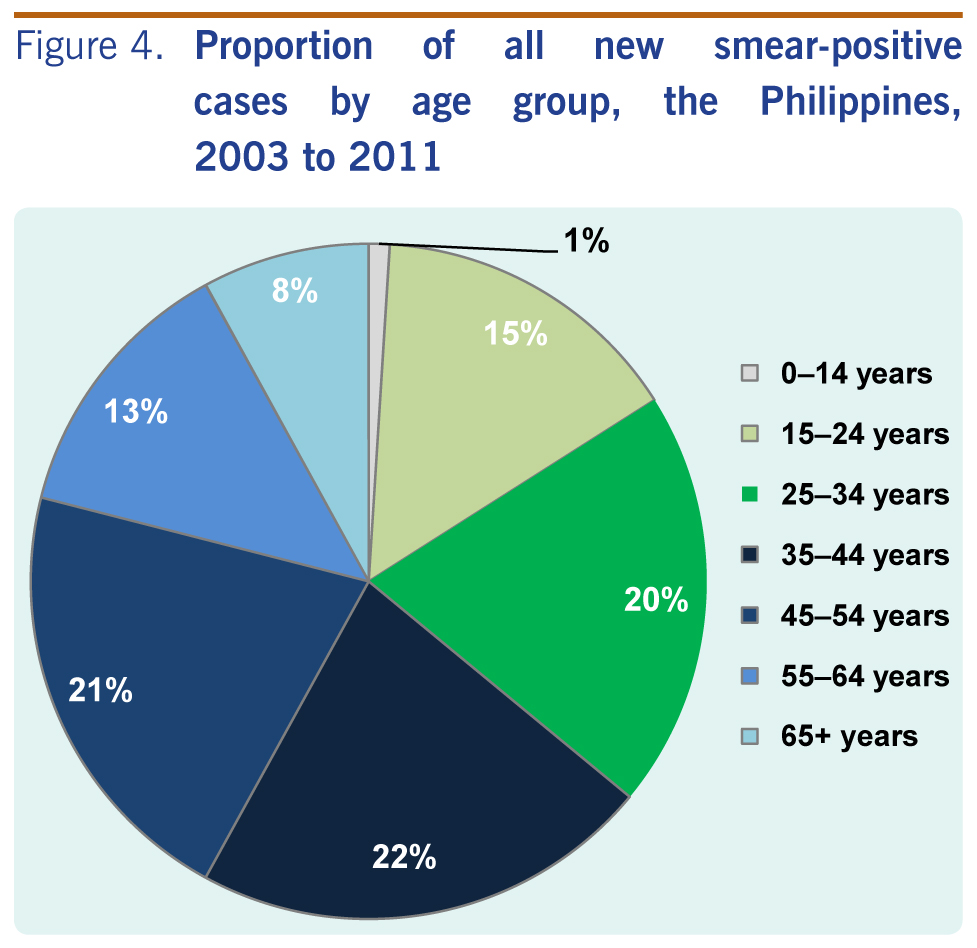
The case notification rate (CNR) for new smear-positive PTB cases increased from 2003 to 2011 (Figure 3). The lowest CNR was in 2003 (86 per 100 000) and the highest was in 2006 (100 per 100 000). During the nine-year period, 63% of new smear-positive cases were aged 25 to 54 years, with 20% in the 25–34 years age group, 22% in the 35–44 years age group and 21% in the 45–54 years age group (Figure 4). The average male-to-female ratio for the period was 2.3.

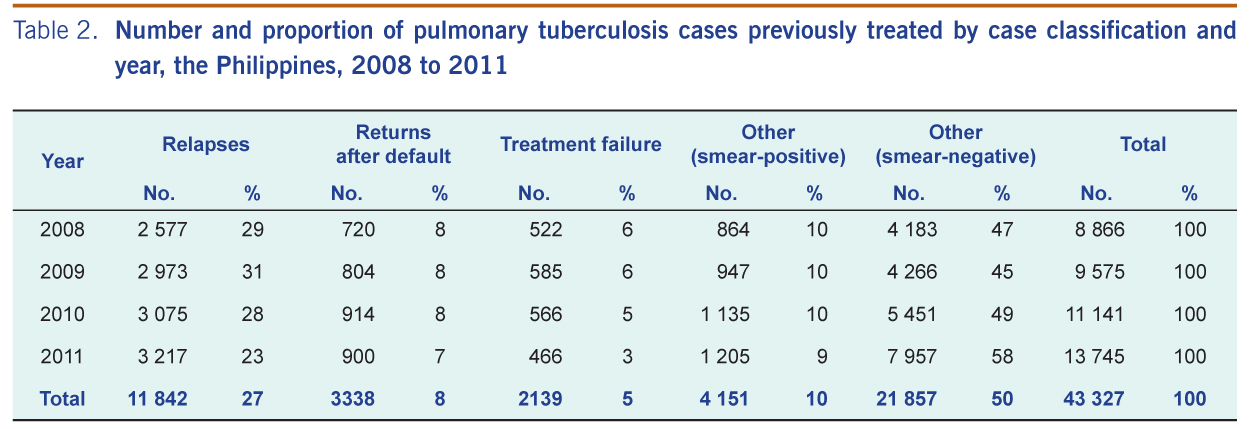
The number of PTB cases previously treated increased from 2008 to 2011 (Table 2). On average, relatively large proportions of PTB cases previously treated were from relapses (27%) or other smear-negative cases (50%).

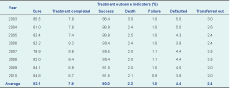
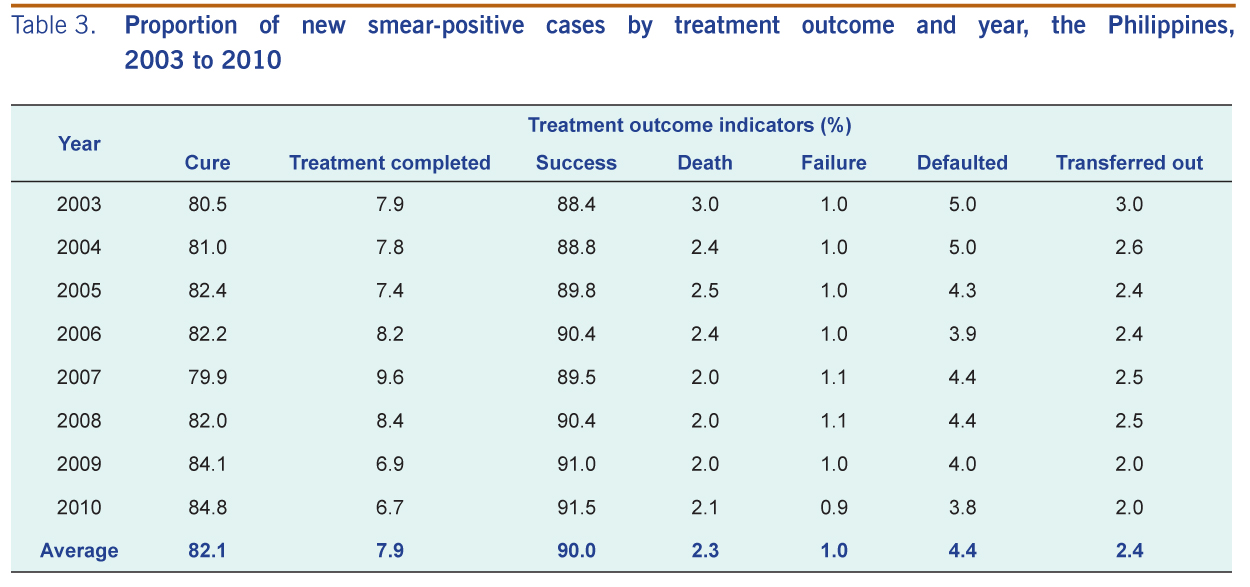
Treatment outcomes for successive yearly cohorts of new smear-positive cases from 2003 to 2010 showed treatment success rates of over 85% with an average of 90% (Table 3). The average annual cure rate for eight years was 82.1%. The eight-year annual average for the other treatment outcomes were: treatment completed at 7.9%, death at 2.3%, treatment failure at 1%, defaulted from treatment at 4.4%, and transferred out at 2.4%.
Changes observed in the TB surveillance data in the Philippines from 2003 to 2011 reflected NTP priorities. The increase in the number of reported TB cases can be attributed to various NTP initiatives to improve access to diagnostic and treatment services especially for the vulnerable sectors. Examples of these initiatives include the expansion of laboratory services and establishing partnerships with public and private health providers. The number of cases contributed by the non-NTP public and private partners also increased from 2008 to 2011; in 2011, these partnerships contributed 11.7% of the total number of cases notified.
More than half the cases per year were new smear-positive cases (apart from 2011 at 46%). This reflects NTP’s high priority for the detection and treatment of highly infectious TB cases to cut the chain of transmission. The increase in the number of new smear-negative cases in 2010 and 2011 reflects a change in programme priorities to detect all forms of TB following the new WHO recommendations issued at that time.9 It also explains the decrease in the proportion of new smear-positive cases in 2011. The increasing trend in the number of cases previously treated from 2008 may be due to the heightened efforts to detect drug-resistant TB cases among these cases. Also in 2008 the management of drug-resistant TB cases was mainstreamed into NTP.
The global target for treatment success rate is 85%,10 this has been exceeded in the Philippines with an eight-year average of 90%. However, the country’s target of 85% for annual cure rates11 was met only in 2010. The low cure rates in previous years were mainly due to the high number of patients who completed treatment without laboratory confirmation of cure (i.e. treatment completed). The average rate of cases defaulting from treatment for the eight-year study period was 4.4%, contributing to the low cure rate and therefore treatment success rates. Moreover, these defaulters may become the future drug-resistant cases.
The death rate of notified TB cases, while low, still contributed to the overall unfavourable treatment outcome as did those cases that transferred out as their outcome is unknown. However, the sustained high treatment success rate reflects ongoing efforts to improve case holding through various NTP strategies such as the administration of DOT in workplaces, homes and other acceptable venues in the community other than the health facility using community volunteers as treatment partners.
In this study, EPTB comprised only 1% of cases, compared to the 15% to 20% reported from other countries.12,13 The low case detection for EPTB in the Philippines may be due to the limited capability of primary care facilities to diagnose these cases or because EPTB cases are diagnosed in hospitals that are not part of NTP. Only 7% of public and 4% of private hospitals report to NTP. However, the higher number of EPTB cases reported from 2008 onwards may reflect the inclusion of more private and non-NTP public providers to NTP. This limitation to the surveillance system is being addressed by increasing the number of NTP-engaged hospitals and improving capacities to confirm EPTB diagnosis.
The proportion of children aged zero to 14 years notified to NTP was 1% for the whole study period, and although there was an increase over this time, its proportion relative to other TB cases did not exceed 2% from 2003 to 2011. It has been estimated that the 0–14 age group should comprise around 15% of cases in low-income countries,14 suggesting that cases in children are either not being diagnosed or if being diagnosed they are not being reported to NTP.
There are some limitations in using NTP surveillance system data to report on TB in the Philippines. Cases diagnosed and treated in health facilities outside the NTP network of providers, including private clinics and hospitals, are not included, therefore the surveillance system is underreporting the total number cases of TB in the Philippines. The submission of case reports are still paper-based, particularly at the peripheral level, which contributes to delays and errors in reporting. Not all regional health units have the capacity to consolidate their data in an electronic format because of gaps in infrastructure and equipment.
The Philippines has achieved improvements in case detection and exceeded the target for treatment success despite numerous challenges, particularly in making services accessible in difficult geographic and socioeconomic settings. The country aims to further improve access to diagnostic and treatment services, especially for highly vulnerable groups, while sustaining high cure and treatment success rates particularly among smear-positive PTB cases. Efforts will be directed at improving diagnostic capabilities in DOTS facilities and hospitals, addressing barriers to follow-up examinations for patients under treatment as well as the factors that promote treatment default and improving the referral system to reduce transfer-outs. Factors that contribute to TB mortality such as diagnostic and treatment delay and co-morbidities need to be addressed as well. Finally, the TB information system will be strengthened to improve its usefulness for surveillance, planning and decision-making. With the current trend of NTP performance, it is predicted that the country will achieve Millennium Development Goals and Stop TB partnership targets before 2015.10
None declared.
None.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}