a The Research Institute of Tuberculosis, Japan Anti-tuberculosis Association, Tokyo, Japan.
b Fukujuji Hospital, Japan Anti-tuberculosis Association, Tokyo, Japan.
Correspondence to Kazuhiro Uchimura (e-mail: uchimura@jata.or.jp).
To cite this article:
Uchimura K et al. Characteristics and treatment outcomes of tuberculosis cases by risk groups, Japan, 2007–2010. Western Pacific Surveillance and Response Journal, 2014, 4(1):11–18. doi:10.5365/wpsar.2012.3.4.016
Introduction: We studied the characteristics and treatment outcomes of the following risk groups for tuberculosis (TB): those with HIV and diabetes mellitus (DM), contact cases, the homeless, foreigners, health care workers (HCW) and the elderly.
Method: A descriptive cross-sectional study was conducted by analysing the Japanese TB surveillance data of all cases registered between 2007 and 2010 (N = 96 689).
Results: The annual proportion of TB cases by risk group was stable over the study period, although there was a slight but significant increase observed for foreigner and elderly cases. Homeless and elderly TB cases had the highest DM co-morbidity (16.6% and 15.3%), respectively. HIV co-infection was low in all TB cases (0.2%) yet highest in foreigners (1.3%). HIV status of 45% of TB cases was unknown. The proportion of multidrug-resistant TB (MDR-TB) was similar among all risk groups (0.0%–0.9%) except foreigner, at 3.4%. Males in most risk groups had higher mortality than females; the mortality of all TB cases in all age groups for both males and females was 3.6–24 times higher than the general population.
Discussion: Reasons for the high proportion of “HIV status unknown” should be investigated and improved. Contact tracing among foreign cases with MDR-TB should be a priority. Homeless persons should be screened for DM together with TB. Programmes to enhance health and nutrition status may benefit TB prevention among the elderly. Tuberculosis screening and TB education are important for HCW.
Globally, it is well documented that certain populations have a higher risk for tuberculosis (TB) due to biological, social or environmental factors.1,2 Identifying populations at risk for TB has important implications for guiding TB control and public health measures. Japan is a high-income country with a mid-level burden of TB. Of the 128 million population, the 2011 TB surveillance reported 22 681 new TB cases with a notification rate of 18 per 100 000 population.3
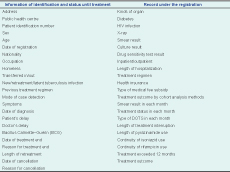
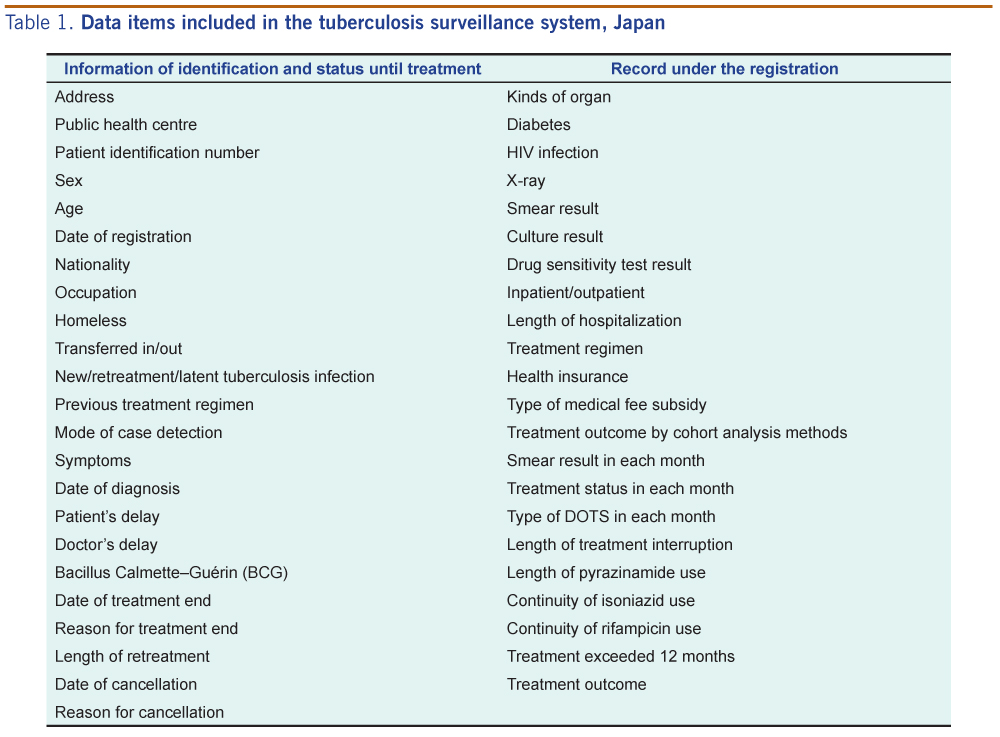
Japan started the first nationwide computerized TB surveillance system in 1987 that underwent revisions in 1992, 1998 and 2007. Reporting of TB is mandatory under Japan’s infectious diseases control law.4 Every public and private hospital is required to report TB cases to a local public health centre where a public health nurse in TB control enters the data into a central computerized surveillance system (Table 1). The data are updated every month. Treatment outcome is automatically coded by the surveillance programme based on the data on treatment regimen and smear results entered. Mechanisms to ensure data quality include automatic verification by the surveillance software on some variables, exchange of information at Directly Observed Treatment meetings at the hospitals, cohort analysis meetings at the health centres and periodic refresher training for public health nurses.
In this paper, we analyse the TB surveillance data and report the characteristics and tuberculosis treatment outcomes of populations identified as high risk for TB by Japanese and international literature including those co-infected with HIV, co-morbidity with diabetes mellitus (DM), cases detected through contact tracing of TB cases (contact cases), the homeless, foreigners, health care workers (HCW) and the elderly.
A descriptive cross-sectional study was performed by analysing data of all new TB cases registered in the Japanese TB surveillance system between 1 January 2007 and 31 December 2010 (N = 96 689). The number of TB cases and the proportion of risk groups over time were evaluated by the test for regression slope and the Cochran-Armitage test for trend. STATA12 (Stata Corp LP, College Station, TX, USA) was used to analyse the frequencies and measures of central tendency and to produce cross-tabulations by risk group. Treatment outcome was included for smear-positive pulmonary tuberculosis (PTB) cases only; the category of “not evaluated for treatment outcome” was excluded from this analysis. Age- and sex-stratified mortality data from national vital statistics were compared with the mortality of the TB cases by risk group. Mortality of TB cases was defined as deaths from any causes during TB treatment course.
Ethical research clearance was not required as the Japanese TB surveillance data do not include case identifiers.
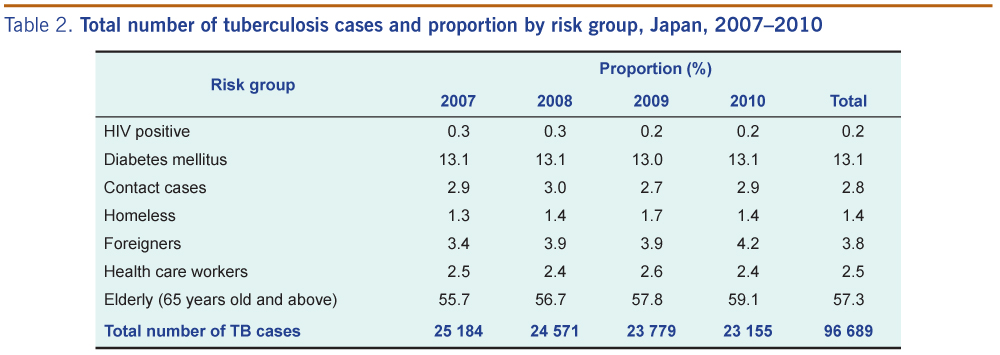
The number of annual TB cases significantly decreased over the study period (P = 0.001) from 25 184 in 2007 to 23 155 in 2010 (Table 2). Among the seven risk groups, the elderly accounted for the largest proportion of TB cases in Japan (57.3%), followed by TB cases with DM (13.1%). The risk group with the smallest proportion was cases with HIV (0.2%) and 2.8% were detected through contact investigation (Table 2). The annual proportion of each risk group was stable over the study period except for foreigners (P < 0.001) and elderly cases (P < 0.001), which show significant increases (Table 2).

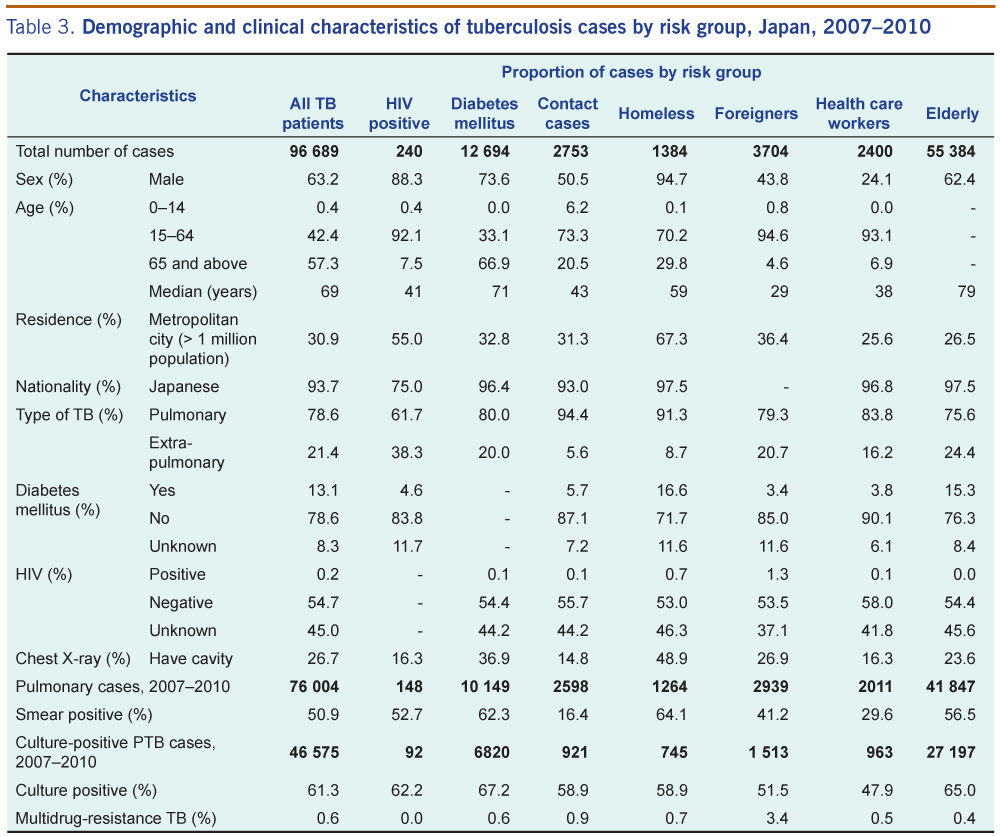
The risk groups with the highest male to female ratio were the homeless and cases with HIV and DM, respectively, while the groups with the lowest male-to-female ratios were HCW and foreigners. The median age of HCW, foreigners, contract cases and cases with HIV ranged from 29 to 41 years, younger than all TB cases (Table 3). More than a half of the cases with HIV and homeless patients were found in metropolitan cities. The proportion of cases having DM testing was relatively high among all risk groups (88%–93%) with the highest proportion of DM co-morbidity among homeless and elderly cases. Almost half (45%) of the cases’ HIV status was unknown (Table 3); this also applied to the reproductive-age TB cases (data not shown).
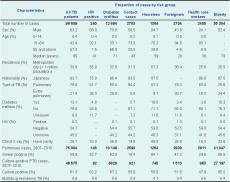
The proportion of cases with HIV among foreigner TB cases was 6.5 times higher than all TB cases. Cavities in the lung on chest X-ray were most frequently observed in homeless cases followed by cases with DM. Within the HCW group, the proportion of smear-positive cases among nurses/public health nurses with PTB (n = 1035) was 26%, compared with 37% for all females aged 20–59 years (n = 9875). Multidrug-resistant TB (MDR-TB) in foreigners was four to nine times higher than the other risk groups and 5.7 times higher than all TB cases.
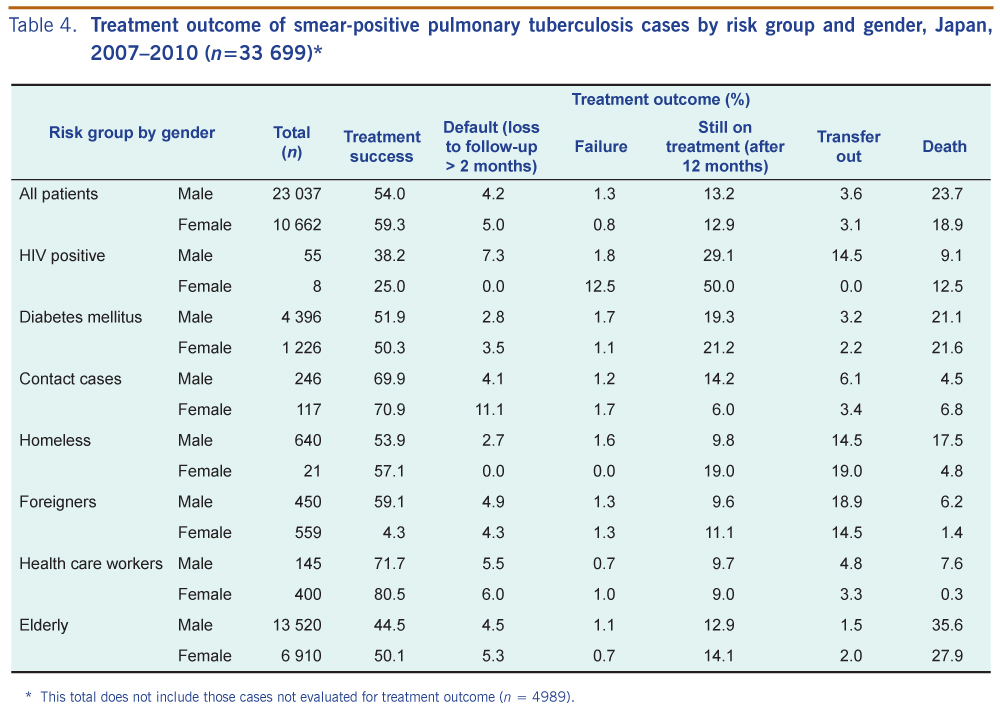
There were 33 699 smear-positive PTB cases with data recorded on treatment outcome. Compared to other risk groups and all TB cases, male and female HCW achieved the highest treatment success, followed by contact cases and foreigners. Contact cases had the highest proportion of default, followed by HCW. Female cases had higher proportions of default than male cases in most risk groups, except cases with HIV, the homeless and foreigners. The proportion of those “still on treatment” was high for all TB cases, especially for both male and female cases with HIV and DM (Table 4).
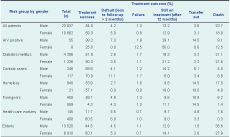
* This total does not include those cases not evaluated for treatment outcome (n = 4989).
For all TB cases and in most risk groups, males had higher mortality compared with females. Mortality for all TB cases in all age groups for both males and females was 3.6 to 24 times higher than that of the general population. Mortality for TB cases aged less than 45 years in most risk groups, except HCW and contact cases, was higher than all TB cases. However, the mortality of older cases for every risk group was similar to those of all TB cases. Remarkably, mortality among male homeless TB cases aged 35–44 was five times higher than all TB cases and 119 times higher than the general population. There were no deaths for female cases with HIV aged 0–74, lower than for all TB cases; however, the number of cases in this group was small (Table 5).
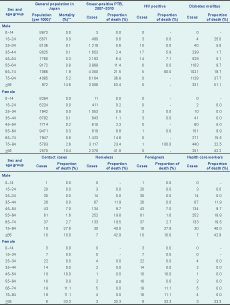
* Average of 2007–2010
** Vital statistics of Japan, 2007–2010
Most international literature reports that the risk groups for TB, such as those with HIV,5 those with DM,6 migrants7 and the homeless,8 have higher mortality or poorer treatment outcome. Although Japan started TB surveillance more than two decades ago, data on risk groups such as cases with HIV and DM and the homeless were only available from 2007. To assess whether these groups also have a higher risk for TB in Japan, routine surveillance data were used for this study. This is the first descriptive report of the general situation of several TB risk groups in Japan.
The magnitude and context of risk groups in Japan were quite different from other high-income countries with low TB burden, which may be related to differences in the prevalence of the risk groups in the general population. Compared with the United Kingdom and the United States of America, Japan has a significantly larger elderly population (23% compared with 16% and 12%, respectively), but lower prevalence of several risk groups. For example the prevalence of DM was 5.1% in Japan, compared with 5.6% in the United Kingdom and 9.4% in the United States of America; the HIV prevalence was < 0.1%, 0.2% and 0.6%, and the proportion of immigrants was < 2%, 9% and 12.8%, respectively. As a result of the different size of the risk groups, the characteristics and treatment outcomes of TB also differed.
A majority (60%) of TB cases in Japan are elderly, whereas in the United Kingdom and the United States of America, the majority (60%–80%) of cases are migrants or foreign-born. In Japan, most elderly cases were infected when they were young yet developed active TB disease when older due to co-morbidity and age-related immuno-suppression, malnutrition and other risk behaviours such as smoking and drinking.9,10 Therefore, there is no direct intervention to prevent active TB among the elderly. Nevertheless, general health interventions such as alcohol and tobacco cessation programmes or programmes to promote balanced nutrition and appropriate physical exercise may indirectly reduce the risk of TB.11 Tuberculosis infection control measures and TB screening for staff and clients in institutions caring for the elderly are recommended. The high proportion of those still on treatment for all TB cases (13.2% in males, 12.9% in females) may be because the majority of TB cases in Japan are elderly and it is quite common to extend the standard treatment regimen according to the individual patient’s clinical condition. Moreover, the Japanese national TB treatment guidelines do not recommend Pyrazinamide for patients aged over 80 years, which lengthens the regimen. A three-month extension of treatment is also recommended for patients with a co-morbidity such as DM.
In line with the World Health Organization (WHO) recommendation,5 DM testing was completed for more than 90% of TB cases in Japan. This may be attributable to the practice of routine blood glucose testing among TB cases in Japan. According to a systematic review,11 cases of TB co-morbidity with DM have a risk ratio for the combined outcome of treatment failure and death of 1.7 (95% CI: 1.4 to 2.1). Our study showed higher mortality for TB cases with a DM co-morbidity for males of younger ages (< 35) but similar mortality for older age groups with a DM co-morbidity, compared with all smear-positive PTB cases of same age group.
The status of HIV testing among TB cases in Japan is quite alarming. Regardless of a country’s HIV prevalence, WHO and the international standard of TB care recommend HIV testing for all TB cases.5 The proportion of TB cases with unknown HIV status was above 40% for all age groups. Reasons for low HIV testing, especially among reproductive-age patients, should be investigated.
Unlike the United States of America or the United Kingdom,8 TB control among the homeless in Japan is not complicated by issues such as drug use and HIV infection. Nevertheless, our study reports high mortality and DM co-morbidity among homeless young adults and this needs to be addressed. Current active case-finding for homeless TB cases should also simultaneously screened for DM.6 Persons with DM have about a three times higher risk of developing TB and therefore may require a different TB screening strategy.
Tuberculosis among foreigners in Japan has continued to be less than 5%. Although TB with HIV co-infection is higher among foreigners than other risk groups, this proportion was only 1.3%. The mortality of foreigner cases was much lower than Japanese cases, probably because they are younger and have four times less co-morbidity with DM than for all TB cases. However, a higher proportion of MDR-TB among foreigner TB cases points to the importance of effective contact investigation among this group. The final treatment outcome for foreigners who transferred out (18.9% in males, 14.5% in females) was unknown, and it is possible that these have ultimately defaulted.
In low- and middle-income countries, the attributable risk for TB disease in HCW compared to the risk in the general population ranged from 25 to 5361 per 100 000 populations per year.13 That the proportion of smear-positive cases among PTB in nurses/public health nurses in this study was lower compared with female cases aged 20–59, and smear-positive cases are an indicator of late diagnosis, suggests that TB cases may be detected earlier in nurses/public health nurses. This may be due to HCW seeking treatment promptly or that routine medical checks of HCW are being conducted. Despite this, overall TB infection and TB disease among HCW is higher than the general population,14 with TB incidence in nurses aged 30–49 being 3.4–4.7 times higher than same-age females in the general population. One of the main reasons for the high TB incidence of HCW is that elderly hospitalized patients infected with TB is causing nosocomial infection to medical staff prior to their diagnosis with TB. Prevention of such nosocomial infection requires earlier TB diagnosis of elderly hospitalized patients.
The final risk group in this study was contact cases. In high-income countries, 2.3% of adults and 4.7% of children in contact with TB cases develop active TB.15 As household size in Japan is becoming smaller, with 32% being one-person households, the number of household contacts is potentially small. However, household and other contacts remain a priority risk group for TB control,16 with almost 3% of cases in this study being contact cases. The current surveillance system does not report the total number of household and other types of contacts. Therefore, the coverage of contact investigation is unknown. Future research should investigate the acceptability of and barriers to contact investigation.
Despite mandatory TB reporting in Japan, anecdotal evidence indicates that underreporting of TB cases may be possible. The magnitude of underreporting is now under a systematic investigation by other researchers. This study is a descriptive analysis using routine surveillance data; therefore analysis using relative risks was not possible due to the lack of reliable denominators of several risk groups such as those with HIV, DM and the homeless. Also access to vital registration data in Japan is limited. The Japanese TB surveillance system is quite advanced in terms of technology and design, yet the system nevertheless may limit our study findings. The high proportion of treatment outcomes “not evaluated” (~12%) may affect the study findings. The current surveillance programme only codes treatment outcomes for those cases receiving the standard treatment regimen. However, this problem has now been recognized, and the additional manual coding of treatment outcomes by public health nurses started in 2012. Although the national surveillance system does not include identifiers, double entering of the same case from different health facilities is unlikely because the data are identifiable at the local level and surveillance staff from the health centres regularly communicate with each other about transferring patients. Recognizing the limitations of the TB surveillance system in Japan will guide its further improvements.
None declared.
This study was supported by the Grant-in-Aid for Scientific Research from the Ministry of Health, Labour, and Welfare, Japan.
{kind=link}
{kind=link}
{kind=link}
{kind=link}