
a Chinese Center for Disease Control and Prevention, Beijing, China.
b World Health Organization Regional Office for the Western Pacific, Manila, Philippines.
Correspondences to: Wei-yi Xiong (e-mail: xiongwy@chinacdc.cn).
To cite this article:
Xiong WY et al. Risk assessment of human infection with a novel bunyavirus in China. Western Pacific Surveillance and Response Journal, 2012, 3(4):69–74. doi:10.5365/wpsar.2012.3.4.002
Objective: To assess the public health risk of human infection from a novel bunyavirus – severe fever with thrombocytopenia syndrome virus (SFTSV) – in China.
Methods: The likelihood of disease spread and the magnitude of public health impact were assessed to clarify overall risk. Literature about hazard, exposure and contextual factors associated with SFTSV infection was collected and reviewed. Information on SFTSV cases and the population in six provinces under surveillance was compared.
Results: SFTSV is a member of the Phlebovirus genus of the Bunyaviridae family. A widely distributed tick species, Haemaphysalis longicornis, can act as the vector; thus the disease is likely to spread in China. Symptoms of SFTSV infection are nonspecific, but have led to multiorgan dysfunction in severe cases. High-risk populations include farmers and older females. Evidence of human-to-human transmission within family and hospital has been reported. The capacity for treatment and diagnosis of SFTSV are adequate in rural communities in China, and community awareness of the disease should be high.
Discussion: There is a low to moderate public health risk related to SFTSV human infection in China. There is potential for an increase in the number of cases reported as awareness increases and when surveillance is expanded.
Severe fever with thrombocytopenia syndrome (SFTS) is a tick-borne haemorrhagic fever first reported in rural areas of central China between late spring and early summer in 2009.1,2 At that time, an unusually high case fatality rate (CFR) of 30% was reported,1 creating wide social concern. In June 2009, a novel Phlebovirus from the Bunyaviridae family, subsequently named SFTS virus (SFTSV), was isolated from a patient’s blood sample.1 A hospital-based active surveillance system aimed at the pathogenic and epidemiologic characteristics of SFTS was put in place in six provinces of central and north-eastern China. It found that among 241 hospitalized patients who met the case definition for SFTS, 171 were positive for SFTSV.1 A tick species, Haemaphysalis longicornis, was found to carry the virus.1,2
Concerns about the potential spread of this novel disease and the possibility of a high number of deaths led to the undertaking of this risk assessment. The risk question addressed was “What is the public health risk related to human exposure to SFTSV in China?”
The risk assessment process involved several components including gathering information through a literature review, a comparative analysis of demographic features between reported SFTSV cases and surveillance population and consensus through group discussion of data based on the likelihood of disease spread and the impact on public health. Estimates of likelihood and impact were then combined to decide on the overall level of risk with the assistance of a risk matrix to enhance the rigour of discussion. The estimates of likelihood of spread of disease, impact on public health, level of overall risk and risk matrix followed the World Health Organization guide for undertaking risk assessment for acute public health events.3
Expertise for group discussion included a core group of four people specializing in public health surveillance, epidemiology and infectious disease. Group discussions were held several times to reach consensus on the level of overall risk and the evidence that supported this level of risk. Presentation of outcomes following core team deliberation to a broader group with expertise in public health, laboratory, epidemiology, infectious disease, logistics and risk communication provided further refinement of the outcomes. Personal communication between the core team and experts from the Chinese Center for Disease Control and Prevention finalized the evidence.
Literature about hazard, exposure and contextual factors associated with SFTSV infection were searched using Google Scholar. Keywords used (both in English and in Chinese) included “severe fever with thrombocytopenia syndrome,” “tick-borne disease,” “SFTS,” “SFTSV,” “phlebovirus,” “bunyavirus,” “tick,” “Haemaphysalis longicornis,” “health care-seeking” and “social panic.” Full texts of the key articles that needed to be reviewed were collected from multiple sources such as PubMed, ProQuest, Wanfang and journals’ web sites.
Based on the results of the literature review, only the capacity for diagnosis and treatment and public awareness were assessed for resilience under the section of contextual factors. The preparedness of local communities and their capacity to mitigate and/or adapt to disruptive consequences were not assessed because of the lack of available data and the difficulty of measuring the flexibility of community preparedness.
Demographic data of the population in the six provinces of central and north-eastern China where surveillance for SFTSV has been conducted were gathered from the China statistical yearbook 2010. The chi-squared test was used to compare the age and gender differences between SFTS cases and this population.
SFTSV is a member of the Phlebovirus genus of the Bunyaviridae family.1,2 Prior to the discovery of SFTSV, the Phlebovirus genus consisted of 68 known serotypes divided into two major antigenic groups: the sandfly fever group (55 serotypes, including Rift Valley fever) transmitted by sandflies, and the Uukuniemi group (13 serotypes) transmitted by ticks.4 Phylogenetic analyses shows that SFTSV variants isolated from humans and ticks are closely related to each other yet form a separate lineage distinct from Uukuniemi virus and other phleboviruses.1 The Bunyaviridae family comprises single-stranded RNA viruses that cause a variety of human diseases including Rift Valley fever, SFTS, Crimean-Congo haemorrhagic fever and Hantavirus pulmonary syndrome. As single-stranded RNA, these viruses are highly prone to mutations that can enhance their capacity to adapt to new vectors and hosts.5
Complete information about the spectrum of infection in humans is not available. According to the prevention and treatment guideline published by the China Ministry of Health, the incubation period of SFTSV infection is one to two weeks.6 Symptoms are nonspecific, including high fever (38°C or higher), anorexia, fatigue, gastrointestinal symptoms (abdominal pain or tenderness, nausea, vomiting and diarrhoea) and regional lymphadenopathy.1,2,6 Laboratory test findings showed that 95% of patients had thrombocytopenia, 86% had leukocytopenia, 84% had proteinuria and 59% had hematuria.1 Blood levels of serum alanine aminotransferase, aspartate aminotransferase, creatine kinase and lactate dehydrogenase were elevated in most patients, suggesting multiorgan dysfunction.1 According to limited published data, the case fatality rate varied from 12% to 30%.1,2 Other bunyavirus, such as Crimean-Congo haemorrhagic fever virus and hantavirus produce severe haemorrhagic fever and potentially fatal outcomes with mortality for hantavirus reaching 35%.7
Surveillance for SFTS among hospitalized patients was undertaken in six provinces in central and northeastern China: Liaoning, Shandong, Henan, Hubei, Anhui and Jiangsu.1 Using the case definition defined by the China Ministry of Health,6 the total number of cases between June 2009 and September 2010 was 241, and 96% (148/154) of the laboratory-confirmed cases in 2010 occurred from May to July.1
The age of SFTS cases ranged from 39 to 83 years. People aged over 50 years made up 75%1 of the cases but constituted only 26% of the population under surviellance (P < 0.001). Fifty-six per cent of the cases were female1 compared with 49% of the total population (P = 0.029). While 97% of the cases were farmers living in wooded and hilly areas and working in the fields,1 precise information about occupation of the total population in the surveillance provinces was not available.
No SFTSV was identified through real-time polymerase chain reaction (PCR) and no antibodies against SFTSV were identified from the patient-matched healthy control subjects in the endemic areas and healthy subjects from non-endemic areas.1 Little population-based seroprevalance information was available; however, one study in Shandong Province in 2011 reported that 2% of 237 healthy humans and 83% of 134 goats tested had antibodies to SFTSV.8
Haemaphysalis longicornis is widely spread in China. The tick species has been found in 18 provinces (Hebei, Shandong, Henan, Anhui, Jiangsu, Taiwan, Hunan, Hubei, Shanxi, Shaanxi, Guizhou, Yunnan, Sichuan, Xizang, Gansu, Heilongjiang, Jilin and Liaoning), including all six surveillance provinces.9
In areas where SFTSV has been found, Haemaphysalis longicornis taken from domestic animals were found to carry SFTSV, suggesting it may be the vector for the virus.1,2 Regular hosts of Haemaphysalis longicornis include goats, cattle, pigs, cats, rats, mice, birds and humans.1 None of the animals from which ticks were collected showed signs of illness, and there were no reports of a similar disease occurring in animals in the same region.2 Antibodies to SFTSV have been found in goats, cattle, dogs, pigs and chickens in Jiangsu Province.10 There was no evidence of SFTSV being isolated from mosquitoes captured in the human-affected areas.1
A recent publication by Bao, et al11 reported a family cluster of SFTSV where person-to-person transmission may have been plausible. Similarly Gai, et al.12 reported a cluster of five cases suspected to have acquired the virus from blood or close nosocomial contact with a case that died from SFTSV. Personal protective equipment was not used by any of the people dealing with the index case in this nosocomial setting.
Experts suggest that the capacity for treatment and diagnosis of SFTS is adequate in rural communities in China because of the continuous efforts by the China Ministry of Health in recent years to enhance the national public health system. Most of the provincial-level laboratories have the ability to confirm SFTSV infection, which includes isolation of SFTSV from the patient’s serum, detection of SFTSV RNA in patient’s serum during the acute phase of the illness, detection of seroconversion or an elevation by a factor of four in serum IgG antibodies against SFTSV on enzyme-linked inmmunofluorescence assay or neutralization testing in serum obtained during the convalescent.6 It is unknown, however, whether tests for SFTSV are undertaken on a regular basis. There is no specific treatment other than supportive therapy;6 thus most of the county-level hospitals have the ability to carry out the recommended therapy for SFTS patients.
Information about cost of diagnosis and treatment of SFTS was not available, although the majority of tests and drugs required for SFTS are on the reimbursement list of the New Rural Cooperative Medical Care System. This system covers more than 90% of the rural areas in China, including the areas in which SFTS cases have been found.13
Community awareness of the disease should be high. In September 2010, the China Ministry of Health held a special press conference about SFTS. Soon after, guidelines on SFTS control and prevention were issued by the Ministry of Health and distributed to the public. Health education information was published on the Internet, printed in newspapers and broadcast on radio and TV. Local Centers for Disease Control and Prevention distributed posters and leaflets to local residents. Therefore, people living in the affected area received information about SFTSV through multiple channels.
No formal studies have been published that provide a quantitative or qualitative estimation of interest in health matters, health care-seeking behaviour or the psychosocial impact caused by SFTS. However some understanding can be made through analysis from studies on other diseases.
In 2007, in a study linking hand, foot and mouth disease cases, media reports and a survey of hospital visitors showed that health care-seeking behaviour increased dramatically after initial cases were reported. The number of hospital visits for hand, foot and mouth disease was five times higher than that of the preceding year, and 85% of visitors reported that they felt “panic.”14
Residents living in rural areas usually have negative health care-seeking behaviour. In a study conducted in Jiangsu Province, 64.8% of rural area residents reported they would not go to hospital until they become seriously ill, and self-treatment or visiting a private clinic was the first choice for 51.9% of the rural area patients.15 If these delays in seeking qualified professional help also occur for SFTS cases, then there are likely to be more severe cases at presentation.
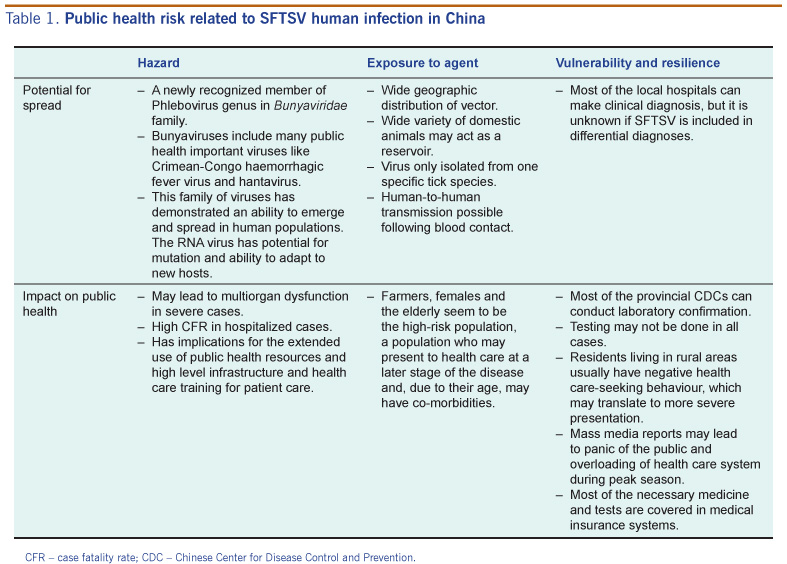
The risk of SFTSV was characterized using the information collected, with key factors considered to assess the likelihood of spread of disease and its impact on public health (Table 1).
CFR – case fatality rate; CDC – Chinese Center for Disease Control and Prevention.
Discussion concluded that it is likely that the disease would spread due to the wide geographic distribution of the vector, ready contact with humans in rural settings and the capacity of this family of viruses to emerge and spread in human populations. Limited cases of nosocomial infection may also occur. Based on this, the overall public health impact was assessed as minor. Good diagnostics and treatment are available; however, the most-at-risk population, elderly females in rural farming communities, may present to health care late. This may increase the disease severity at presentation and thus the need for prolonged and sophisticated treatment in health care facilities. Overall the combination of the level of likelihood of spread of disease and the impact on public health results in a low to moderate public health risk of SFTSV human infection in China.
A low level of risk for a disease would indicate that it can be managed under existing protocols for surveillance systems, response and regulation.3 As the level of risk increases, the focus and intensity of the guidance for SFTS prevention and treatment must also change so that the risk posed by the disease can be reduced to an acceptable level. This will allow the local health facilities to better handle the consequences of the changed level of risk. With a low to moderate level of risk for SFTS, there is an indication that current protocols are working well; however, some enhancement to current practice may be appropriate for public health management of the disease. Recommendations made by this paper are summarized below.
This assessment had some limitations. Only published documents were used in this assessment as we were unable to access the primary data. SFTSV is novel and as such there have been few studies conducted. Therefore there were some key gaps in information including transmission mode, seroprevalence, full spectrum of infection, health care-seeking behaviour and suspicion of disease by clinicians. Hospital-based surveillance may bias the number of cases and spectrum of disease identified to date, community-based surveillance may have found more mild and asymptomatic cases and could provide a thorough knowledge of the status of this disease. Comprehensive national surveillance data and further research will be useful in understanding the risk to public health from this disease. There is potential for an increase in the number of cases reported as awareness increases and also from increased case reporting from other provinces when active surveillance is expanded. This will lead to a greater need for diagnosis and health care service during the peak season.
Based on this risk assessment, the main recommendations for decision-makers at the national level on SFTSV infection prevention and control in China are:
None declared.
None.
The authors thank all the experts from Chinese Center for Disease Control and World Health Organization Regional Office for the Western Pacific who gave their generous and valuable opinions and supports.
{kind=link}