a World Health Organization Country Office, Ha Noi, Viet Nam.
b Provincial AIDS Center, Hai Duong, Viet Nam.
c Independent Consultant, Bangkok, Thailand.
d Population Services International, Ha Noi, Viet Nam.
Correspondence to Nguyen Thien Nga (e-mail: nguyenthie@wpro.who.int or nguyenthienga@yahoo.com).
To cite this article:
Nga NT et al. Innovative data tools: a suite for managing peer outreach to key affected populations in Viet Nam. Western Pacific Surveillance and Response Journal, 2012, 3(3):29-34. doi: 10.5365/wpsar.2012.3.2.003
Problem: The paper tools used to monitor outreach work in all major cities in Viet Nam had substantial writing requirements for each contact with difficulty maintaining confidentiality.
Action: This paper describes the development of a Unique Identifier Code (UIC), a field data collection notebook (databook)and a computer data entry system in Viet Nam. The databook can document 40 individual clients and has space forcommodity distribution, group contacts and needles/syringe collection for each month.
Outcome: Field implementation trials of the UIC and databook have been undertaken by more than 160 peer outreachworkers to document their work with people who inject drugs (PWID) and sex workers (SW). Following an expanded trialin Hai Phong province, there have been requests for national circulation of the databook to be used by peer educators documenting outreach to PWID, SW and men who have sex with men. The standardized UIC and databook, in a variety of locally adapted formats, have now been introduced in more than 40 of the 63 provinces in Viet Nam.
Discussion: This development in Viet Nam is, to our knowledge, the first example of the combination of a confidential UIC and an innovative, simple pocket-sized paper instrument with associated customized data-entry software for documenting outreach.
The HIV epidemic in Viet Nam remains in a concentrated stage with signs that it may have begun to stabilize over the last two years. There has been some decrease in HIV prevalence among people who inject drugs (PWID) and female sex workers (SW) in most provinces. According to the Viet Nam national 2011 sentinel surveillance, HIV prevalence among PWID and SW remains high, at 13.4% and 3%, respectively; Integrated Biological and Behavioural Surveillance 2009 data indicate that prevalence among men who have sex with men (MSM) also remains high at 16.7%.1 The distribution of HIV cases largely follows the distribution of these three populations that are heavily concentrated in urban centres (though not absent in non-urban communities). The overall adult HIV prevalence (ages 15-49) remained at 0.45% in 2011.2
Since 2004, projects implementing broadly similar HIV prevention peer outreach targeting PWID and SW have expanded across Viet Nam to 60 provinces for the Needle Syringe Programme (NSP) and 63 provinces for condom distribution.3 These outreach activities, designed to take HIV prevention education, behaviour change communication and HIV prevention commodities into the networks of key affected populations, have followed similar practices under each project, often being co-located in the same province, district or even commune, and reaching out to the same networks. At the end of 2011, these peer outreach workers numbered in excess of 6200 across the 63 provinces.3
Previous paper instruments to collect client contact data by peer outreach workers, under the variety of projects in Viet Nam, had problems with reliability of data recording, confidential monitoring of individuals and recording of commodity distribution and other services. There exist major practical challenges to harmonizing and collecting data for various coverage indicators at the provincial and national level while managing the data collection burden in the field.4
To improve the collection and reporting of these outreach data, we document the development of a suite of innovative data tools for managing peer outreach to PWID, SW and MSM in Viet Nam.
The tools in use for peer outreach at the beginning of this project in 2008 were extremely varied, comprising paper notebooks of A5, A4 or even larger sizes. The data collected were loosely standardized but often included name, address, birthdate, mobile number and signatures for each contact where free commodities (needles/syringes, condoms) were distributed. Some projects attempted to use code numbers or names including codes for frequency of contact. Most outreach workers had their own informal notebooks from which they transferred data into official project books at home at the end of each day. These paper systems often involved serious breaches of client confidentiality and gave supervisory staff false confidence in the system's protection against service contact fraud and diversion of commodities.
The data collected by outreach workers were transferred to summary sheets at the district level, and both the number of contacts and of individuals were collated for provincial reports. There was no system to avoid double counting of individuals by different outreach workers or services, or for the accurate collating of total monthly individuals reached. The summary outreach data were usually collated on paper at each Provincial AIDS Center (PAC) from the district reports, for hardcopy transmission to Central Project Management Units in Ha Noi, as well as for entry into the Ministry of Health online HIV reporting system.
In 2008, Population Services International (PSI) in Viet Nam initiated development of a Unique Identifier Code (UIC) for their programmes with PWID and SW in Viet Nam.5,6 PSI undertook a test of several proposed UICs on large databases of names in university lists (>4000 student names in two cities) to identify the sequence of likely initials and numbers able to be generated from an individual's family name, location and age that could generate a de-identifying code with low duplication rates (less than 2.5% for example). The aim of the search for such a unique identifier was to find a code that could be generated consistently by clients which would preserve their confidentiality and protect their privacy, yet which contained some data useful for client contact analysis (such as age and gender) and which could readily be standardized across several client services. The use of UIC would enable removal of double-counted clients and creation of more accurate coverage numerators.
Of the codes tested by PSI, a nine-digit easily self-generated code using letters and numbers was identified with a duplication rate of less than 1.5% in all cities and 0.9% overall. In collaboration with several development partners and the Viet Nam Authority of HIV/AIDS Control this code was refined to 10 digits incorporating the standard Ministry of Health three-letter code for each of the 63 provinces. The UIC could be collected over time as familiarity and trust developed; initially a nickname was used by the outreach worker.
The final field-tested code agreed as the national standard contains:
In a parallel process, a standardized data collection tool for the outreach workers (the databook) was developed. This process began with the collection and analysis of many outreach data collection tools from across the country and region. It was agreed that the new tool should be pocket-sized; be able to track at least 40 individual clients; require a minimum of written pen strokes to record each contact; and facilitate monitoring of outreach worker client workloads, service coverage and service intensity.
The initial versions of the databook were based on small handbooks used in a small number of provinces in Viet Nam by Burnet Institute, other project tools and data sheets from several NSPs in Australia in the early 2000s. Several refinements were field-tested in Hai Duong province by PAC, but all required an excessive number of pen strokes to accurately record client field contacts.
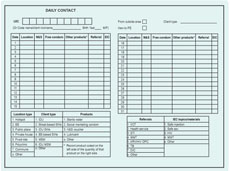
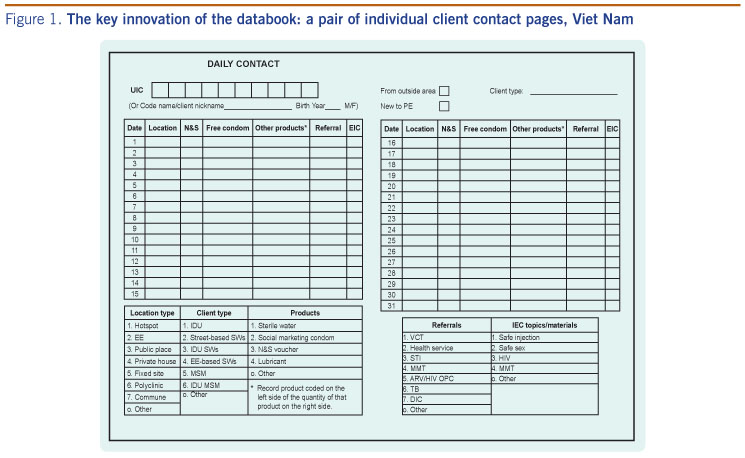
An innovative adjustment was made to the prototypes in 2009 with the restructuring of the databook into client pages, each divided into lines for 31 days, and a client index at the front, to quickly direct the worker to the relevant pages for known or new individuals (Figure 1). The tool also allowed for documentation of outreach activities including distribution of needles/syringes, sterile water, condoms, lubricant and other HIV prevention commodities.
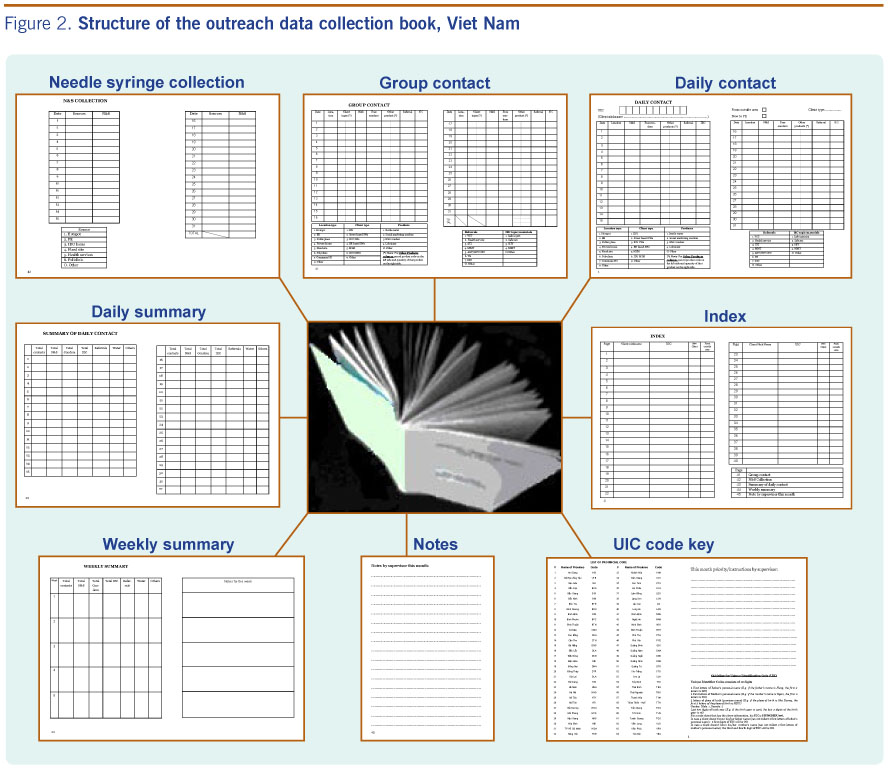
The databook thus evolved into an inexpensive A6-size pocket recording book of around 45 pages per month (Figure 2) with:

The 40 pairs of pages devoted to documenting up to 40 clients each month provide single-digit number keys for recording common commodities and referral services. This number of client pages is adjustable according to the average and maximum number of individual clients each outreach worker is likely to see each month.
Following extensive field testing, the innovative databook was introduced through a series of participatory training courses for health system supervisors and peer outreach workers in five provinces.
The final component of the outreach worker suite of tools was a tailored freeware database built on the Microsoft Access platform by one of the authors (NB). It is fully consistent with the data collected in the new databook and with the health system environment and reporting structure in Viet Nam, and was based on similar client service databases developed for use in China and Myanmar.7
The new software allows bilingual entry, interpretation and export of data. It is easy-to-use and requires minimal keystrokes. The use of UIC and the data-entry software enables provinces and projects to enter data at a district or provincial level, to monitor frequency of contacts with clients and to provide reports documenting clients contacted each month, quarter or year. The software is now at an advanced stage of field testing in three provinces in Viet Nam.
In the absence of a full computerized database at any site, accurate identification of double-counted clients can be undertaken at the district or provincial level by creating simple alphabetical lists of all the collected UIC by month and cumulative by year.
Feedback from the development of UIC found it to be easily generated and remembered by the clients, with retained confidentiality. It has been consistently provided over time in several provinces with no perception of release of personal information.8 Within the first month of the pilot, full UIC were collected for 55% of SW and 100% of PWID, with the remainder collected using the nickname. Because most peer outreach workers know their clients well, the majority of UIC were easily collected - particularly for PWID and MSM outreach. In the absence of a full UIC, the nickname is vital.
peer outreach workers in the pilot phase of the databook reported that it was easy to document client contacts with a minimum of pen strokes, and they could use nicknames or a full UIC. At the end of every day and every week, the outreach workers could easily total the commodities they distributed and activities conducted in the summary pages. For ease of supervision, the book provides at a glance an accurate measure of individuals contacted each month plus a good impression of intensity and nature of client contacts.
Although the databook may seem wasteful of paper or space, the benefits of ease of use, clarity, speed and accuracy, and the avoidance of the transcription of data burden generously outweigh this downside. The databook requires 12 books per year per outreach worker and therefore the programme cost is dependent on the quality of paper (12 A4 pages per book) and the size of print runs.
Post-implementation supervision of the outreach team leaders and workers has been used to ensure consistent recording detail and appropriate and accurate recording of UIC and service content. The databook has been readily used by low literacy peer outreach workers. It is fortunate that the ability to write letters and numbers is near universal in Viet Nam, which allows for easy recording of codes by peer outreach workers. There may be difficulties in less literate sub-populations.
Comprehensive training modules have been developed for use of UIC and the databook. All trainings, usually lasting one day, have been conducted in Vietnamese with systematic use of group discussion, examples and paper exercises. The databook, in a variety of (minimally) locally adapted formats, and the standardized UIC has now been adopted by two large donor-funded harm reduction projects, and are now progressively being used by outreach workers in more than 40 of the 63 provinces in Viet Nam.
During the expanded trial in Hai Phong there was considerable interest expressed by programme managers from other provinces for national propagation of these tools for their ease of documenting peer outreach to PWID, SW and MSM, and the distribution of commodities. The software to manage the wealth of data collected by the outreach workers is also slowly being rolled out, yet programme managers can, using the databook, UIC and a simple spreadsheet, generate accurate client service data and low technology client lists to remove double counting.
This suite of tools for effective management and documentation of peer outreach client contacts in Viet Nam is, to our knowledge, the first example of the combination of confidential UIC and an innovative, inexpensive pocket-sized paper instrument with associated customized data-entry software for documenting outreach.
Initial reservations about obtaining UIC information from key affected populations, limited literacy of the peer outreach workers and coding difficulties have been overcome by the extremely hands-on nature of the training process and the follow-up supervision that emphasizes techniques for stepwise collection of UIC over time. Collection of the complete UIC was consistently more difficult from more mobile venue-based SW than other client groups.
In a new country context, rigorous testing of a proposed UIC using a large, detailed database of names will be necessary to ensure that the duplication rate of the code remains low (recommended less than 5%) with the training tailored to the local situation and literacy.
None declared.
Funding for this research and field trial activities has been provided from a number of organizations including the Swedish International Development Agency, United States President's Fund for AIDS Relief, the United Kingdom Department for International Development, the Norwegian Agency for Development Cooperation, the World Bank, the Australian Agency for International Development and the Government of Viet Nam National Target Programme for HIV.
{kind=link}
{kind=link}