a Partnership for Epidemic Analysis (PEMA), New Delhi, India.
b UNAIDS Regional Support Team Asia and the Pacific, Bangkok, Thailand.
c HIV and AIDS Data Hub for Asia-Pacific, Bangkok, Thailand.
Correspondence to Tobi Saidel (e-mail: tobisaidel@pemapartners.org).
To cite this article:
Loo V et al. HIV surveillance systems in the Asia Pacific region. Western Pacific Surveillance and Response Journal, 2012, 3(3):9-14. doi:10.5365/wpsar.2012.3.2.009
In 2011, the United Nations Joint Programme on HIV/AIDS (UNAIDS) Regional Support Team for Asia-Pacific conducted a stock-taking process of available strategic information in the Asia Pacific region. This paper summarizes the progress of HIV surveillance for 20 countries in the region, covering population size estimates of key populations at higher risk, HIV case reporting, HIV sentinel surveillance and probability surveys of behavioural and biological markers. Information on surveillance activities was obtained from publically available surveillance reports and protocols, supplemented by personal communication with the UNAIDS monitoring and evaluation advisers and surveillance experts in country. Key findings include substantial efforts in broadening the number and types of HIV surveillance components included in national HIV surveillance systems and adopting approaches to make surveillance more cost-efficient, such as integrating routine programme monitoring data and passive surveillance case reporting systems. More investment in regularly analysing and applying surveillance data to programme strengthening at the subnational level is needed but will require additional capacity-building and resources. The ability to triangulate multiple sources of surveillance data into a more comprehensive view of the HIV epidemic will be enhanced if more investment is made in better documentation and dissemination of surveillance activities and findings.
During the decade following the introduction of second generation surveillance for HIV and AIDS in 2000,1 there was a proliferation of surveillance data collection activities throughout the Asia Pacific region. HIV and AIDS surveillance systems evolved differently in different countries depending on a host of factors including type and stage of the epidemic, level of government and donor commitment and support and local capacity. Over the last decade, two global HIV surveillance conferences and several reviews of HIV surveillance systems have documented some of this progress.2-4 In 2011, the Joint United Nations Programme on HIV/AIDS (UNAIDS) Regional Support Team for Asia-Pacific reviewed available strategic information in the Asia Pacific region as part of a stock-taking process.5 The intention was to describe how surveillance and monitoring and evaluation systems had evolved in the countries in the region and to identify strengths and opportunities for better use of data to understand and respond to the epidemic. This paper focuses on the surveillance components of the project.
The project included 20 countries within the UNAIDS Asia Pacific region, including Afghanistan, Bangladesh, Bhutan, Cambodia, China, Fiji, India, Indonesia, the Lao People's Democratic Republic, Malaysia, Maldives, Mongolia, Myanmar, Nepal, Pakistan, Papua New Guinea, the Philippines, Sri Lanka, Thailand, and Viet Nam. Four types of surveillance activities were included: estimation of the size of key populations at higher risk; HIV case reporting; HIV sentinel surveillance (HSS) and probability surveys of risk behaviours, including those integrated with biological markers. It also covered the use of surveillance data for epidemic modelling, programme design and monitoring and evaluation.
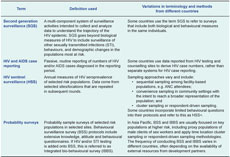
Information on surveillance activities collected for this review came from publically available surveillance reports and protocols supplemented by unstructured interviews with the UNAIDS monitoring and evaluation (M&E) advisers and surveillance experts in country. Collated tables and documentation developed by the Asia Pacific-Regional Support Team and the HIV and AIDS Data Hub for Asia-Pacific were also used. The variation in use of terms to describe different surveillance activities across countries was a key challenge. For purposes of clarity, we used the terms HIV case reporting, HSS and probability surveys (includes behavioural surveillance survey [BSS] and integrated bio-behavioural survey [IBBS]) (Table 1).
Resources for generating population size estimates have increased as the core uses of such data for programme planning, budgeting and monitoring of programme coverage have been recognized. More recently, size estimation exercises have also been recognized as a key component of the surveillance system and an integral part of understanding epidemic potential in "Know Your Epidemic" analysis.6
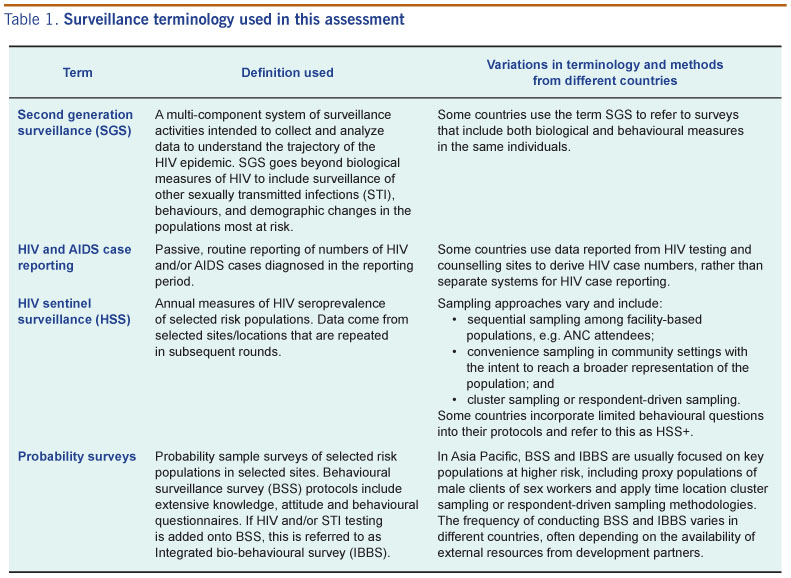
A large array of approaches are being used to generate size estimates in the region, most commonly mapping of key populations in certain locations and survey-based multipliers in conjunction with probability surveys of key populations at higher risk (Table 2). Since 2000, 14 countries have generated population size estimates using mapping techniques, while 10 have used the multiplier method. As solicitation points and partner-meeting venues are easier to define for sex workers and men who have sex with men (MSM), these populations are more often estimated using the mapping method. Almost twice as many countries have relied on multiplier-based approaches for estimating the population size of people who inject drugs (PWID) than those that use mapping. Six countries have used both mapping and the multiplier method in the same population to enable comparison of results between methods. National-level estimates of the size of key populations at higher risk are usually made by extrapolating local-level estimates from a few areas (Table 2).

FSW - female sex workers; MSM - men who have sex with men; and PWID - people who inject drugs.
* In Viet Nam, specific implementing partners have used mapping, enumeration, capture-recapture and multipliers in selected provinces, but not through a national/centrally coordinated effort.
Despite these efforts, a large number of countries still lack local size estimates of key populations at higher risk in most geographic areas or feel dissatisfied with the level of reliability of the results from their size estimation efforts. Countries are interested in strategies for optimizing their size estimation activities, including:
Of the 20 countries included in the review, 18 maintain functioning HIV case reporting systems. Many of these systems rely on routine monitoring data for HIV counselling and testing services as the primary source from which to obtain HIV cases disaggregated most commonly by age, gender and risk factor. This combining of routine data with passive surveillance systems is efficient but may result in the exclusion of collecting more detailed information about newly diagnosed HIV cases, e.g. occupation, whether the person has a regular sex partner. Place of residence is another important characteristic to collect on HIV cases to identify emerging geographic pockets of the epidemic; however, some routine monitoring systems for HIV counselling and testing use the location of the testing site as an imperfect proxy for this information. On the other hand, a benefit of most routine monitoring systems for HIV testing and counselling is data on the number and types of people tested. The availability of these "denominators" are critical for determining whether trends in HIV case reports reflect changes in testing patterns rather than potential changes in the number of actual cases.
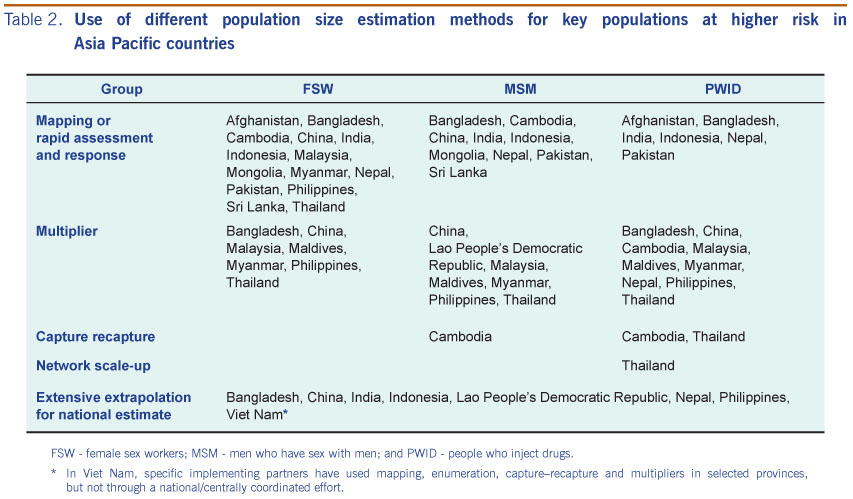
Globally, HSS originated as a relatively low-resource method for observing trends in annual HIV seroprevalence among clinic-based populations who provided blood specimens for other routine tests, i.e. syphilis screening among antenatal care (ANC) attendees. Data from ANC attendees are valuable in generalized epidemic settings, but are less useful in tracking the HIV epidemic in low-level and concentrated epidemic settings. Eleven countries in the Asia Pacific region have adapted HSS methods of sampling to measure HIV seroprevalence among key populations - Bangladesh, Cambodia, China, India, Indonesia, Mongolia, Myanmar, the Philippines, Sri Lanka, Thailand and Viet Nam. Nine of these countries also include seroprevalence measures among ANC populations (Bangladesh and the Philippines do not conduct HSS among ANC populations). A major challenge in conducting HSS among key populations is developing consistent approaches for sampling hidden, mobile groups who may not routinely come to health facilities for services. Over time, many countries have adopted community-based methods for sampling these groups; however, there are insufficient resources to apply rigorous approaches for representative, replicable samples in most countries. In some countries, the distinction in seroprevalence measures from HSS and probability survey efforts (i.e. IBBS) have become less clear (Table 3).

ANC - antenatal care; BSS - behavioural surveillance survey; HSS - HIV sentinel surveillance; IBBS - integrated bio-behavioural survey; STI - sexually transmitted infections; and TB - tuberculosis.
As new components of surveillance have been introduced and the numbers of HSS sites have increased, the available management and technical resources have been stretched. In some cases quality control and continuity of data have suffered. These inconsistencies can be difficult to reconcile when interpreting HSS trend data. Further exacerbating this problem, there has often been an absence of written reports documenting methods and results and potential quality control problems during the implementation of surveillance activities.
Many countries in the region have put considerable resources into conducting probability surveys of female sex workers (FSW), MSM and PWID to obtain representative measures of HIV, sexually transmitted infections (STI) and risk behaviour. Eight countries, including Bangladesh, China, Cambodia, India, Nepal, Pakistan, Thailand, and Viet Nam, now have more than three rounds of consecutive BSS or IBBS survey data for key populations at higher risk in selected sites.
From the review of available documentation, it appears that the main use of surveillance data in the region is related to quantifying the burden of disease at the national level every two years using the Estimation and Projections 7 and reporting on biennial United Nations General Assembly Special Session indicators at the national level.8 More recently, countries have begun to apply these models at the subnational level to better understand local epidemic patterns that may better guide programming and help develop a more informed national picture of the epidemic (e.g. Viet Nam, Nepal, India and Indonesia).
Several countries have also used surveillance data for the purpose of impact evaluation of their national programmes generally, as well as of specific prevention programmes (e.g. 100% Condom Use Programme).
Over the past decade, HIV surveillance systems in the region have evolved from focusing primarily on HIV case reporting and annual seroprevalence measures from HSS to inclusion of a broad array of data collection activities. The types of data include population size estimates, behavioural surveys and integrated bio-behavioural surveys that are combined to inform the understanding of the epidemic and the response.
More recently, it appears that some countries are scaling down or streamlining their surveillance activities for HIV and AIDS; eliminating those which are perceived to return little usable data or substituting earlier activities with other sources of similar data, e.g. using HIV prevalence data from prevention screening of pregnant women in the place of HSS among ANC populations. The intention is to better direct limited surveillance resources and improve the quality and usability of the results. As many countries in the region are heavily dependent on external funding for HIV and AIDS programming,9 and there is uncertainty that current level of funding from development partners will continue,10 a decrease in the numbers and frequency of these resource-intensive surveys, such as probability surveys, in the future is likely. All countries would benefit from evaluating the design of their surveillance systems to clarify the utility of each surveillance component, including how different components work together to give a more in-depth picture of the epidemic in different regions of the country.
There is also a need to balance national analysis with subnational-level analysis and use of HIV and AIDS surveillance data. The substantial effort to generate national-level estimates and global reports, usually for donors, competes with the resources and time needed to conduct the same assessments at subnational-levels. These subnational analyses can highlight variations within a country and may be more likely to generate insight to guide effective prevention strategies. Countries should be supported to make decisions driven by their local epidemic context with surveillance data that allows for this.
To improve subnational analysis and use of surveillance data, it is essential that data collection and data analysis be integrated in the same unit with year-round attention to both. Data analysts and users need to coordinate well from the beginning. A clear understanding of how the data can or will be used can motivate more streamlined and efficient systems of data collection locally. Involvement of subnational-level programme staff in efforts to synthesize, triangulate and interpret data into national-level indicators may enhance the robustness of the results and consensus by all partners. Commitment from donors and technical agencies to support approaches to engage subnational partners in data analysis is also essential.
This assessment was based on publically available information and through communication with M&E and surveillance advisers for HIV and AIDS in country. Therefore it is likely that some activities may have been missed.
From the information collected in this assessment we can conclude that HIV surveillance systems in the Asia Pacific region are maturing; however, there are still opportunities for improving the collection and utilization of the data to understand and respond to the HIV epidemic.
None declared.
None.
The authors wish to acknowledge the contribution of the monitoring and evaluation advisers at the UNAIDS country offices in Asia Pacific for providing surveillance-related information for the Asia Pacific strategic information review in 2011 and reviewing the updated tables in the manuscript for accuracy.
{kind=link}
{kind=link}
{kind=link}