
a HIV/AIDS and STI, Division of Combating Communicable Diseases, World Health Organization Regional Office for the Western Pacific, Manila, Philippines.
b Department of HIV, World Health Organization, Geneva, Switzerland.
Correspondences to Yu Dongbao (e-mail: yud@wpro.who.int).
To cite this article:
Yu D et al. How are countries in the Western Pacific Region tracking the HIV epidemic? Results from a 2011 survey of ministries of health. Western Pacific Surveillance and Response Journal, 2012, 3(3):3-8. doi:10.5365/wpsar.2012.3.2.010
In 2011, as part of the World Health Organization global reporting tool to collect data on the progress of improving the health sector response to HIV/AIDS towards universal access, a questionnaire was sent to ministries of health of Western Pacific Region Member States on the scope and functioning of their HIV surveillance systems. Of the 17 countries that responded, 13 were low- to middle-income countries and four were high-income countries. Regular serosurveillance surveys are conducted with female sex workers in all lower- and middle-income countries that responded to the survey but less so with people who inject drugs and men who have sex with men. Furthermore, there are no surveillance activities of the key populations in most of the Pacific island countries. It is recommended that estimations of high-risk populations be conducted in priority Pacific island countries and tailored surveillance systems be designed. Efforts should also be made to gather and accumulate data from sufficient geographic coverage to allow the HIV epidemic to continue to be monitored.
An appropriate and effective national HIV surveillance system is necessary for countries to be able to understand and monitor the HIV epidemic and evaluate the national response. Such surveillance systems facilitate countries in estimating the magnitude of the epidemic, monitoring the trend of the epidemic, evaluating the effectiveness and outcome of health promotion efforts and advocating for commitment and resources. Countries in the Western Pacific Region have made significant progress in developing their HIV surveillance systems over the past years, but there are still important gaps. This includes surveillance data on high-risk groups such as men who have sex with men (MSM).1,2
Periodic assessment and review of countries' HIV surveillance systems are important to identify gaps and improve their performance, integration and long-term sustainability.3 There have been several reviews and assessments of HIV surveillance systems at global and regional levels, focusing on the different dimensions of surveillance such as flexibility and simplicity, usefulness, timeliness, data completeness and quality.4,5 Since 2007, the World Health Organization (WHO), together with United Nations Children's Fund (UNICEF) and Joint United Nations Programme on HIV/AIDS (UNAIDS), has been collecting national-level data from ministries of health to report on the progress of the health sector response to HIV/AIDS. In the 2011 country reporting, a set of programmatic questions related to the functioning of routine serosurveillance systems in countries were included, providing a snapshot of the scope and operation of HIV surveillance systems. This included the major populations, periodicity and geographic location covered by the surveillance systems, the most recent sexual and injecting drug behaviour surveys and any surveillance of HIV drug resistance.
In this paper, we report on the data from the 2011 survey for the Western Pacific Region. This assessment does not intend to be a comprehensive evaluation of HIV surveillance systems or a detailed account of sampling and reports, but it provides the most recent updates of the scope and functions of countries' surveillance systems as reported by the countries themselves.
In 2011, a questionnaire was sent to ministries of health of Western Pacific Region Member States on the scope and functioning of their HIV surveillance systems. It included questions on the coverage of population groups by routine serosurveillance surveys, determining whether sexual and drug use behaviour surveys or demographic health surveys with HIV testing had been conducted and whether of any surveillance of HIV drug resistance had been implemented.
A total of 17 countries from the Western Pacific Region submitted their data. Thirteen were from lower- and middle-income countries: Cambodia, China, Fiji, Kiribati, the Lao People's Democratic Republic, Malaysia, Mongolia, Papua New Guinea, the Philippines, Samoa, Solomon Islands, Tonga and Viet Nam; four were from high-income countries: Australia, Brunei Darussalam, New Zealand and Singapore. Epidemiologic and programmatic data on antiretroviral therapy (ART), prevention of mother-to-child transmission, prevention with key populations and other indicators have been published previously.6
The survey results were reported for lower- and middle-income countries, separately for Asian and Pacific island countries, and for high-income countries.
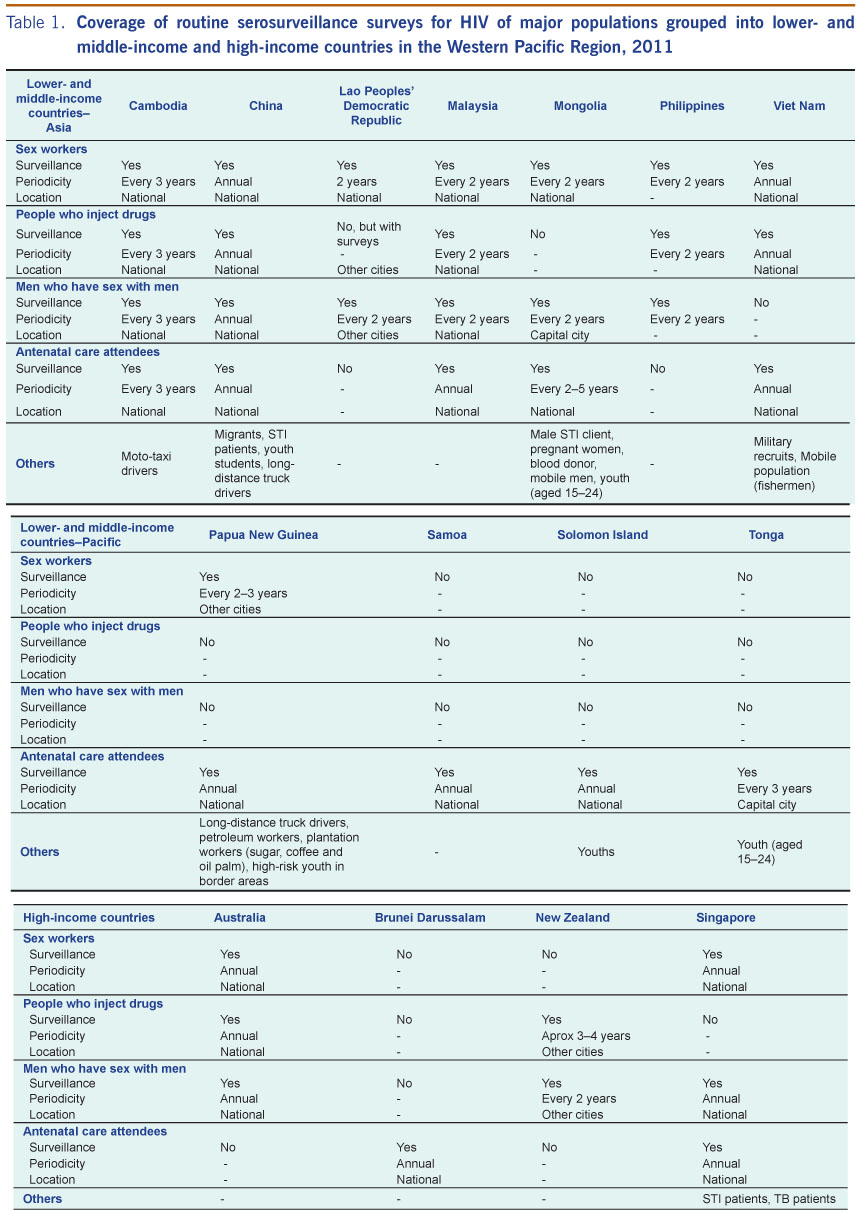
All the Asian lower- and middle-income countries reported that routine serosurveillance surveys have been in place for female sex workers (FSW). Most countries conduct these surveys every two to three years, except for China and Viet Nam where they are conducted on a yearly basis.
Among the Pacific island countries, only Kiribati and Papua New Guinea report routine serosurveillance for FSW every two to three years. For other Pacific island countries, including Fiji, Samoa, Solomon Islands and Tonga, no serosurveillance was conducted for FSW.
Among the high-income countries, Australia and Singapore reported routine serosurveillance for FSW, while Brunei Darussalam and New Zealand do not conduct surveys for this population (Table 1).
Among the Asian countries, China and Viet Nam conduct routine, annual serosurveillance of people who inject drugs (PWID), while Cambodia, Malaysia and the Philippines use a two-to-three-year cycle. The Lao People's Democratic Republic conducts sporadic serosurveillance among PWID in cities other than the capital. Mongolia does not conduct serosurveillance of PWID.
For the Pacific island countries, only Kiribati reported conducting routine serosurveillance of PWID in cities other than the capital on a three-year basis.
For the high-income countries, Australia and New Zealand reported routine serosurveillance of PWID - annually at the national level in Australia and in cities other than the capital in three-to-four-year intervals in New Zealand (Table 1).
Among the Asian countries, Cambodia, China, the Lao People's Democratic Republic, Malaysia, Mongolia and the Philippines reported routine serosurveillance surveys of MSM. Viet Nam notably reported no routine surveys for this population group. For Pacific island countries, only Kiribati reported conducting routine serosurveillance among MSM. It is notable that Papua New Guinea does not conduct these surveys among MSM.
For the high-income countries, Australia, New Zealand and Singapore reported conducting routine serosurveillance of MSM on an annual or biennial basis (Table 1).
Among the Asian countries, only the Lao People's Democratic Republic and the Philippines reported not conducting routine serosurveillance for antenatal care (ANC) attendees. China and Viet Nam both reported annual serosurveillance of ANC patients, while the other Asian countries conduct ANC serosurveillance every two to five years.
All the Pacific island countries reported conducting annual serosurveillance of ANC attendees, either at the national level or in capital cities.
For the high-income countries, Brunei Darussalam and Singapore implement routine serosurveillance to ANC attendees while Australia and New Zealand do not (Table 1).
Routine serosurveillance of other populations was reported according to the epidemic situation in each country. For example, China, Fiji, Mongolia and Singapore include sexually transmitted infection (STI) clinic attendees in their routine serosurveillance. Long-distance truck drivers and taxi drivers are under regular serosurveillance in Cambodia, China and Papua New Guinea. Military recruits and police are monitored in Fiji and Viet Nam. Migrant populations are targeted for serosurveillance in several countries, including China, Fiji (seafarers), Mongolia, Papua New Guinea and Viet Nam. Youth are also under periodic serosurveillance in China, Fiji, Mongolia, Papua New Guinea, Solomon Islands and Tonga. It is noteworthy that Singapore conducts periodic HIV serosurveillance among tuberculosis patients (Table 1).
In addition to the routine serosurveillance of the high-risk groups reported above, several countries also conduct sexual and drug use behaviour surveys for these population groups. Among the lower- and middle-income countries, China conducts annual surveys on sexual and drug use behaviours for the different at-risk populations; the most recent surveys in other countries were conducted in 2008 through 2010.
Among the Pacific island countries, Kiribati and Papua New Guinea reported surveys on sexual and drug use behaviours of key populations at the same time as serosurveillance.
For the high-income countries, Australia conducts a sexual and drug use behaviour survey of PWID on an annual basis. The most recent behaviour survey data for Singapore were collected in 2007 among university students, the general population and STI clinic attendees.
Four low HIV prevalence countries - Kiribati, Mongolia, the Philippines and Samoa - reported that demographic and health surveys (DHS) with HIV testing have been carried out among the general population. The DHS reports are publicly available for the Philippines7 and Samoa,8 although the HIV testing results were not reported.
The four Asian countries with the highest number of people on ART - Cambodia, China, Papua New Guinea and Viet Nam - have implemented one or more elements of HIV drug resistance (HIVDR) strategies: development of HIVDR prevention and assessment strategies, HIVDR early warning indicators, data collection, monitoring survey of patients on ART, HIVDR transmission survey among recently infected individuals and preparation of annual HIVDR report and recommendations. In other countries, there are no major HIVDR surveillance activities.
Countries in the Western Pacific Region all have concentrated or low-level HIV epidemics, where the high-risk behaviour of key populations, particularly FSW, PWID and MSM, drive the epidemics. HIV surveillance for low-level and concentrated epidemics should include estimates of the population size of these key populations and routine HIV serosurveillance and behavioural surveys among them. These should be regularly assessed and evaluated so they can be adapted to any changes in the HIV epidemic situation and response from countries.9
This study shows that in 2011, most Asian countries were adequately tracking their HIV epidemics, although there are gaps in tracking the key populations in most Pacific island countries. Serosurveillance had been established for FSW in most Asian countries, although there were gaps for surveillance among PWID and MSM. For example, Viet Nam does not conduct routine surveillance for MSM, despite this being a high-risk group for HIV. Despite these surveillance efforts it can be difficult to determine the HIV trends among different population groups in some countries due to the insufficiency of data and limited geographic coverage of these surveys. For example, the Lao People's Democratic Republic conducted some surveys of PWID but not in a consistent and continuous manner. Asian countries are encouraged to continuously and consistently conduct surveillance among these populations and expand the geographic coverage.
In the Pacific island countriess, surveillance activities in most countries focus on ANC attendees, although Kiribati and Papua New Guinea did report surveillance of FSW, with Kiribati also reporting surveillance of PWID and MSM. Fiji also reported surveillance of other high-risk groups. Using ANC attendees is not recommended for low-level HIV epidemic countries and is done as ANC data are easy and convenient to collect. There is a lack of capacity of the surveillance systems to track other at-risk populations in these countries. Therefore it is recommended that mapping of high-risk populations should be conducted in priority Pacific island countries, and if these high-risk behaviour groups are indeed existing and active, tailored surveillance systems should be designed to track the HIV epidemic and risk behaviours. As STIs are especially high in many of the Pacific island countries,10 active surveillance of STIs and HIV among groups with risk behaviours is warranted. Furthermore, greater efforts should be made to strengthen HIV testing and counselling and HIV and STI case reporting in the Pacific island countries.
DHS with HIV testing has been reported as implemented in several low prevalence countries, but data are not available in the public domain. As for surveillance of ANC attendees, this may not be a suitable method for these low epidemic countries as it requires HIV testing of very large samples. As most HIV cases are found within the key populations, a more targeted approach might be better.
HIV drug resistance surveillance was reported from the four countries with the highest number of people on ART, and this is essential to optimize ART delivery. The implementation, however, needs to be strengthened in this Region, as has been extensively discussed by a recent systematic review.11
There are several limitations to this report. Not all countries responded to the survey; therefore, the representativeness of the results might be affected. Moreover, it is based on self-reported results, which might be affected by the understanding of the questions, leading to possible misreporting. There are several other issues that this current survey could not cover but that are important for countries' surveillance systems. In some countries, surveillance surveys are conducted in facilities such as detention centres and STI clinics using convenient sampling. The representativeness could be improved with better sampling methods, such as respondent-driven sampling or time-location cluster sampling. There is also the need for better mapping and size estimation of the key populations in some countries, especially in the Pacific island countries. Improvement in the consistency of methods, data quality and data use for the surveillance activities is also needed.
None declared.
This study was undertaken as part of routine activities of the World Health Organization Regional Office for the Western Pacific.
We thank the Member States in the Western Pacific Region for responding to the survey in 2011.
{kind=link}