a Field Epidemiology Training Program, National Institute of Infectious Diseases, Tokyo, Japan.
b Division of Quarantine and Sanitation, Chubu Airport Quarantine Branch, Nagoya Quarantine Station, Aichi, Japan.
c Emerging Diseases Surveillance and Response Unit, Division of Health Security and Emergencies, World Health Organization Regional Office for the Western Pacific, Manila, Philippines.
d Infectious Disease Surveillance Center, National Institute of Infectious Diseases, Tokyo, Japan.
e Kawasaki City Institute for Public Health, Kanagawa, Japan.
Correspondence to Naomi Nakamura (e-mail: nakana@nih.go.jp).
To cite this article:
Nakamura N et al. Incidence of dengue virus infection among Japanese travellers, 2006 to 2010. Western Pacific Surveillance and Response Journal, 2013, 3(2):39-45. doi:10.5365/wpsar.2011.2.3.002
Introduction: Dengue continues to be a global public health concern. In Japan, although dengue cases are currently seen only among travellers returning from endemic areas, the number of reported cases is rising according to the national case-based surveillance system. We evaluated the characteristics of dengue cases imported into Japan and the relationship between the incidence of infection and season of travel to popular destinations.
Methods: Dengue cases reported to the national surveillance system were retrospectively examined. The number of reported cases per number of Japanese travellers to a dengue-endemic country was calculated to estimate the country-specific incidence of imported dengue virus infection. The incidence of dengue infection among Japanese travellers was compared between dengue high season and low season in each country using relative risk (RR) and associated 95% confidence intervals (CI).
Results: Among 540 Japanese residents who were reported as dengue cases from 2006 to 2010, the majority had travelled to Indonesia, India, the Philippines and Thailand. The RR of dengue infection among Japanese travellers during dengue high season versus low season was 4.92 (95% CI: 3.01–8.04) for the Philippines, 2.76 (95% CI: 1.67–4.54) for Thailand and 0.37 (95% CI: 0.15–0.92) for Indonesia.
Discussion: Overall, higher incidence of imported cases appeared to be related to historic dengue high seasons. Travellers planning to visit dengue-endemic countries should be aware of historic dengue seasonality and the current dengue situation.
Dengue fever (DF) has rapidly spread over the last few decades and is currently found in most tropical and subtropical areas throughout the world.1 In Japan, according to the national case-based surveillance system, the number of reported DF cases has been steadily increasing, from fewer than 50 cases in 2006 to more than 200 cases in 2010. It is thought that there is no dengue transmission in Japan and that all reported cases are among those who returned from endemic countries. However, one of the mosquito vectors for dengue, Aedes albopictous, inhabits Japan and a major outbreak in western Japan occurred between 1942 and 1945.2 As rapid globalization has accelerated international travel and trade, there is a growing fear that secondary transmission will cause a dengue outbreak in Japan, as documented in Australia3,4 and France.5
In Japan, DF and dengue haemorrhagic fever (DHF) have been notifiable diseases regulated by the Infectious Disease Control Law since April 1999. Physicians in all clinics and hospitals are required to report demographic information and clinical and exposure history about every patient meeting the DF/DHF case definitions (Box 1) to the nearby public health centre. The data are reported by local governments to the Ministry of Health, Labour and Welfare and the Infectious Disease Surveillance Center (IDSC), National Institute of Infectious Diseases (NIID).
To estimate the incidence of dengue virus infection among Japanese travellers, we described the characteristics of dengue cases reported to the national case-based surveillance system and the relationship between the incidence of dengue infection and season of travel.
Using the Japanese reportable disease surveillance data, the epidemiological characteristics of reported DF and DHF from 2006 to 2010 were described.6
To estimate the country-specific annual incidence of imported dengue virus infection among Japanese travellers, the number of reported cases returning from an endemic country for a given year was divided by the number of travellers that visited that country in that year. Countries were included if there were more than 50 reported cases from that country over the study period; cases were excluded if they had a home address outside of Japan or they had reported visiting multiple destinations (i.e. more than one country). International traveller data among the Japanese population were obtained for the Philippines and Thailand from the Japan Tourism Marketing Company,7 and for Indonesia and India from the relevant ministries of receiving countries.8,9 For Indonesia, international traveller data were only available from 2007 to 2010. Travellers from Japan were based on nationality, except for the Philippines, which were based on residency. Information on visit duration and areas visited in the destination countries was not available.
Country-specific aggregated monthly incidence was calculated in the same manner but over a period of one calendar month, and the data for each month were aggregated over the period 2006–2010. Monthly data were summed over these years as the number of cases reported for each month was small and the monthly pattern remained consistent. Monthly data for Japanese travellers were unavailable for India9 and only available for 2010 for Indonesia.8
Historical dengue seasons are from January to February in Indonesia, June to August in Thailand, August to November in India10 and July to October in the Philippines.11 The incidence of infection among Japanese travellers was compared between dengue high season and low season months. This comparison was calculated as a relative risk (RR) and associated 95% confidence intervals (CI).
There were a total of 589 reported cases between 2006 and 2010 - 565 of DF and 24 of DHF. Three hundred eighty-two cases (64.9%) were male and the median age was 29 years (range: eight months to 90 years). The largest proportion of cases were among those aged 20–29 years (239/589 [40.6%]) and 30–39 years (126/589 [21.4%]). Of the 24 cases classified as DHF, 17 cases were male and the median age was 32 years (range: one to 64 years); information on previous history of DF was unknown.
Laboratory confirmation was made by the following methods: virus isolation (60/589 [10.2%]), virus-specific nucleic acid sequences by PCR (295/589 [50.1%]) and positive IgM antibody in serum (346/589 [58.7%]); 49/589 [8.3%] tested positive by multiple methods. Information regarding clinical symptoms was available for 581 cases (557 DF and 24 DHF). Among DF cases, the following were reported: fever (551/557 [98.9%]), thrombocytopenia (369/557 [66.2%]), headache (320/557 [57.5%]), leukocytopenia (308/557 [55.3%]) and rash (293/557 [52.6%]). All 24 cases of DHF reported all four symptoms as per the case definition.
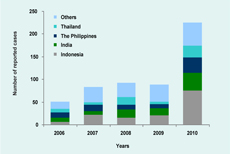
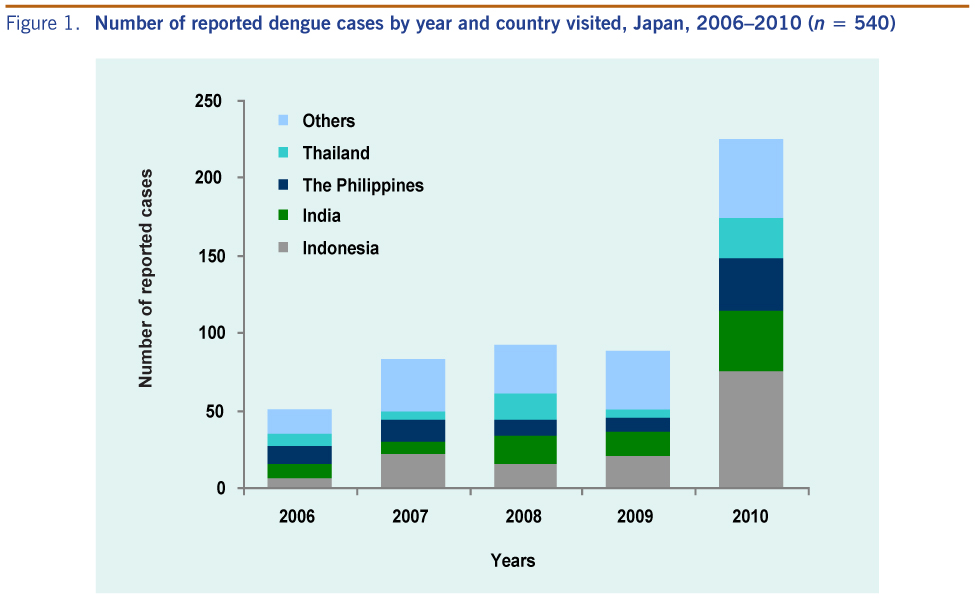
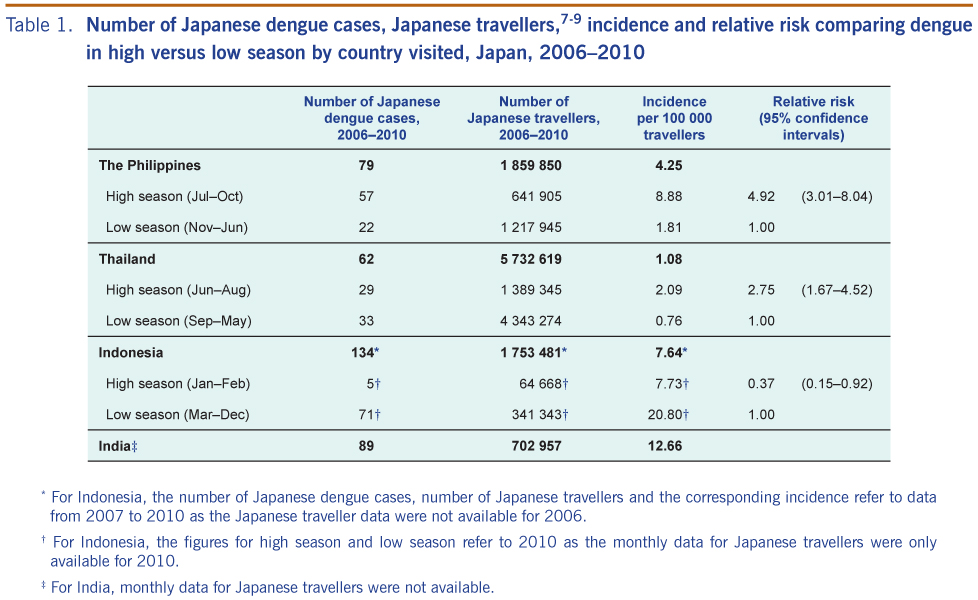
Among the 589 cases, 15 had home addresses outside of Japan and 34 had visited multiple destinations. Of the remaining 540 cases, 491 (90.9%) were associated with travel within Asia. Twenty-seven (5.0%), 14 (2.6%), seven (1.3%) and one (0.2%) were associated with travel to Latin America and the Caribbean, Australia and Oceania, Africa and the Middle East, respectively. The countries with the largest number of reported Japanese dengue cases were Indonesia (141 cases [26.1%]), India (89 cases [16.5%]), the Philippines (79 cases [14.6%]) and Thailand (62 cases [11.5%]) (Figure 1). In terms of estimated incidence of imported dengue virus infection among Japanese travellers, India was highest, followed by Indonesia, the Philippines and Thailand (Table 1).
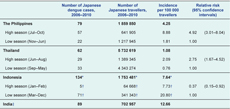
* For Indonesia, the number of Japanese dengue cases, number of Japanese travellers and the corresponding incidence refer to data from 2007 to 2010 as the Japanese traveller data were not available for 2006.
† For Indonesia, the figures for high season and low season refer to 2010 as the monthly data for Japanese travellers were only available for 2010.
‡ For India, monthly data for Japanese travellers were not available.
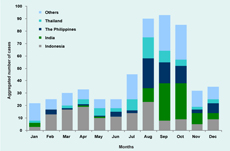
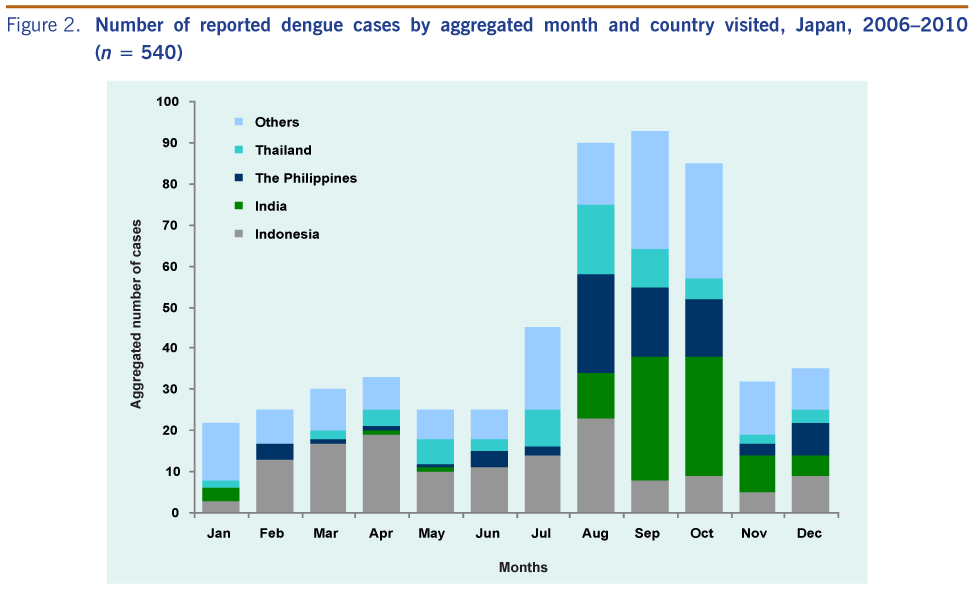
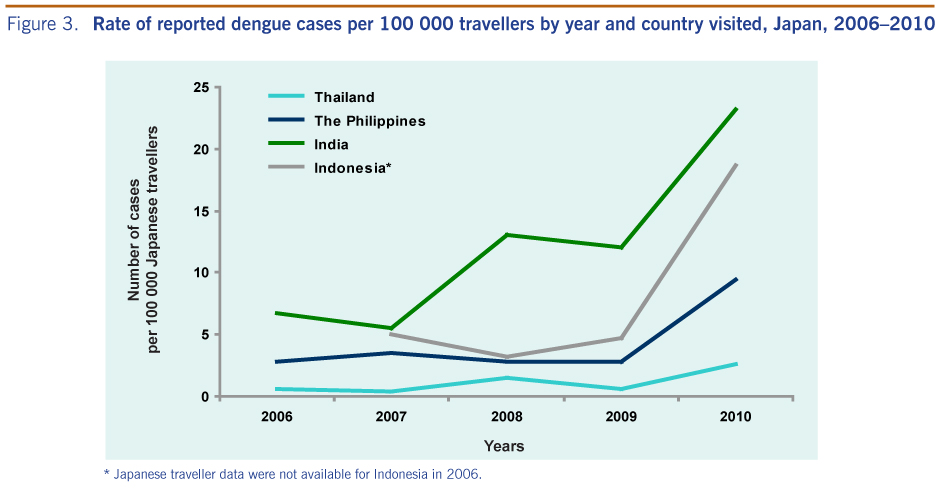
The aggregated number of cases by month from 2006 to 2010 showed that travel among the reported cases was most common during August through October (Figure 2). Among the reported cases, travel to Indonesia, Thailand and the Philippines was highest in August, while travel to India was highest in September. The annual country-specific incidence of imported cases per 100 000 Japanese travellers indicated a considerably higher incidence in 2010 relative to previous years (Figure 3).
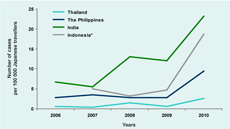
* Japanese traveller data were not available for Indonesia in 2006.
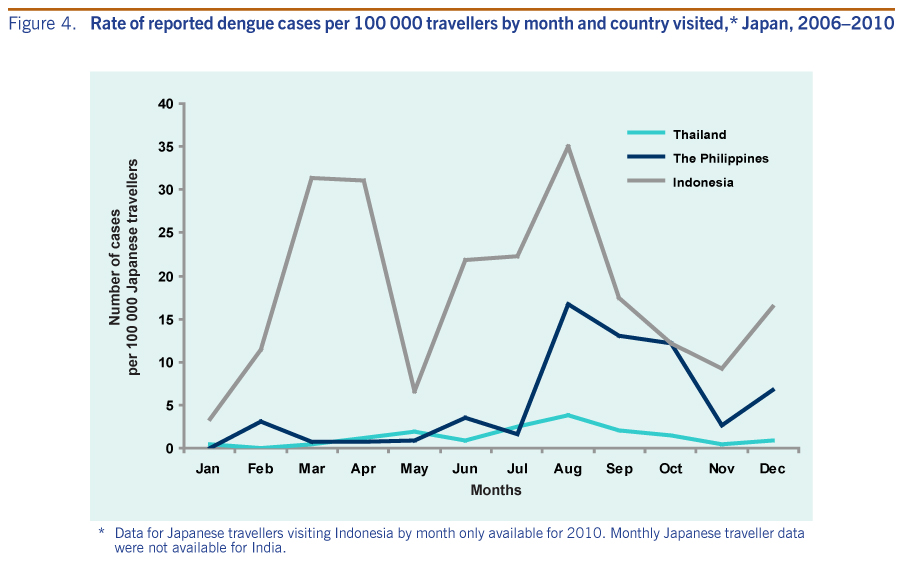
The aggregated monthly data from 2006 to 2010 showed that the monthly incidence of dengue infection among Japanese travellers to the Philippines, Indonesia and Thailand were highest in August (Figure 4). The incidence of dengue infection among Japanese travellers during high versus low season was significantly higher for the Philippines and Thailand but significantly lower for Indonesia (Table 1).
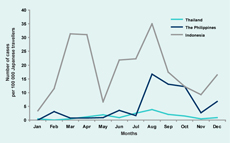
* Data for Japanese travellers visiting Indonesia by month only available for 2010. Monthly Japanese traveller data were not available for India.
The global incidence of dengue has grown dramatically in recent decades.1 In the World Health Organization (WHO) South-East Asian Region and WHO Western Pacific Region, the incidence has also been increasing.10,11 While the number of overseas Japanese travellers has recently been slightly declining,12 the number of reported dengue cases in Japan has been increasing overall. This study shows the majority of dengue cases notified in Japan were imported from Asia, especially Indonesia, India, the Philippines and Thailand; both the number of reported cases from those countries and the incidence among Japanese travellers from those countries increased in 2010.
Most of the cases were reported from August to October, which corresponds with late summer vacation season in Japan. Moreover, the incidences of imported cases from the Philippines and Thailand were significantly higher during the historic dengue high season relative to the low season. Peak incidence among travellers to Indonesia in 2010 (i.e. August) was not associated with travel during the historic high season (i.e. January and February). However, analysis for Indonesia was limited as monthly data were available only for 2010 and the high incidence also observed in March is temporally close to the historic peak season during January and February.10 In addition, a recent study of reported dengue cases in Bali from 2005 to August 2010 indicated a particularly high number of cases from March to July 2010.13 As Bali is one of the most popular Japanese travel destinations in Indonesia, with 61% of Japanese travellers to Indonesia visiting Bali in 2010, it is possible that the second peak in August 2010 may have been associated with the high activity observed in Bali from March to July 2010. Therefore, it is important that travellers planning to visit dengue-endemic countries be aware of the historic dengue high seasons and the current local dengue situation.
Surveillance data from exported traveller cases should be reported not only to the local populations in the endemic countries but also to the international community. While there are various studies of travel-related dengue infection, several studies of imported cases have been useful in suggesting the existence of local DF outbreaks in endemic areas.14,15 In 2008, for example, a dengue case was imported from Côte d’Ivoire to Japan and tested DENV-3 positive. Following this case and another case in France, an international alert was issued because DENV-3 had never been reported in West Africa before.16 The practice of timely information sharing of the dengue situation among endemic countries has recently been facilitated through the WHO Western Pacific Regional Office.17
There are several important limitations in our study. There is concern whether the reported cases truly arose from the traveller population. While we excluded cases reported to the national surveillance system that had home addresses outside of Japan, their nationalities were not identified. As the population that travelled from Japan to the destination countries was based on nationality (except for the Philippines, which was based on residency), there is a possibility that some of the cases captured by the Japanese national surveillance system did not arise from the traveller population considered at risk.
Our study might be underestimating the risk of dengue infection for Japanese travellers. Dengue infection has a broad spectrum of presentation, and dengue patients with only mild symptoms might not seek medical attention. In addition, while the national surveillance system requires reporting of all dengue cases from all medical doctors in Japan, as dengue is not endemic, the disease might be misdiagnosed and not reported.
Specific information on the travellers’ behaviours, detailed information on locations visited and duration of visit, which may influence the risk of dengue infection, were not available. For example, specific activities of the visitors, such as exploration/adventure-themed travel, may have accounted for some of the recent increase in reported dengue cases. In addition, while there were nearly twice as many male than female cases during the period 2006–2010, the lack of sex-stratified traveller information limited our ability to assess differential risk due to sex.
However, despite these limitations, the higher incidence of infection associated with travel to dengue- endemic countries during historic epidemic seasons is an important public health finding from this study. Although imported dengue cases may not be representative of local cases in endemic countries (among overseas Japanese travellers, tour groups are popular and such groups may stay and visit specific tourist locations not frequented by the local population), this study nevertheless suggests that travellers are more likely to contract dengue during historic dengue high seasons in endemic countries. Travellers should thus be advised to be aware of dengue, especially during historic peak seasons. Communicating such seasonality to medical practitioners could also be beneficial in enhancing their awareness for appropriate diagnosis and treatment. In addition, travellers and medical practitioners should also both be aware of the current dengue situation.
Given the continued increase in both global dengue incidence and global travel, sustained dengue surveillance for both endemic and exported dengue cases, enhanced awareness among travellers and clinicians and international information sharing are essential for combating the global dengue threat.
None declared.
None.
We would like to thank the staff of local health centres and public health institutes/laboratories all over the country for regularly reporting dengue cases and kindly answering our inquiries.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}