
a Medical Services Promotion Division, Iwate Prefecture Government, Japan (e-mail: m-nohara@pref.iwate.jp).
To cite this article:
Nohara M. Impact of the Great East Japan Earthquake and tsunami on health, medical care and public health systems in Iwate Prefecture, Japan, 2011. Western Pacific Surveillance and Response Journal, 2011, 2(4):24-30. doi:10.5365/wpsar.year.2011.2.4.002
Problem: The Great East Japan Earthquake was one of the largest earthquakes ever recorded in global history. The damage was spread over a wide area, with the worst-hit areas being Iwate, Miyagi and Fukushima prefectures. In this paper we report on the damage and the impact of the damage to describe the health consequences among disaster victims in Iwate Prefecture.
Context: In Iwate Prefecture the tsunami claimed 4659 lives, with 1633 people missing. In addition to electricity, water and gas being cut off following the disaster, communication functions were paralysed and there was a lack of gasoline.
Action: Medical and public health teams from Iwate Prefecture and around the country, including many different specialists, engaged in a variety of public health activities mainly at evacuation centres, including medical and mental health care and activities to prevent infectious diseases.
Outcome: Given the many fatalities, there were relatively few patients who required medical treatment for major injuries. However, there were significant medical needs in the subacute and chronic phases of care in evacuation centres, with great demand for medical treatment and public health assistance, measures to counteract infection and mental health care.
Discussion: By referring to past experiences of national and international large-scale disasters, it was possible to respond effectively to the health-related challenges. However, there are still challenges concerning how to share information and coordinate overall activities among multiple public health response teams. Further examination will be required to ensure better preparedness in response to future disasters.
The Great East Japan Earthquake struck Japan on 11 March 2011, with an epicentre off the Sanriku coast (latitude 38°6.2', longitude 142°51.6', depth 24 km).1 It was one of the largest earthquakes ever recorded in global history (magnitude 9.0) and was compounded by the further disasters of an enormous tsunami, fires and an accident at a nuclear power station in Fukushima Prefecture. The damage was spread over a wide area, with the worst-hit areas being Iwate, Miyagi and Fukushima prefectures. While the impact of the damage from the earthquake in terms of human cost and destroyed structures was relatively light, the tsunami almost entirely obliterated the coastal regions (Figure 1).
* Reproduced with permissions from the Iwate Prefectural Government
In this paper we report on the damage and its impact to describe the health consequences among disaster victims in Iwate Prefecture who were subject to damage from the tsunami. We also detail the public health and sanitation activities that were implemented by the Iwate prefectural government and various other health-related organizations.
Although the severity of the impact of the earthquake itself varied from region to region, it affected an extremely large area of eastern Japan. The subsequent tsunami brought about catastrophic damage to the three prefectures of Fukushima, Miyagi and Iwate and in particular the area from the southern part of Miyagi Prefecture to the coastal regions of Iwate Prefecture. This is because of the geographical characteristics of the region which has a series of peninsulas and deep bays and inlets that are referred to in geographical terms as a “ria” coast.
The structure of this coastline means that when a tsunami strikes it tends to increase greatly in height once it reaches the coast. Due to the “ria” coast characteristics of the Iwate Prefecture coastline, at its highest point the tsunami reached a height of approximately 38 m, and damage was spread along a 600 km stretch of the coast.
Due to these geographical characteristics, the Tohoku region has had previous experience with large-scale tsunami damage, and it was perhaps the best-prepared region in the world for tsunami countermeasures, including the presence of large-scale coastal levees and breakwaters and the implementation of evacuation training for residents. However, this massive natural disaster, said to be a once-in-a-thousand-year event, inflicted a tremendous human cost in this region.
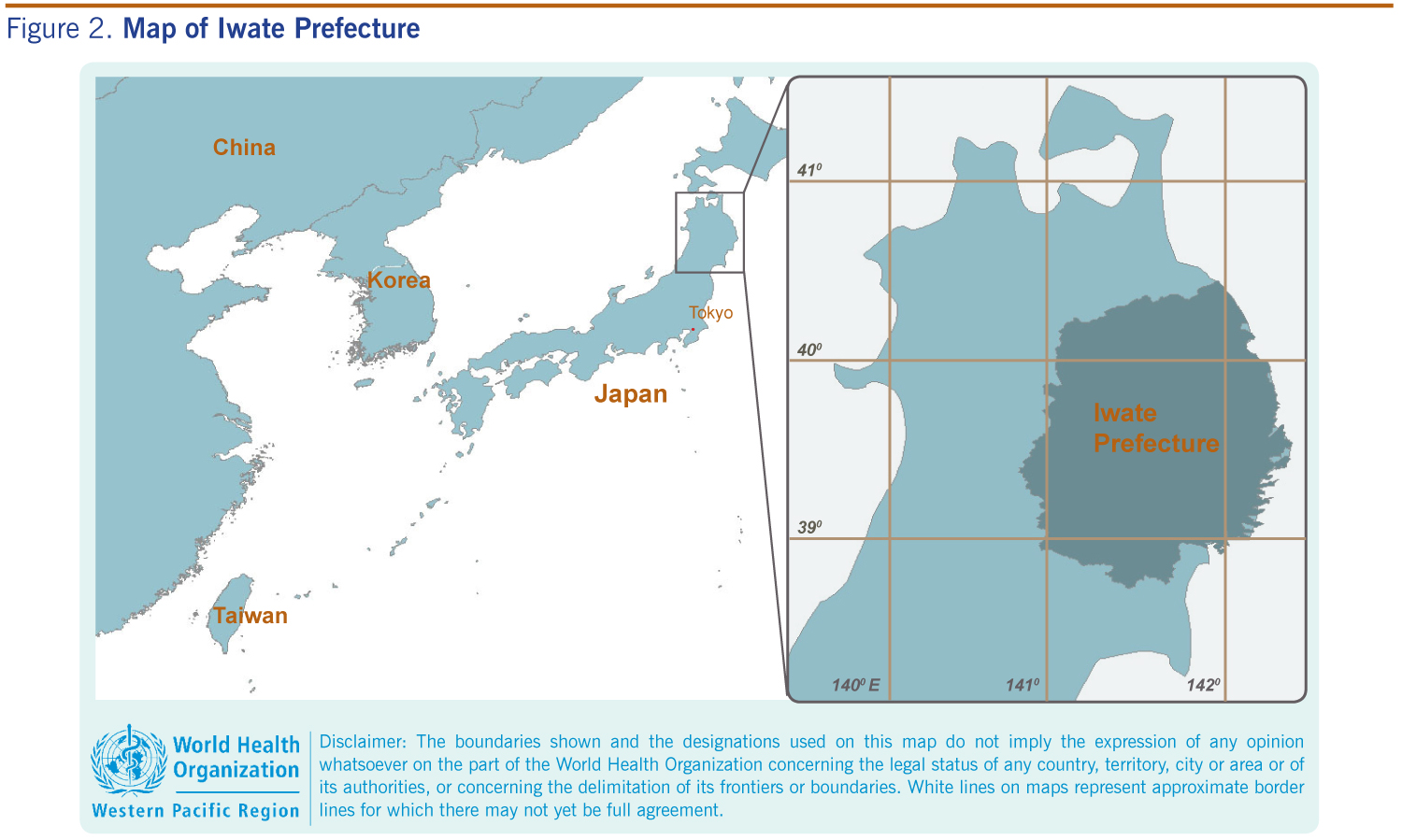
Iwate Prefecture is situated in the north-east of Honshu, the main island of Japan, and is the second largest prefecture after northernmost Hokkaido, accounting for 4% of Japan’s total land mass (Figure 2). It has a population of 1.33 million. The people of the coastal regions of Iwate that were hardest hit are predominantly engaged in the fisheries industry. The proportion of the population over 65 years of age stands at 30%, greater than the national average of 20%, with the aging of the population continuing to progress. In comparison to other regions the Iwate Prefecture has relatively few human resources in terms of health and welfare practitioners, including doctors.2,3
As of 21 September 2011, six months after the disaster struck, the official number of victims in Japan was 15 799 dead and 4041 missing.4 The fatalities were approximately three times the number claimed by the Great Hanshin-Awaji Earthquake (1995), which was the largest natural disaster in recent times until 2011. The number of casualties in Iwate Prefecture alone stands at 4659 dead and 1633 missing.5
Electricity, water and gas were all cut off in the disaster. Although these were restored in two or three days to inland areas that escaped tsunami damage, in the coastal areas it took approximately one-and-a-half months for electricity to be restored and four months for the water supply.
All normal means of communication were also lost in the disaster and in the initial aftermath (approximately two weeks) only satellite mobile phones functioned (and these did not always work effectively). It was for this reason that in the initial post-disaster period local governments were severely restricted in their attempt to assess and evaluate the status of the damage.
There was no public transportation in the coastal areas. Although most of the local residents had used vehicles to go about their daily lives, many of these were washed away in the tsunami. In addition, roads were damaged or blocked, meaning that access to and travel within the disaster regions were very difficult.
The inland cities that were expected to provide backup functions in times of emergency almost exclusively relied on vehicular transportation for assistance activities (excluding air transport); following the disaster, travel between the inland and the coast took between two and three hours. In addition, there was an initial lack of gasoline, and health and welfare workers experienced difficulties in procuring gasoline for their vehicles to go about their health and medical support activities.
In the coastal areas of Iwate Prefecture, three hospitals were entirely destroyed by the tsunami, and approximately half of all clinics and other health facilities were damaged in some way. Many local government personnel, including public health personnel, were affected by the disaster also, resulting in local government functions, which are expected to play a central role in post-disaster response, being entirely paralysed or severely restricted.
In the coastal areas of Iwate Prefecture, there are four hospitals designated as disaster base hospitals that are expected to perform a central role in the provision of medical care following a disaster. Fortunately, these hospitals escaped major damage and were able to provide emergency medical care following the disaster, including initial patient triage, emergency response and transportation of patients to inland areas.
A total of 128 Disaster Medical Assistance Teams (DMATs), consisting of one to two physicians, one to two nurses and one administrator, came to the assistance of Iwate Prefecture for a nine-day period beginning 11 March 2011, engaging in emergency medical care and patient transportation activities and other duties. These teams provided transportation via helicopter to inland areas and established a wide-area distribution centre and staging care unit (a temporary medical facility for emergency medical evaluation outside of affected areas), at Hanamaki Airport further inland from where they provided wide-area transportation and distribution services via aircraft to medical facilities both inside and outside Iwate Prefecture.
Taking on the work of medical activities performed by DMATs in the post-disaster acute phase, medical assistance teams (Japanese Red Cross Society, Japan Medical Association, etc.) provided medical care mainly at evacuation centres from the subacute through to the chronic phases of operations. In early April, a maximum of 58 teams were engaged in activities in Iwate Prefecture. Their number gradually decreased as local medical facilities reopened and evacuation centres were closed. Medical assistance from outside the prefecture was ultimately concluded at the end of July 2011.
At the peak period there were a total of 399 evacuation centres in Iwate Prefecture and a total of 54 429 evacuees. Following the completion of temporary accommodations, all the evacuation centres were closed by mid-August 2011.
In addition to medical teams, many public health and sanitation teams engaged in activities in the disaster areas. These included health maintenance activities by public health nurses, mental care from psychiatrists and clinical psychologists, oral care by dentists, as well as support from pharmacists, certified nurses, occupational therapists and physiotherapists.
In areas where damage was relatively slight, as of September 2011, the public health and sanitation systems were gradually recovering and accordingly assistance from outside the prefecture was being reduced.
Current public health and sanitation assistance activities shifted from evacuation centres to home-based care by mid-August 2011, both for residents living in their own homes and also those in temporary accommodation.
There are many residents who continue to require assistance in the form of mental health care, and as there are few local human resources who can provide mental health care, it is expected that external assistance will be required in the long term.
Since many of the evacuation centres had lost basic infrastructures, resulting in no power or water for drinkingand sanitation purposes, there was a marked downturn in the state of sanitation. Iwate Prefecture provided sufficient bottled water for drinking. However, clean water for hand washing and water for toilets was insufficient. In addition, there was damage to the sewage system.
In the largest evacuation centres, almost 1000 evacuees were living together, and they were joined by many volunteers coming and going. In addition, since the disaster struck during the season for influenza and infectious gastroenteritis, there was an extremely high risk of outbreaks of infectious diseases becoming epidemic. It was necessary to implement a strategy whereby the signs of an infectious outbreak could be detected at an early stage and swift intervention measures implemented. Infection control assistance teams organized by experts in infectious diseases from within the prefecture were launched. They implemented Daily Surveillance for Outbreak Detection using mobile terminals in 40 large-scale evacuation centres. These teams also provided assistance with improving the disease–resistant environments in evacuation centres and providing infection control measures. These measures included evaluation of sanitary condition of evacuation centres, training for hand hygiene for public health workers/evacuees, instruction for infection control (e.g. isolation and prophylaxis for infectious disease cases), information-sharing about infectious disease and prevention and procurement of disinfectants.
In contrast to the 1995 Great Hanshin-Awaji Earthquake, in which there were 6434 fatalities and 43 792 people injured, in Iwate Prefecture following the Great East Japan Earthquake there was a remarkably small number of individuals injured compared to those that died. There were 6322 fatalities (4659 dead and 1633 missing) and only 188 people reported injured5 (based on reports from municipal governments).
These figures clearly show the characteristics of tsunami damage: relatively few casualties caused by falling structures in the earthquake, and approximately 90% of the deaths caused by drowning.6
Through 18 March 2011, a total of 191 patients were airlifted to Hanamaki Airport in Iwate Prefecture, and 16 were transferred to medical facilities outside the prefecture. The patient breakdown was 101 females and 90 males, with an average age of 54.4 years (0–100 years). In addition to conditions caused directly by the disaster, such as broken bones, external injuries, water inhalation and hypothermia, there were other medical needs including care for pregnant women and dialysis patients.
Given the many fatalities, there were relatively few patients who required medical treatment for external injuries caused by the disaster, particularly in view of the scale of the disaster itself. However, there were significant medical needs in the subacute and chronic phases of care in evacuation centres, with great demand for medical treatment and public health, sanitation assistance for general disorders, measures to counteract infection and mental health care.
The conditions and health status in the disaster-affected areas that should be mentioned in particular are as follows:
Local municipalities with detailed knowledge of the local situation are usually expected to devise a disaster prevention plan and play a central role in disaster response with the assistance of the prefectural government. However, in this disaster, many local officials including public health personnel lost their lives, and those who survived engaged in disaster response in a situation in which they themselves were disaster victims. Although it is local government personnel who are expected to take the lead in formulating plans for the reconstruction of towns and ensuring the restoration of the public health sector, it is likely that long term sustained assistance from external sources will be required in terms of human resources, and financial and technological assistance.
As Iwate Prefecture had experienced large earthquakes over the course of several years, the initial disaster medical response was well prepared in the form of manuals and implementation of training. Preparations among the relevant organizations and institutions were also in place to respond to earthquake and tsunami disasters. Although the recent disaster exceeded assumed scenarios, the response to it ran smoothly overall, including the mobilization of DMAT, transportation of patients and establishment of a staging care unit according to the pre-designed emergency plan, although several individual issues and challenges remain.
Challenges for the initial medical response to disaster include: (1) difficulty in transmitting information quickly and accurately due to the disruption of means of communication, (2) securing medical and food supplies at medical facilities, and (3) securing fuel for electricity generators and gasoline for vehicular transport.
The damage caused by the disaster covered a wide area, and evaluation of the public health and sanitation aspects of many evacuation centres was also required. Although assistance was provided by many health experts for the maintenance of medical care and ensuring the health of evacuees and residents, further examination will be required to ensure better preparedness in response to a future disaster. This includes the sharing of information among various teams, overall coordination of functions on the ground, and information-sharing and liaison with a central command. Furthermore, most of the disaster–designated hospitals in Iwate Prefecture had a three-day stockpile of medicines, foods and fuel for their own generators. Advance agreements to have prioritized procurement with suppliers are important to prepare for long-term interruption of basic services.
The psychological and physical burdens of living for a long period of time as evacuees were extremely large. As of September 2011, there had not been a reported rise in the number of severe conditions such as stroke or heart failure, but these aspects will require careful monitoring in the future.
There were no large-scale epidemics of infectious diseases in the evacuation centres. The enhanced knowledge and awareness of public health and medical practitioners is thought to have contributed to this outcome. Ad hoc surveillance (daily surveillance for outbreak detection) was helpful to monitor infectious disease status in large-scale evaluation centres.
The lessons from previous disasters such as the great Hanshin-Awaji and the Niigata-Chuetsu earthquakes tell us that the psychological impact of the disaster will require careful, attentive and systematic assistance over the long term.9–12 In addition, it will be essential to provide sustained assistance to bereaved children and orphans on whom the psychological impact will be especially great, as well as on-the-ground medical activities and technical advice to local support staff. These include health care workers, local government officials, fire and police service personnel and teachers who were, despite engaging in assistance activities, disaster victims themselves.
By referring to past experiences of national and international large-scale disasters,13 there was an effective response to several health-related challenges pertaining to medical and public health and sanitation. However, there were many issues that exceeded initial expectations or scenarios for a large-scale disaster, and a specific response needs to be made to tsunami disasters. There are many outstanding challenges that cannot be resolved by resorting to a response based on a disaster manual.
Furthermore, it is a fact that the health and welfare systems of each country are different. There are various laws and health insurance plans relating to medical qualifications and systems that vary from country to country. There are cases in which a response made in one country may not be applicable in another. Therefore, a response is required that is based on the particular systems and local characteristics of the country in question.
Six months after the disaster, the evacuation centres were closed, the acute phase of the disaster response ended and the full-fledged recovery and restoration of the public health system, including maternal care or immunization activities for children, was re-started. Public health systems are essential for overall recovery as they form a safety net for residents. However, such systems cannot stand alone in society, as they are all closely related to other factors, including industry and employment, the living environment, social capital and administrative systems. This interdependence is also something that will require action in the long term to achieve cooperation among the various sectors of society.
None declared.
None.
I would like to take this opportunity to mention the tremendous and diverse assistance Japan received from around the world following the disaster. This assistance has been a great help in reconstruction efforts by residents in the disaster-affected areas and the knowledge that the world was providing such support was also a great comfort. I would like to offer my heartfelt appreciation.
{kind=link}
{kind=link}