a Emerging Disease Surveillance and Response, Division of Health Security and Emergencies, World Health Organization Regional Office for the Western Pacific, Manila, Philippines.
Correspondence to Yuzo Arima (e-mail: arimay@wpro.who.int).
To cite this article:
Arima Y et al. The Great East Japan Earthquake: a need to plan for post-disaster surveillance in developed countries. Western Pacific Surveillance and Response Journal, 2011, 2(4):3-6. doi:10.5365/wpsar.2011.2.4.007
After a devastating earthquake and tsunami struck north-eastern Japan in March 2011, the public health system, including the infectious disease surveillance system, was severely compromised. While models for post-disaster surveillance exist, they focus predominantly on developing countries during the early recovery phase. Such models do not necessarily apply to developed countries, which differ considerably in their baseline surveillance systems. Furthermore, there is a need to consider the process by which a surveillance system recovers post-disaster. The event in Japan has highlighted a need to address these concerns surrounding post-disaster surveillance in developed countries.
In May 2011, the World Health Organization convened a meeting where post-disaster surveillance was discussed by experts and public health practitioners. In this paper, we describe a post-disaster surveillance approach that was discussed at the meeting, based on what had actually occurred and what may have been, or would be, ideal. Briefly, we describe the evolution of a surveillance system as it returns to the pre-existing system, starting from an event-based approach during the emergency relief phase, a syndromic approach during the early recovery phase, an enhanced sentinel approach during the late recovery phase and a return to baseline during the development phase. Our aim is not to recommend a specific model but to encourage other developed countries to initiate their own discussions on post-disaster surveillance and develop plans according to their needs and capacities. As natural disasters will continue to occur, we hope that developing such plans during the “inter-disaster” period will help mitigate the surveillance challenges that will arise post-disaster.
After the devastating magnitude 9.0 Great East Japan Earthquake and tsunami struck north-eastern Japan on 11 March 2011, the public health system was severely compromised in the affected areas. The destruction caused by the event was unprecedented since the Second World War; in addition to causing nearly 16 000 deaths with more than 3500 still missing,1 the event destroyed the medical and public health buildings and the telecommunication systems vital to the public health system. The public health workforce was also severely affected; many public health workers were victims of the disaster, and those who could work did so under extremely difficult conditions. While no large infectious disease outbreaks occurred, systematic collection, collation, interpretation and reporting of infectious disease data faced numerous challenges, making needs and risk assessments difficult.
In May 2011, the World Health Organization (WHO) meeting, “Informal meeting on disaster recovery for the health sector,” was held at the WHO Kobe Centre in Japan, where post-disaster recovery of public health services, including infectious disease surveillance systems, was discussed by a group of experts and public health practitioners from affected areas. The approach described in this article is based on those preliminary discussions, which emerged from both observations and initial assessments from the field in addition to input from public health infectious disease surveillance experts. The authors hope that public health practitioners in other developed countries will find this information useful to initiate their own discussions and review or plan their post-disaster surveillance systems to better prepare in case a major disaster occurs.
The existing infectious disease surveillance system in Japan is similar to those in many other developed countries, with components of laboratory confirmations and reporting based on both notifiable disease and sentinel surveillance.2 Despite the occurrence of periodic natural disasters including earthquakes and tsunamis, the Japanese system lacked a comprehensive post-disaster surveillance plan. Furthermore, while there are existing models, frameworks and discussions of post disaster surveillance,3–8 many focus on the developing country setting, and such models do not necessarily apply to developed countries. Developed countries differ considerably from developing countries in their baseline surveillance system, including the medical and laboratory facilities and the telecommunication services that support them.
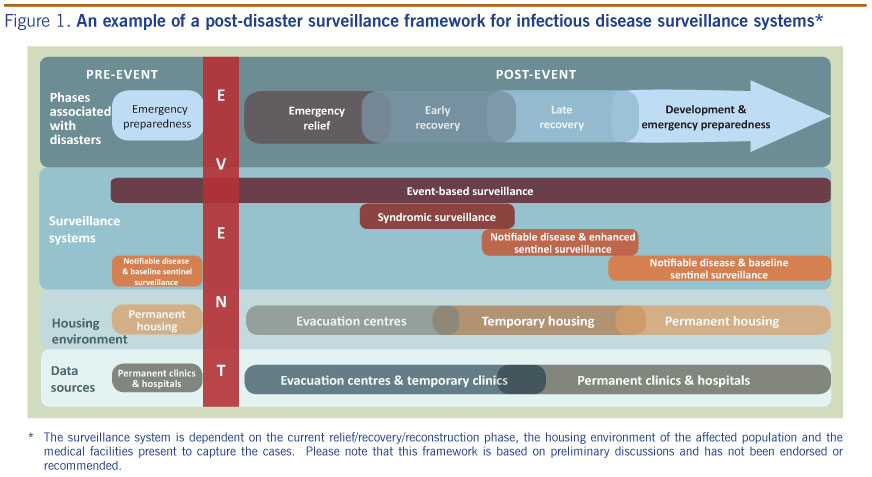
As in other major natural disasters, soon after the Great East Japan Earthquake, emergency relief focused on medical care for rescued survivors and implemented acute public health measures, such as sanitation and hygiene, to reduce occurrences of infectious diseases. During this period, there was very limited communication and coordination capacity, making systematic information collection difficult. Given that situation, event-based surveillance (EBS) (organized and rapid capture of information about events that are a potential risk to public health9) was used at many of the shelter sites by first responders and others working on site (Figure 1). Events, as clusters of syndromes, could be rapidly detected and reported through ad hoc telecommunication systems (e.g. radio). EBS was believed to be the most efficient and effective way to collect and act on the information during the emergency response phase due to its practical and informal method.
* The surveillance system is dependent on the current relief/recovery/reconstruction phase, the housing environment of the affected population and the medical facilities present to capture the cases. Please note that this framework is based on preliminary discussions and has not been endorsed or recommended.
During the early recovery phase of the Great East Japan Earthquake, workforce capacity, physical infrastructure and telecommunication infrastructure improved; frequent and routine (e.g. daily reporting) syndromic surveillance began to supplement ongoing EBS at the evacuation shelters where the majority of the displaced persons resided and at the temporary health clinics that were established. Such an intermediate step may be more feasible than attempting to return fully to the pre-existing, baseline indicator-based surveillance system (e.g. routine reporting of notifiable diseases, sentinel surveillance, and laboratory-based surveillance9), as a syndromic approach is less dependent on sophisticated medical and laboratory needs which may still be limited in capacity.
During the late recovery phase, when the displaced population has relocated to temporary or semi permanent residences, the concept of an “enhanced” sentinel surveillance system was discussed for diseases or syndromes that are usually followed through sentinel surveillance (e.g. influenza-like illness), with routine but less frequent (e.g. weekly) reporting. With mass gathering conditions no longer present (e.g. high population density, challenges in sanitation/hygiene, poor nutrition, higher stress levels), the risk of infectious disease outbreaks would decline, making reporting on a more routine basis from all sites unnecessary. In addition, with the further recovery of medical, public health and laboratory capacities, implementing a system that existed pre-event would be possible. However, an “enhanced” system with proportionately more sentinel sites than normal from the catchment area/population may be useful given the vulnerability of the displaced and the altered geographic locations and demographics of the populations. In addition, with likely continued migration of persons over time, it is important to monitor trends in infectious diseases in an enhanced manner before returning completely to the baseline sentinel system. Lastly, at the development phase, when the displaced have moved to permanent homes and permanent clinics and hospitals have been re-established, surveillance can return to the baseline system.
The progression of the surveillance system described here, based on both actual occurrences and proposed ideas, can be viewed as the evolution of a surveillance system as it matures after a disaster event. Throughout this process, participants at the WHO meeting noted that surveillance professionals who are familiar with interpretation of surveillance data should be closely involved. As the surveillance system recovers, it was also emphasized that the post-disaster system should function within the existing surveillance system to the extent possible, so as not to become a competing ad hoc system that duplicates or burdens the baseline system. While baseline surveillance systems may be limited in scope and capacity in developing countries and the implementation of a post-disaster system may not greatly burden or conflict with the pre-existing systems, comprehensive surveillance systems often already exist in developed countries.
As different surveillance systems have their advantages and disadvantages and as surveillance systems are designed to meet particular needs at particular moments (e.g. differing priorities of sensitivity, specificity and timeliness), the meeting participants emphasized flexibility with consideration of the following:
Comprehensive risk assessment would assist in making decisions by taking these points into account. Thus, when planning for post-disaster surveillance systems, public health practitioners in developed countries should carefully balance the need to work within the existing system, adjusting the system to the current needs and capacities. As natural disasters will continue to occur, we hope that planning for post disaster surveillance during the “inter-disaster” period will help mitigate the numerous surveillance difficulties that would be faced in times of such occurrences.
None declared.
None.
The authors wish to thank all those who were instrumental in making the meeting on disaster recovery for the health sector in May 2011 and the two WHO missions to the affected sites in northern Japan possible. The authors would also like to thank the Japanese Ministry of Health, Labour and Welfare who welcomed the WHO missions, in addition to National Institute of Infectious Diseases who provided important background information of the situation. In particular, we would like to thank Dr Kiyosu Taniguchi and colleagues at the National Institute of Infectious Diseases for the in-depth discussions on post-disaster surveillance. Dr Hiroyuki Kunishima and other faculty members at Tohoku University and Iwate Medical University also need to be thanked for their logistical assistance and invaluable accounts from the field. Dr Masaru Nohara from the Iwate Prefectural government also made important contributions to this topic. Lastly, we would like to greatly acknowledge all the front-line workers in the field, who worked tirelessly for long hours with little rest.
{kind=link}