a Emerging Diseases Surveillance and Response, Division of Health Security and Emergencies, World Health Organization Regional Office for the Western Pacific, Manila, Philippines
Correspondence to Yuzo Arima (e-mail: arimay@wpro.who.int).
To cite this article:
Arima Y and Matsui T. Epidemiologic update on the dengue situation in the Western Pacific Region, 2010. Western Pacific Surveillance and Response Journal, 2011, 2(2):4-8. doi:10.5365/wpsar.2011.2.2.005
Dengue is an emerging vectorborne infectious disease that is a major public health concern in the Asia Pacific region. Official dengue surveillance data for 2010 provided by the ministries of health were summarized as part of routine activities of the World Health Organization Regional Office for the Western Pacific. Based on reported data, dengue has continued to show an increasing trend in the Western Pacific Region. In 2010, countries and areas reported a total of 353 907 dengue cases, of which 1073 died, for a case fatality ratio of 0.30%. More than 1000 cases were reported each from Australia (North Queensland), Cambodia, the Lao People's Democratic Republic, Malaysia, the Philippines, Singapore and Viet Nam. All of these countries, except for Australia where the dengue virus is not endemic, reported an increase in the number of reported cases in 2010 compared to 2009. The elevated number of cases reported in 2010 in some countries, such as the Philippines, is likely due to several factors, such as enhanced reporting and continued epidemic activity. However, increases in reported number of cases in other areas, such as Singapore and Malaysia, appear to indicate sustained epidemic activity in those countries. The continued epidemic dengue activity in the Region highlights the need for timely and routine regional sharing of information.
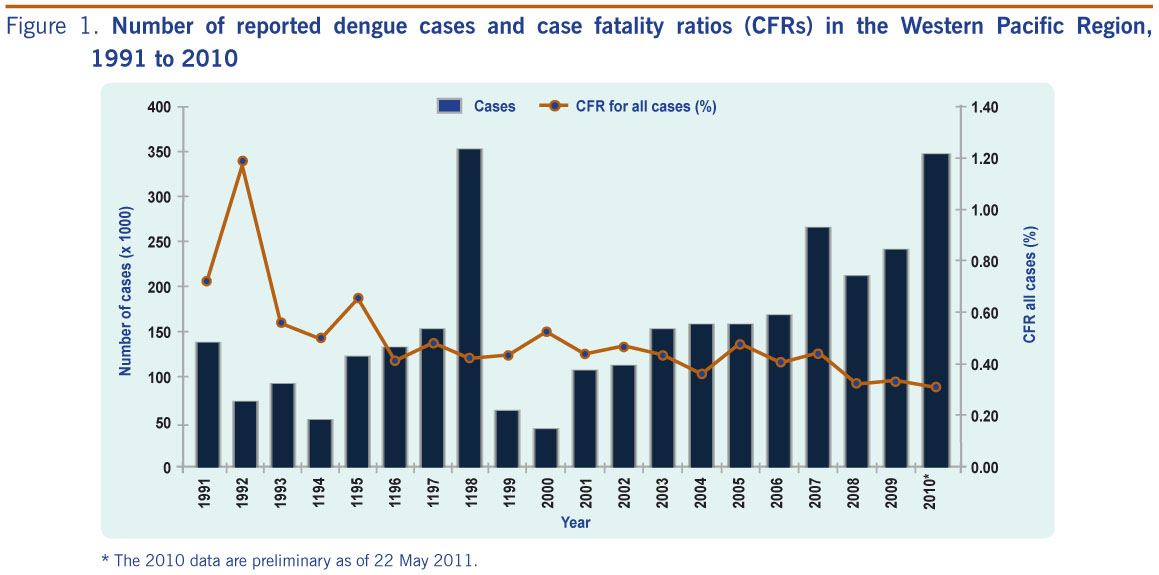
Dengue is the fastest emerging arbovirus infection in the Asia Pacific region, with a high burden of this disease also borne by countries in this region. Multi-year oscillations in disease occurrence have been observed, reflecting dengue's dynamic and complex epidemiology.1,2 Although the number of reported cases dropped to around 50 000 annually in 1999 and 2000 after the large epidemic in 1998, dengue has again increased in overall activity over the past decade. During the period 2003–2006, the number of reported cases increased to 150 000–170 000 per year, and since 2007, the region has consistently reported over 200 000 cases annually (Figure 1).
* The 2010 data are preliminary as of 22 May 2011.
In 2009, there were 242 424 dengue cases and 785 dengue deaths reported in 25 out of 37 countries and areas in the Western Pacific Region. Countries that reported more than 1000 cases were: Australia (North Queensland), Cambodia, French Polynesia, the Lao People's Democratic Republic, Malaysia, New Caledonia, the Philippines, Singapore and Viet Nam. Cambodia, the Lao People's Democratic Republic, Malaysia, the Philippines, Singapore and Viet Nam contributed 781 of the 785 deaths. While surveillance is limited in the Pacific islands, dengue activity has been occurring, as evidenced by data from the French territories of New Caledonia and French Polynesia. In 2009, 14 Pacific Island countries and areas reported dengue outbreaks, and five reported high dengue incidence: American Samoa (644/100 000 population), Cook Islands (1090/100 000 population), French Polynesia (922/100 000 population), New Caledonia (3443/100 000 population) and Tonga (263/100 000 population). While dengue surveillance is not conducted in Papua New Guinea, circulation of dengue virus there is well known given the importation of cases into Australia.3,4
Through this epidemiologic update, the World Health Organization (WHO) Regional Office for the Western Pacific aims to inform the latest regional dengue situation. This report is the first of its kind and the goal is to continue such communication on a routine basis and encourage countries and areas in the Western Pacific Region to maintain their surveillance and reporting activities.
This report provides a descriptive summary of the regional dengue situation for 2010 based on data derived from indicator-based surveillance systems in the Region. Particular focus is given to dengue-endemic countries where dengue surveillance systems exist (i.e. Cambodia, the Lao People's Democratic Republic, Malaysia, the Philippines, Singapore and Viet Nam); Australia is also included as periodic dengue outbreaks occur in North Queensland. WHO Regional Office for the Western Pacific, with the assistance of WHO country offices, obtains these data on a biweekly basis from ministries of health, and collection of such information, along with periodic risk assessment, are routine activities of Regional Office. The timeliness of reporting and completeness of reporting sites and surveillance data vary by country, and the latest information available is presented. The Regional Office also feeds back these data to countries and areas on a biweekly basis through http://www.wpro.who.int/health_topics/dengue.
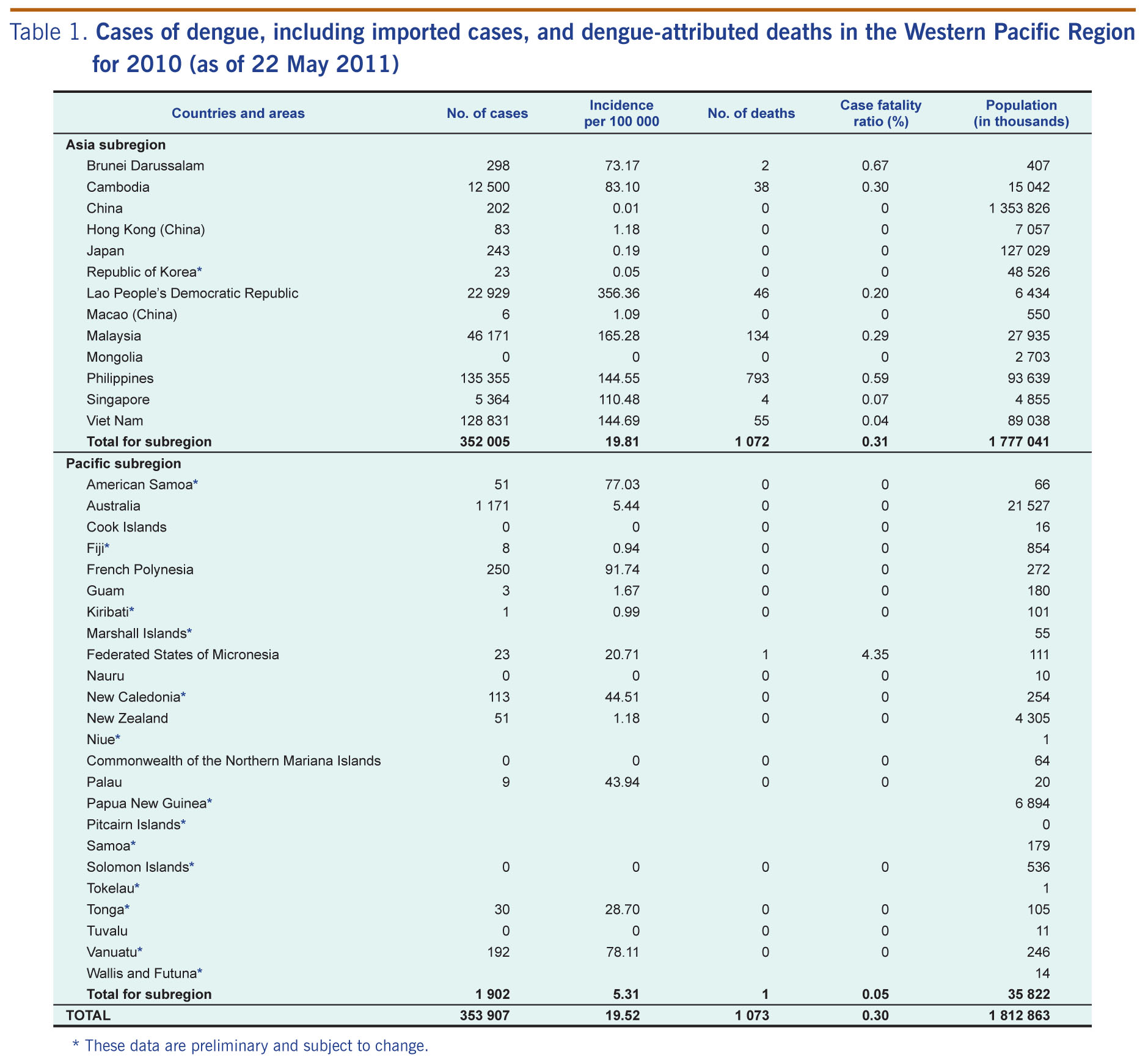
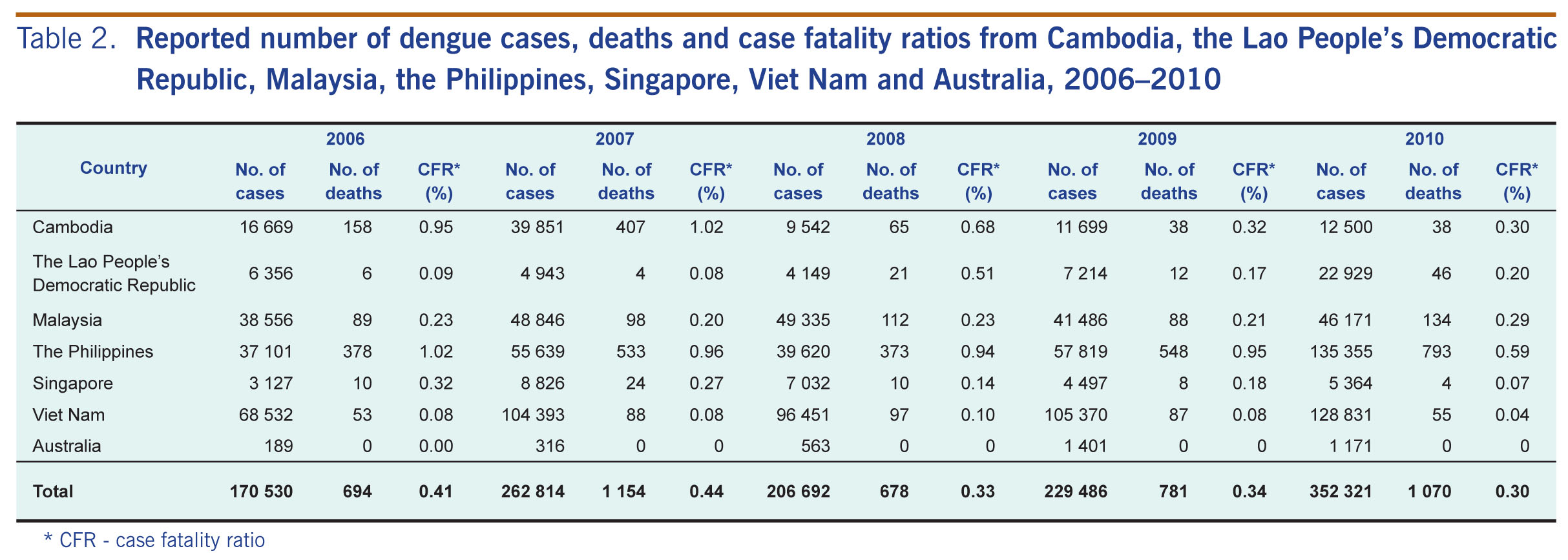
In 2010, Western Pacific Region countries and areas reported a total of 353 907 cases, of which 1073 people died, for a case fatality ratio (CFR) of 0.30%. While incidence of dengue was greatest in the Lao People's Democratic Republic, the total numbers of cases and deaths reported were greatest for the Philippines (Table 1). Summarization and reporting of the 2010 dengue data from the Pacific subregion are ongoing, but more than 100 cases were reported each from French Polynesia, New Caledonia and Vanuatu (Table 1). While dengue is not endemic in New Zealand, 51 cases were reported in 2010; all cases had overseas exposures with 12% of cases associated with travel to Vanuatu. Detailed information for countries with more than 1000 reported cases (Australia [North Queensland], Cambodia, the Lao People's Democratic Republic, Malaysia, the Philippines, Singapore and Viet Nam) is presented below. With the exception of Australia, the number of reported cases in 2010 was greater than that reported in 2009 for these countries (Table 2).
* These data are preliminary and subject to change.

* CFR - case fatality ratio
Under the National Dengue Control Programme, suspected or probable dengue cases are reported through seven sentinel sites and other non-sentinel sites. In 2010, Cambodia reported 12 500 cases (38 fatal), with a peak (n = 835 cases) during week 31 in August. While all four serotypes circulated, the predominant serotypes identified were DEN-1 and DEN-2.
In the Lao People's Democratic Republic suspected or probable dengue cases are reported through the National Surveillance System for Selected Notifiable Diseases and Early Warning and Response Network. In 2010, the Lao People's Democratic Republic reported 22 929 cases (46 fatal), with a peak (n = 1323 cases) during week 33 in August. While all four serotypes circulated, the predominant serotype identified was DEN-1, followed by DEN-2 and DEN-3.
Suspected or probable dengue cases are reported through the National Notifiable Infectious Diseases system. In 2010, Malaysia reported 46 171 cases (134 fatal). While the number of cases fluctuated throughout the year, the greatest number of cases (n = 1 159) was reported during week 34 in August. While all four serotypes circulated, the predominant serotype identified was DEN-1, followed by DEN-3 and DEN-2.
Suspected or probable dengue cases are reported through the Philippines Integrated Disease Surveillance and Response (PIDSR) system. In 2010, the Philippines reported 135 355 cases (793 fatal), with a peak (n = 30 009) during the month of August. While all four serotypes circulated, the predominant serotype identified was DEN-3.
Dengue cases are laboratory-confirmed and reported through the Infectious Diseases Management and Outbreak System. During 2010, Singapore reported 5364 cases (4 fatal), with a peak (n = 182) during week 38 in September.
Suspected or probable dengue cases are reported through the National Notifiable Disease Surveillance system. In 2010, Viet Nam reported 128 831 cases (55 fatal). While all four serotypes circulated, the predominant serotypes identified were DEN-1 and DEN-2.
Dengue cases are laboratory-confirmed and reported through the National Notifiable Diseases Surveillance System. In 2010, Australia reported 1171 cases (none fatal), with a peak (n = 139) during the month of November. Dengue activity in Australia is restricted to North Queensland where the vector Aedes aegypti is present (the dengue virus itself is not endemic). The predominant serotypes identified from outbreaks in North Queensland were DEN-1 and DEN-2, although all four serotypes have been isolated from imported viraemic cases.
In 2010, dengue continued to show an increasing trend in the Western Pacific Region as observed in the past decade. The countries with the greatest dengue burden in the Asia subregion, namely the dengue endemic countries of Cambodia, the Lao People's Democratic Republic, Malaysia, the Philippines, Singapore and Viet Nam, showed an increase in reported number of cases, ranging from 1.1-fold (Malaysia) to 3.2-fold (the Lao People's Democratic Republic) the number of cases reported in 2009 (Table 1). Importantly, the Lao People's Democratic Republic also reported an increase in CFR relative to 2009 (Table 1). For Cambodia, the Lao People's Democratic Republic, the Philippines and Singapore peaks in dengue activity followed historic seasonal trends, with peaks occurring shortly after onset of the rainy season during and around the month of August. The increase in the Aedes aegypti habitat is believed to increase overall prevalence of disease in the environment and raise the risk of its spread.5 From the Pacific subregion, French Polynesia, New Caledonia, Vanuatu and Australia contributed 91% of reported cases, with Australia (North Queensland) reporting more than 1000 laboratory-confirmed cases for two consecutive years.
Sharing of regional surveillance data plays an important role in dengue control. While vector control activities at the local level are essential to interrupt dengue transmission, routine and timely information-sharing of regional data helps to improve countries and areas' understanding of the overall dengue situation, including dengue epidemiology in neighbouring countries or other countries of interest with close trade/travel links. Indeed, dengue does not acknowledge national borders, and in the Pacific islands, dengue activity has been associated with introductions from various locations in Asia.6,7 Comprehensive regional information provides better-informed risk assessments by each country that directly lead to response activities, such as preparation for enhanced education and awareness activities. Regional surveillance data showing continued high level dengue activity have also contributed to the recent launch of the Association of Southeast Asian Nations Dengue Day on 15 June 2011, which aimed at improving advocacy and community participation. Sharing additional surveillance data, such as serotypes and affected age group data, can further improve risk assessments since monitoring these data may reveal important changes or features in dengue epidemiology.8
As with any surveillance data, these data have important limitations attributable to changes in reporting behaviour, surveillance systems, misclassifications and underreporting. For example, a proportion of the excess cases in the Philippines in 2010 (135 355 in 2010 versus 57 819 in 2009) is a result of an ongoing change in the surveillance system. Since 2008, the surveillance system has been transitioning from a sentinel (National Epidemic Sentinel Surveillance System) to an all-case reporting system (PIDSR). The extent of this transition has been variable, with some areas starting the transition earlier than others (personal communication, the Philippines Department of Health). In addition, as dengue surveillance in Cambodia, the Lao People's Democratic Republic, Malaysia, the Philippines and Viet Nam is based on suspected or probable cases that are not all laboratory-confirmed, the number of reported cases should be interpreted with caution. Moreover, systematic and representative sampling for laboratory confirmation in some of these countries has been challenging, limiting interpretability of reported serotype data. As dengue surveillance across endemic countries differ and are not standardized, any comparison between countries should also be interpreted with caution. For example, CFRs are affected not only by clinical management but also by case-reporting systems and reporting behaviours of clinicians.
While direct comparisons between countries cannot be made, these data are important for assessing trends both within and across years. The data from 2010 indicate that for the majority of endemic countries, dengue activity followed historic seasonality. In addition, the increase in the yearly trend of reported cases in Singapore and Malaysia appeared to indicate a true increase for 2010 in these countries. As cases are reported from consistent surveillance systems and case definitions, any misclassifications of cases likely remain constant. To make dengue surveillance useful for timely and effective public health response, trend assessments will continue to be essential both at national and regional levels.
The ongoing dengue burden in the Western Pacific Region underscores the continuing need for region-wide sharing of information on a timely and routine basis. Countries and areas should continue to maintain their surveillance activities and, where they are lacking or deficient, enhance or implement dengue surveillance systems. Enhancement or implementation of dengue surveillance could also act as a model system for countries where surveillance capacities are limited for endemic infectious diseases; such activities are in line with the biregional Asia Pacific Strategy for Emerging Diseases framework to strengthen national capacities for surveillance and response. Even in countries where dengue is not endemic (e.g. Australia and Japan), the ever-increasing importation of cases3,9,10 signifies the importance of monitoring and reporting of dengue for all countries and areas in the Region. Lastly, to improve preparedness and response activities in the face of the ever-evolving epidemiology of dengue, there is a need for more systematic surveillance and reporting of serotype and age- and sex-stratified data.
None declared.
This study was undertaken as part of routine surveillance activities of the WHO Regional Office for the Western Pacific.
The authors would like to thank all the WHO Western Pacific Regional Country Office staff for assisting with surveillance data collection and reporting.
{kind=link}
{kind=link}
{kind=link}