a Department of Virology, Tohoku University Graduate School of Medicine, Sendai, Japan (e-mail: oshitani@med.tohoku.ac.jp).
To cite this article:
Oshitani H. Influenza surveillance and control in the Western Pacific Region. Western Pacific Surveillance and Response Journal. 2010, 1(1):3-4. doi:10.5365/wpsar.2010.1.1.005
Influenza is one of the most common acute viral infections in humans. It is estimated that seasonal epidemics affect 10–20% of the population, resulting in 250,000 to 500,000 deaths every year.1 In addition to seasonal influenza epidemics, antigenically distinct viruses originating from animal species tend to emerge in the human population every 10 to 40 years. Since most the human population does not have immunity to such viruses, global epidemics with significant impact, i.e. influenza pandemics, have occurred in the past.
Countries and areas in the Western Pacific Region are very diverse in terms of population size, climate, and social and cultural characteristics. Due to such diversity, the Region has special issues, challenges and global importance in influenza surveillance and control. In particular, the Region is known as a ‘hotspot’ for influenza as East and South-East Asia are considered to be a source of new antigenic variants.2
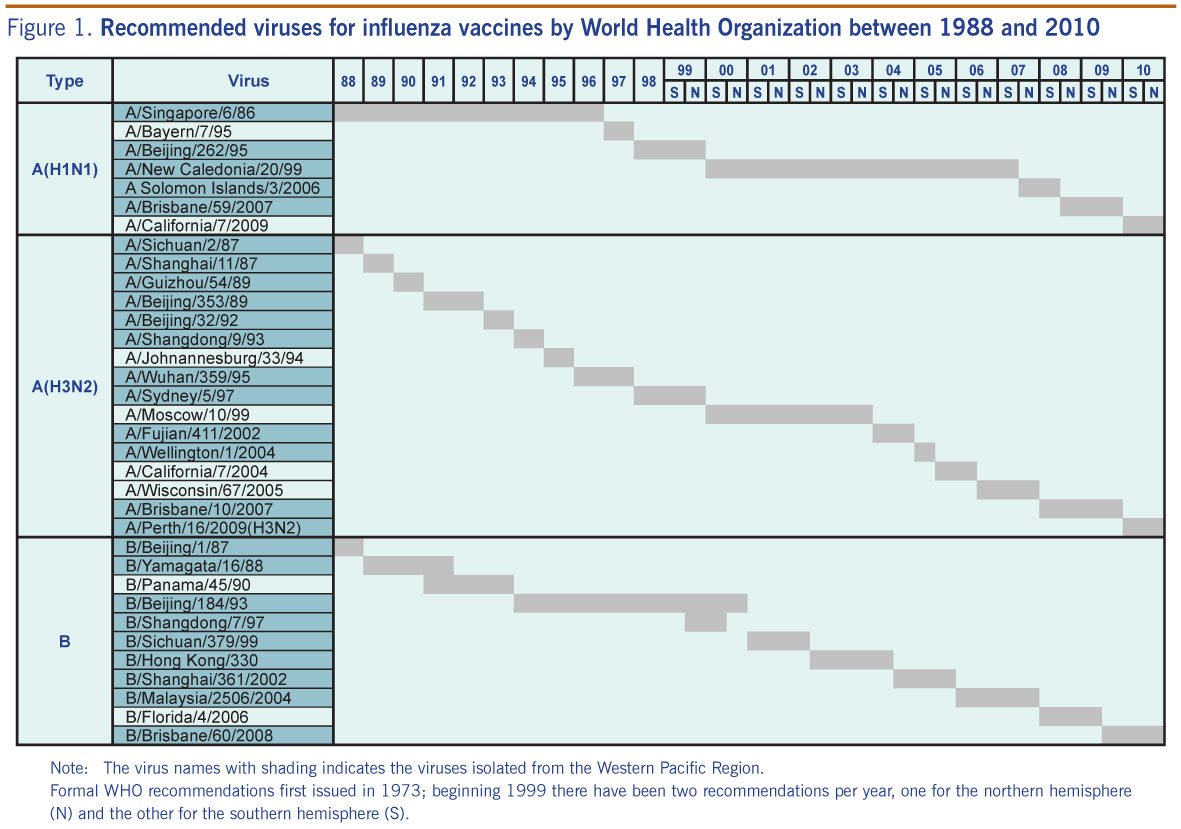
Because seasonal influenza viruses are constantly changing, vaccine strains should be updated to ensure the closest possible match with circulating strains. The World Health Organization (WHO) has made recommendations on vaccine strains annually since 1972 and twice a year since 1999 (in February for the northern hemisphere and in September for the southern hemisphere).3 Many viruses isolated in the Region have been recommended as vaccine strains by WHO. A total of 34 different viruses have been recommended for vaccine strains by WHO between 1988 and 2010, and 26 out of 34 (76.4%) were isolates from the Region (Figure 1)
The Region is also considered to be a potential source for pandemic influenza. At least two past pandemics, Asian Flu in 1957 and Hong Kong Flu in 1968, are believed to have been originated from the Region.4 Therefore, influenza surveillance in the Region is critical in monitoring antigenic changes of seasonal influenza and detecting viruses with pandemic potential.
Despite regional and global importance, influenza surveillance in the Region was fragmented until recently. In developing countries, there are many competing priorities such as HIV/AIDS, tuberculosis, and malaria. Financial support from international organizations tends to be diverted to these other priority diseases.
Another important factor for low resource allocation for influenza is lack of disease burden data for influenza in the Region, especially in tropical developing countries. Epidemiological methods to estimate the mortality impact due to influenza have been established for countries with temperate climates, where the influenza season is clearly observed in winter or early spring. Estimating disease burden in the tropics and subtropics is more challenging because there is no clear seasonality of influenza; therefore, methods developed for temperate climates are difficult to apply. Recent studies conducted in Hong Kong (China) and Singapore indicated that influenza has a high disease burden in tropical and subtropical climates.5,6 However, the disease burden in less developed countries in tropical and subtropical climates is still largely unknown due to a lack of data.
Influenza became a major public health agenda in most countries and areas in the Region, mainly because of the threat posed by highly pathogenic avian influenza A(H5N1). Human infections of H5N1 were confirmed in Hong Kong (China) for the first time in 1997. Since late 2003, there has been widespread transmission of H5N1 among poultry, starting in Asia and later spreading into other regions including Europe, the Middle East and Africa. This virus is highly pathogenic in chickens, but it also causes very severe infections in humans. Nearly 60% of confirmed human cases have died.7 If this virus acquires transmissibility among humans and becomes a pandemic virus, it may have devastating health and social impacts.
Due to the global, regional and national concern about H5N1, influenza has become a major public health issue in the Region. With government commitment and international support, the influenza programmes in many countries have made remarkable progress in the past decade. The quantity and quality of virological testing in National Influenza Centers (NICs) have been improved. Most countries have also developed their national pandemic preparedness plans.
In 2009, the world experienced the first influenza pandemic since 1968. It was caused by influenza A(H1N1) that originated from a swine virus. While it was not as severe as anticipated, the pandemic revealed that there are still many issues and challenges in influenza surveillance and control in the Region. The data generated by influenza surveillance in different countries were difficult to compare because surveillance systems varied between countries. Many NICs were completely overwhelmed by the rapid increase in the number of specimens for testing. Vaccines were either not available or in severe shortage during the epidemic peak in most countries. The supply of antiviral drugs was also not enough, especially in developing countries. These shortfalls revealed the need for strengthened capacity in surveillance and control for both seasonal and pandemic influenza in the Region.
It is necessary to standardize regional and global reporting for seasonal and pandemic influenza. More epidemiological data are required to improve control programmes for seasonal influenza, including increasing the use of seasonal influenza vaccines. Surveillance in each country and throughout the Region also needs to be further strengthened to achieve the ultimate goal of better control and prevention of seasonal and pandemic influenza.
{kind=link}