Nick Morrison
Abstract Although surgical treatment of saphenous vein incompetence is still the most adopted approach worldwide, endovenous thermal ablation of superficial truncal veins is firmly established in the armamentarium of phlebologists in some countries for the ablation of saphenous and non-saphenous veins. Reported results are equal to or better than surgical treatment in terms of postoperative pain and return to full activities. 1 One of the technical challenges of the thermal ablation procedure is the instillation of tumescent anesthesia into the saphenous sheath under ultrasound guidance. This promotes patient comfort allowing the procedure to be carried out in an ambulatory setting. Ultrasound guided tumescent anesthesia is arguably the most difficult hurdle for operators who are new to the procedure. It also represents the most painful part of thermal ablation for the patient. While there is no high-level scientific evidence to support the use of compression following thermal ablation, in practice, nearly everyone utilizes some form of compression for up to several weeks following the procedure because anecdotal evidence suggests that patients are significantly more comfortable and enjoy better postoperative recovery. |
Tumescent anesthesia instillation under ultrasound guidance is challenging and postprocedural compression is considered to be a standard requirement. Given this, even less invasive techniques for venous ablation are being developed. Among these is the instillation of cyanoacrylate glue (CAG) into the target vein. Cyanoacrylate glue has been used effectively as a tissue adhesive, a vascular closure agent, and as an intracranial embolic agent for arteriovascular malformations. Cyanoacrylates are synthetic glues that rapidly polymerize on contact with water or blood. N-butyl-2-cyanoacrylate (Histoacryl; B Braun, Melsungen, Germany) has been used extensively in surgery for a decade. Another N-butyl-2-cyanoacrylate (Glubran, GEM Srl., Viareggio, Italy) was recently approved for endoscopic use in Europe. 2-octyl-cyanoacrylate (Dermabond, Ethicon, Inc., Somerville, NJ, USA), approved by the Federal Drug Administration for superficial wound closure, is widely used in the US, particularly by emergency room physicians, dermatologists and surgeons. Substances such as plasma, blood or saline stimulate polymerization of the adhesive upon contact, leading to occlusion of the vessel. The resultant polymerization damages the vascular intima and induces an immunological response. After polymerization is complete, gradual resorption of the occlusive polymer takes place. Within approximately one month, the response progresses to a granulomatous process with foreign body giant cells and eventual fibrosis.
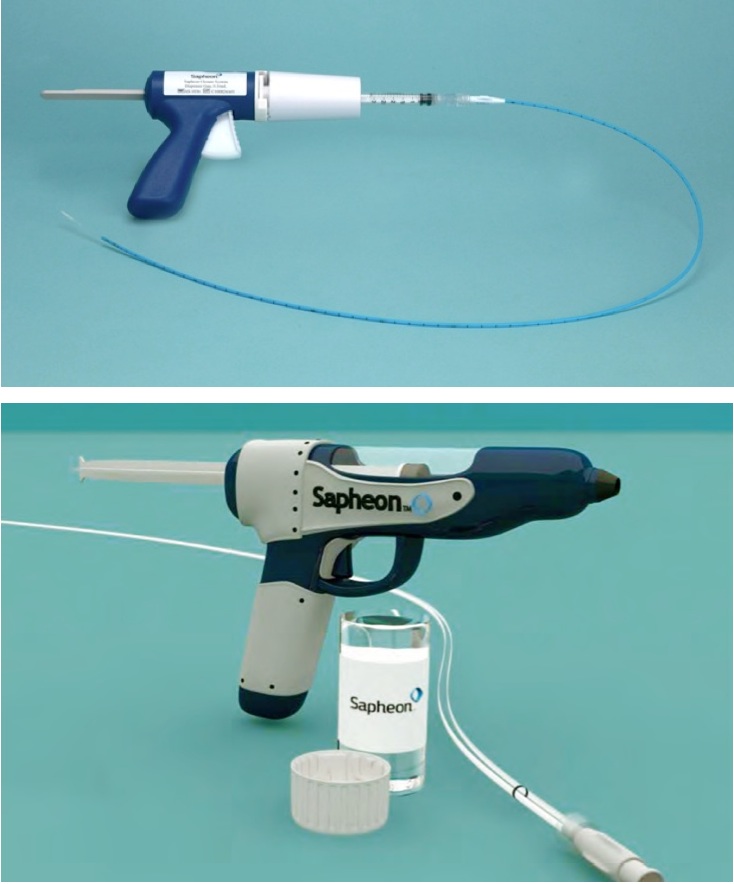
Sapheon Inc. (Santa Rosa, California, USA) has developed a proprietary cyanoacrylate adhesive (SCA) for permanent closure of incompetent superficial leg veins in an attempt to eliminate the need for the tumescent anesthesia and postoperative compression used in thermal and surgical ablation procedures. Following successful vein occlusion in animal models, 2 the first human study was carried out by an American group (Almeida et al. 3). This product received CE approval for use in Europe in September 2011. However, since it has not been approved by the US FDA for saphenous vein ablation, the studies 4 were conducted outside the US on 38 patients treated with SCA of the great saphenous vein (GSV) under only local catheter insertion site anesthesia and without the use of tumescent anesthesia or postoperative compression. The mean maximum GSV diameter was 8 mm and 17 of 38 patients were CEAP class 4 or above. The catheter was positioned approximately 4 cm below the saphenofemoral junction (SFJ). This was manually compressed and the SCA was injected. Compression was maintained for 3 min. The adhesive was delivered at 3 cm intervals for the remainder of the treated vein using 30 s of compression for each subsequent delivery (Figure 1).
|
Figure 1. Sapheon Inc. (Santa Rosa, California, USA) has developed a proprietary cyanoacrylate adhesive for permanent closure of incompetent superficial leg veins. |
The mean length of ablated GSV segments was 33 cm (range 15-52) and the average treatment duration was 20.3 min (range 11-33). The mean volume of SCA delivered was a total of 1.3 mL (range 0.63-2.25). Thirty-six of 38 (95%) patients were followed for 30 days, including clinical (VCSS scores) and duplex evaluations. The procedure was well tolerated by all patients who required no postoperative analgesics (6 of 37 received NSAIDs). Duplex examination documented complete occlusion of the GSV in 35 of 38 patients (92%) with one complete recanalization and 2 partial mid-thigh recanalizations. Clinical VCSS scores decreased dramatically within 24 h and continued to improve over the follow-up period (mean 6.0-1.9 at 30 days).
The problem of post ablation thrombus extension (PASTE) through the SFJ, an infrequent event after thermal or foam saphenous ablation, was seen in 8 of 38 (21%) patients in the study. However, in a preliminary report 5 of a study of 20 patients (eSCOPE study in Germany, Denmark and the UK) this problem appears to have been resolved by moving the first injection to 5 cms below the SFJ, as reported by Proebstle et al. 5
In conclusion, several innovative methods for saphenous ablation have been developed and are currently undergoing clinical tests. The use of cyanoacrylate glue appears to hold some promise in reducing the two main challenges related to thermal ablation for physicians and patients alike: the need for ultrasound guided tumescent anesthesia and postoperative compression.
References
1. Rasmussen LH, Lawaetz M, Bjoern L, et al. Randomized clinical trial comparing endovenous laser ablation, radiofrequency ablation, foam sclerotherapy and surgical stripping for great saphenous varicose veins. Br J Surg 2011;98:1079-87.[CrossRef][PubMed][TOP]