|
|
|
Free Neuropathology 3:26 (2022) |
|
Review |
|
Neurotrauma: 2022 update |
|
David S. Priemer1-3, Daniel P. Perl1,2 |
|
1 The Department of Defense/Uniformed Services University Brain Tissue Repository, Bethesda, MD, USA |
|
Corresponding author: |
|
Submitted: 24 October 2022 Accepted: 01 November 2022 Copyedited by: Shino Magaki Published: 15 November 2022 |
|
Keywords: Traumatic brain injury, Chronic traumatic encephalopathy, Tau, Interface astroglial scarring, Diffuse axonal injury, Multidimensional MRI |
|
Abstract The year 2021 was highlighted by many notable advancements in the field of neurotrauma and associated neuropathology. After a thorough review of the new literature, we call attention to what we feel are among the most impactful studies and publications. In brief, 2021 was marked by published consensus papers related to the diagnosis of chronic traumatic encephalopathy (CTE) and its clinical counterpart, traumatic encephalopathy syndrome. There was also progress toward our understanding of the impact of traumatic brain injury (TBI) on the general population, and how strongly CTE pathology may, or may not, commonly underlie long term clinical sequelae following TBI. Next, a critical new study has identified that acetylated tau protein, which has been found to be increased in the brains of Alzheimer’s disease and CTE patients, can be induced by TBI, is neurotoxic, and that its reduction via already-existent therapeutics is neuroprotective. There are also several important updates that pertain to military and blast TBI, particularly as they pertain to establishing causality of interface astroglial scarring. In addition, and for the first time, a specific signature for diffuse axonal injury has been identified in ex vivo tissues using multidimensional magnetic resonance imaging, providing promise for the clinical diagnosis of this lesion. Finally, several important radiologic studies from 2021 have highlighted long-standing structural reductions in a number of brain regions following both mild and severe TBI, emphasizing the need for neuropathologic correlation. We end by highlighting an editorial piece discussing how TBI is portrayed in entertainment media and how this impacts public perception of TBI and its consequences. Introduction Through the emergence of new viral variants, and the waxing and waning of health measures taken by both governments and private industry, the COVID-19 pandemic remained an obstacle to ongoing research work related to neurotrauma in the year 2021. However, a review of the published literature in 2021 reveals that interest and advancement has not been slowed, but rather appears to have increased. For example, a simple search for the term ‘traumatic brain injury’ (TBI) on PubMed reveals 5,387 results for the year 2021, which is the most of any year on record. Correspondingly, a number of important papers appeared that are of considerable impact to our neuropathology-oriented readership. Here, we present our admittedly biased list of highlight papers that were published in the year 2021, with commentary on the information they provided and why we chose to include them in this year’s listing. We are quick to note that a few of these papers have involved our own participation; we do not apologize for these choices, as we think others tasked with the judgement of important contributions to the field of neurotrauma would have similarly considered them. Updates to neuropathological criteria for chronic traumatic encephalopathy (CTE) and its proposed clinical syndrome The light that is the study of CTE burned as brightly as ever in 2021, and perhaps is best represented by the publication of the highly awaited conclusions of the Second National Institute of Neurological Disorders and Stroke (NINDS)/ National Institute of Biomedical Imaging and Bioengineering (NIBIB) Consensus Meeting to Define Neuropathological Criteria for CTE.1 Five years in the making, this paper details the results of the reconvening of the NINDS/NIBIB consensus panel in the year 2016 to refine the diagnostic criteria for CTE that were set after the first panel meeting in 2015. Through the evaluation of 27 cases of different tauopathies, the panel of neuropathologists was able to identify and discern CTE according to the original diagnostic criteria, with high rates of agreement while both blinded and unblinded to gross neuropathological findings and clinical histories. Therefore, the panel agreed to largely uphold the original definition of the pathognomonic lesion of CTE, but with some refinement that can be appreciated in the comparison below: Definitions of the pathognomonic lesion for a minimal diagnosis of CTE:
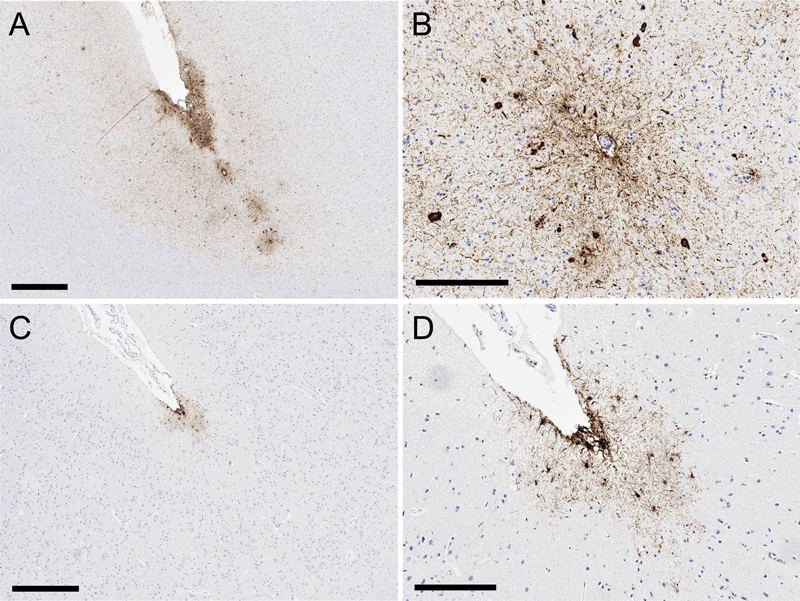
As can be seen, the updated definition for the pathognomonic lesion maintains that a diagnostic CTE lesion must be at a cortical sulcal depth and that it must display perivascular neurofibrillary changes, but now more strongly emphasizes neuronal involvement as necessary, and details that p-tau pathology cannot be limited to the superficial aspects of the cortex. These refinements were made in the hopes that they will lead to more reliable delineation between CTE and other entities, such as age-related tau astrogliopathy (ARTAG) (see Figure 1).
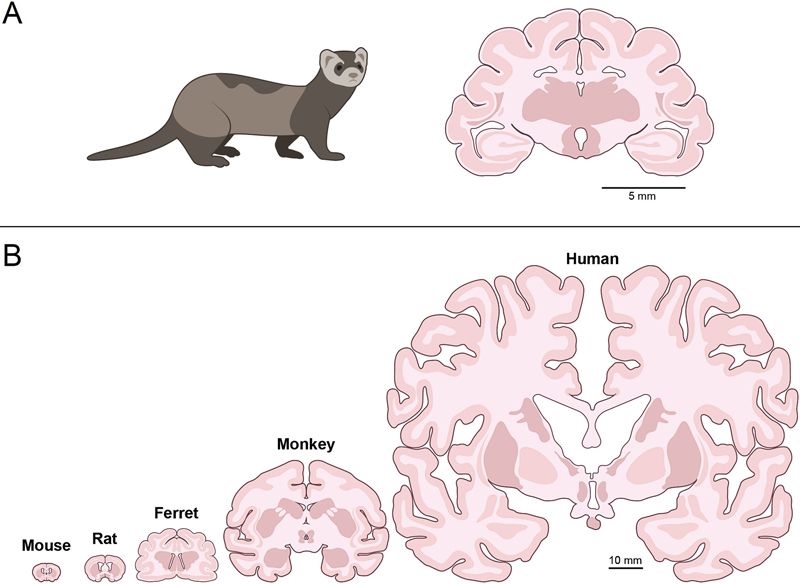
Figure 1. Comparison of chronic traumatic encephalopathy (CTE) and sulcal tau astrogliopathy. A and B (black bars are 900µm and 200µm, respectively): pathognomonic CTE lesion with tau aggregates in neurons (and glia) around small blood vessels at the depth of a sulcus, with tau pathology not restricted to superficial cortical layers. C and D (black bars are 600µm and 200µm, respectively): in contrast, glial tau aggregates in a sulcal depth without perivascular predilection and limited to superficial cortical layers is not diagnostic for CTE, but is rather most fitting of tau astrogliopathy. In addition to a refinement of CTE minimal diagnostic criteria, the Second NINDS/NIBIB Consensus Panel on CTE introduced a working protocol/workflow for the neuropathological evaluation of a brain for CTE, which it hopes to be of service to neuropathologists in the community. Further, the panel ambitiously proposed the first consensus-based scheme for staging the severity of CTE pathology as either “Low CTE” or “High CTE” according to a checklist of criteria. On the clinical side, the year 2021 also saw the publication of the details of the First NINDS Consensus Workshop to Define the Diagnostic Criteria for Traumatic Encephalopathy Syndrome (TES),3 the clinical syndrome which is intended to correspond to CTE neuropathology. The workshop was intended to improve upon the first proposed diagnostic criteria for TES that were published in 2014.4 As part of the workshop, a multispecialty panel of experts in TBI and its sequelae reviewed all published cases of neuropathologically confirmed CTE, and where possible, carefully assessed predictive validity of clinical features in relation to CTE pathology in 298 cases, and used a modified Delphi method to agree upon a restructured, stepwise process for the clinical diagnosis of TES. In short, a diagnosis of TES foremost requires a substantial history of repetitive head impacts and cognitive and/or neurobehavioral dysregulation (core clinical features) with a progressive course unexplained by another disorder. Supportive clinical features for TES which the panel concluded had insufficient predictive value to be included as core clinical features include delayed onset of symptoms, motor symptoms (e.g. parkinsonism), and relatively non-specific psychiatric features (e.g. anxiety, depression, paranoia). Beyond this, the panel also agreed upon provisional criteria (for research purposes) for determining the level of certainty of CTE pathology in a clinical case based on meeting TES criteria, varying levels of impact TBI history (particularly long-standing contact sports history), presence or absence of supportive clinical features as described above, and severity of clinical dementia. There is no evidence, as yet, supporting the predictive value of these clinical criteria based on subsequent neuropathology evaluation. Time will judge the success of the neuropathological diagnostic criteria and staging scheme for CTE, and also of the new proposed clinical criteria for TES. Almost certainly, new issues will arise. However, the continued pursuits of consensus agreement in the face of rapidly evolving, and not uncommonly controversial, data are a promising sign for the future. Additional consensus meetings to evaluate newly emerging data will clearly be needed. CTE in the community Crucial and yet unanswered questions with respect to CTE concern its frequency in the general community, and its impact on members of the general public with a history of TBI (concerns largely raised by frightening media accounts). In the almost two decades since the resurgence of TBI and CTE in the eyes of the public and the scientific community because of its discovery in American football players and other contact sport athletes, collection of materials and data by a number of research centers is starting to bear fruit. With the use of the National Health and Nutrition Examination Surveys (NHNES), whose participants are selected to be representative of the civilian general population, and who undergo a rather thorough interview process, physical examination, and blood and urine collection, Schneider and colleagues reported a large scale analysis of 7,390 participants over the age of 40 years to determine a prevalence estimate of prior head injury with loss of consciousness (LOC) and associated disability.5 Of the 7,390 participants, 944 had a history of self-reported head injury with LOC. Of those 944 with this degree of head injury, 47.4% were noted to be living with a disability in at least one domain of functioning (e.g. activities of daily living, work limitation, memory and confusion limitation, etc.), which was significantly higher (p<0.001) than those without a history of head injury. Extrapolating the data to a prevalence estimate for the general public, the study estimated that there are 11.4 million individuals above the age of 40 with a history of head injury and LOC and who suffer disability in at least one domain of functioning. It should be pointed out that this figure is more than twice the current prevalence estimated for Alzheimer’s disease. As neuropathologists we naturally wonder what pathologies could underlie this staggering new public health data, and perhaps many of us would suspect CTE. However, evidence that has been published from a community cohort in the last year seems to suggest otherwise. In a study entitled “The Delayed Neuropathological Consequences of Traumatic Brain Injury in a Community-Based Sample” published in Frontiers in Neurology,6 authors Postupna et al. reported the neuropathological findings of 532 brains from deceased elderly individuals (average age at death: 87 years) consecutively donated to the Adult Changes in Thought study, which itself is focused on aging and dementia in community-dwelling individuals. One hundred seven of these cases had a history of at least one remote head injury associated with LOC (most participants sustained their first TBI with LOC at less than 25 years of age). Of the 532 cases, only 3 (0.6%) brains had diagnostic CTE lesions. Further, and more surprisingly, none of these 3 cases were among the 107 subjects with a history of TBI and associated LOC. While it may be inappropriate to draw conclusions about the general population from this particular study, when viewed in juxtaposition with the aforementioned NHNES study, it appears that disability relating to one or even a few past instances of TBI with LOC in the general community (as opposed to cohorts selected for repetitive neurotrauma, such as contact sports athletes) is not widely attributable to CTE, and that different mechanisms are likely involved. Future study is necessary. Reducing acetylated tau is neuroprotective following brain injury The literature has long established that TBI is associated with increased risk of developing clinical Alzheimer’s disease and dementia in general, albeit with extremely limited neuropathologic correlation studies.7,8 Nonetheless, this suggests that TBI may potentiate or exacerbate neurodegenerative disease and therefore that neurodegenerative proteins may be a therapeutic target for the prevention of long-term cognitive sequelae of TBI. However, precise pathophysiologic links between TBI and neurodegeneration have proven rather elusive. Using studies that pointed to acetylated tau as increased in CTE, Alzheimer’s disease, and other tauopathies as a basis for their research, Shin et al. conducted a hallmark study to determine whether TBI induces acetylated tau and thus establish a potential link between TBI and neurodegenerative disease, to establish that acetylated tau is neurotoxic, and to investigate whether inhibition of tau acetylation could be neuroprotective after TBI.9 The authors used a multimodal mouse model for TBI, and showed that acetylated tau protein (acetylated at positions K263 and K270, corresponding to K274 and K281 in humans) was rapidly induced by TBI in both the mouse cerebral cortex and hippocampus, selectively in neurons, and that this was dose-dependent. Further, they demonstrated that acetylated tau levels not only rose acutely in injured mice, but remained elevated for months following injury. In the same study, the authors additionally analyzed human frontal cortex specimens of elderly individuals and demonstrated that acetylated tau accumulation was significantly higher in Alzheimer’s disease cases when compared to controls, and amongst the Alzheimer’s disease cases acetylated tau levels were significantly higher in those who had a remote history of TBI(s) versus those who did not. In a separate component of the study, the authors sought to determine if acetylated tau was directly neurotoxic. They conducted both in vitro and in vivo genetic studies on cultured human neuroblasts exposed to acetylated tau and transgenic mice with mutations that mimic tau acetylation at K263 and K270, respectively. In the cultured human cell lines the authors found that tau acetylation specifically increased neuronal cell death, and in the transgenic mice there was a significant degree of axonal degeneration particularly in the cerebral cortex and hippocampus compared to controls after one year of life. In a translation of their work to therapeutics, the authors experimented with 3 agents that are established inhibitors of processes that promote tau acetylation or promotors of tau deacetylation: CGP3466B omigapil (GAPDH nitrosylation inhibitor), salsalate (non-steroidal anti-inflammatory drug and p300/CBP acetyltransferase inhibitor), and aminopropyl carbazole P7C3-A20 (NAMPT activator that increases preservation of NAD+). Administration of all three agents blocked tau acetylation, protected against axonal degeneration, and provided significant protection from neurocognitive deficits following TBI in mice. As if the above data were not enough, the authors finally also demonstrated that acetylated tau levels in mouse plasma were elevated following TBI, establishing the potential for acetylated tau to serve as a blood biomarker for neurodegenerative risk following TBI, and noted that the aforementioned neuroprotective therapies decreased concentrations of acetylated tau in plasma following TBI. Collectively this laudable study, published in Cell, establishes a potential relationship between TBI and neurodegeneration in the form of acetylated tau, demonstrates that acetylated tau is neurotoxic, and provides a basis for the assessment for and protection from neurodegenerative risk after TBI. Updates from the battlefield Published 100 years after Frederick Mott’s seminal reporting of the gross neuropathologic features of acute blast exposure in the brains of World War I military personnel who had died from high explosives,10 a new entity was posited to represent a long-term neuropathological consequence of blast exposure in 2016: interface astroglial scarring (IAS).11 IAS describes a pattern of glial scarring, visible by glial fibrillary acidic protein (GFAP) immunohistochemistry, at brain interfaces (e.g. subpial glial plate, around penetrating cortical vessels, grey-white matter junctions, and structures lining the ventricles). At the time of publication, it was suggested that injury at brain interfaces was compatible with the biophysics of blast waves passing through tissues, though this was presented without experimental data in the brain. As expected, this newly described entity was met with criticism,12 much of which was valid and could not be addressed without more study. The year 2021 brought two important publications in support of IAS as a novel entity that is caused by blast exposure. In the Journal of Neuropathology and Experimental Neurology, Schwerin and colleagues reported the results of a ferret model of blast exposure and provided the first animal correlate of blast-induced IAS.13 Ferrets were chosen because, unlike lissencephalic rodent brains with relatively limited translational capability, the brain of a ferret is more similar to humans in that it is gyrencephalic, has a high white-to-grey matter ratio and a well delineated grey-white matter junction, and has a ventrally positioned hippocampus (see Figure 2). In the study, ferrets were anesthetized and exposed to compressed air shock waves, mimicking exposure to a primary blast wave, and sacrificed after survival periods of 1, 4, or 12 weeks. Immunohistochemistry for GFAP, particularly beginning at 4 weeks survival and in multiply exposed ferrets (four blast exposures compared to one), showed striking astrocyte immunoreactivity precisely at brain interfaces, including the subpial plate, grey-white matter junctions, and surrounding penetrating vessels, thereby reproducing the pattern of IAS that was published in human blast cases. Further, in demonstrating that blast exposure produces astrogliosis in a similar distribution to that seen in human blast cases, the study transversely also provides evidence that ferrets may serve as a translatable animal model for human TBI.
Figure 2. Comparison of ferret brain with human and other animal species. Though relatively small, ferret brains show striking structural similarities with that of primate and human brains, particularly relative to the brains of rodents which themselves are lissencephalic, lack clear grey-white matter interfaces, and have substantially less white matter. The biophysics of a blast wave producing stresses at brain interfaces has also now been supported using an artificial head model. In a study entitled “Localizing Clinical Patterns of Blast Traumatic Brain Injury through Computational Modeling and Simulation” Miller et al. describe a human head model – simplified but nonetheless complete with distinct skull, cerebrospinal fluid, white and grey matter forming gyri and sulci geometrically similar to human brains, vasculature, and ventricles – which was blast-loaded at three different overpressures and from three different directions (front blast, side blast, and a more complex but true-to-life “wall blast” in which a reflecting surface was introduced for the blast wave to bounce back at the head).14 What the authors found was that strain from blast exposure within the model was most significant in perivascular regions, the subpial plate, and the periventricular regions, i.e. an interface pattern of mechanical stress from the blast wave. Simply put, the investigators demonstrated, in an idealized human head model, support for the hypothesis that TBI from blast injury primarily concerns structural interfaces in the brain. Further study of different forms of TBI, especially impact TBI, using this model will be critical to additional understanding and establishing its utility in the study of human TBI. A radiologic signature for diffuse axonal injury In what may come as a surprise to some neuropathologists who are quite familiar with this entity, diffuse axonal injury (DAI) was purely a pathologic diagnosis without a sensitive or specific radiologic correlate prior to the year 2021. DAI is essentially invisible to conventional computed tomography (CT) and magnetic resonance imagining (MRI) scans. In a landmark study, authors Benjamini et al. applied multidimensional MRI to ex vivo samples of human brain with and without neuropathologically confirmed DAI (10 cases in total).15 Multidimensional MRI is an emerging imaging technique that encodes multiple contrasts (e.g. T1, T2) together to provide a “multidimensional” distribution of these components combined with artificial intelligence to allow for enhanced separation of different biological elements within a heterogeneous tissue sample. Using this new technique, the authors were able to identify a unique MRI signature that allowed them to produce radiologic findings in tissue that precisely mirrored the distribution of APP immunohistochemistry on sections cut from the same samples, and further allowed them to blindly differentiate all of the DAI and non-DAI cases. Though this study was performed on ex vivo tissues and utilized preclinical MRI technology, the authors have nonetheless provided a bedrock for the potential future clinical detection of DAI and more subtle axonal injury in living patients. With further improvements of the multidimensional MRI modality, studies scanning whole brains and brains in vivo, and advancements in clinical MRI system technology, this imaging breakthrough may soon redefine the clinical assessment of TBI. Long-term structural changes in the brain following TBI with clinical correlation There were a number of imaging studies published in 2021 that assessed the volume and/or integrity of a variety of brain structures in the subacute and chronic stages in mild TBI patients. Churchill et al. describe reductions of cingulate gyrus blood flow, particularly in the posterior cingulate chronically (1 year after return-to-play) in adult contact sport athletes with a history of concussion, along with increased mean diffusivity in the corpus callosum (CC) (toward the splenium), as compared to control subjects, indicating potential long-term effects of mild TBI on these midline brain structures.16 In a related study, Wang et al. conducted diffusion tensor imaging and functional MRI on 42 mild TBI patients and 42 matched controls.17 In the TBI patients, they found evidence of structural impairment in the CC which expanded from the anterior-to-midbody of the CC in acute/subacute phases following TBI into both more anterior and posterior regions of the CC in chronic phase (6-12 months), with corresponding evidence of impairment in interhemispheric connectivity. Further, these findings correlated to reduced executive function parameters on clinical testing of the patients. Finally, authors Meier et al. assessed the hippocampus via MRI in a group of 106 collegiate athletes.18 They report that hippocampal volume was reduced in athletes with a history of concussion(s), in comparison to those without, and further that hippocampal volume was inversely correlated with the number of previous concussions. This was observed along with a greater association of various neuropsychiatric symptoms. As it pertains to severe TBI, authors Tomaiulo et al. describe the long-term MRI findings in a group of 25 patients with a history of severe non-missile TBI but without large focal lesions taken at one year and nine years following head injury. They report significant volume reduction in both grey matter (frontotemporal region, crests of gyri, amygdala, hippocampus, basal ganglia, and thalamus) and white matter (CC, fornix, parasagittal white matter, cerebral peduncles) at one year following injury.19 At nine years, there were no significant increases in grey matter reduction, but white matter reduction continued particularly in the posterior body of the CC, and in the white matter under-surface of several cerebral lobes. The above studies, all image-based, are alarming and should serve as a call to action for neuropathologists interested in studying TBI. The need to pathologically characterize and corroborate the growing myriad of long-term structural changes that occur in the brain from TBI as suggested by radiologic evaluation is obvious. In closing As you have read, there were several important developments in the field of neurotrauma in the year 2021. Given the sheer volume of publications produced in the field over this time, this article could easily have continued on toward a tome’s length, and admittedly it was quite difficult to refrain from discussing more. However, we hope that you as the reader have enjoyed this summation of the literature that we chose to highlight. To conclude this writing, we would like to bring to attention a poignant short article entitled “The Banality of Head Injury in The Punisher”, written by Daniel M. Donaldson et al. and published in Lancet Neurology in 2021.20 In this article, the authors examined 26 episodes of the action- and violence-packed TV series The Punisher, which focuses on an antihero from the Marvel comic universe who employs vigilante, and usually lethal, methods to fight crime. In their assessment, the authors identified 125 instances of head trauma inflicted on characters in the show, including 12 inflicted on The Punisher himself, and determined the severity of the TBI events (as best it could be achieved) by the Glasgow Coma Scale. By their assessment, 62% of the head injuries depicted in the show were severe, with an initial Glasgow Coma Scale of 3 in most cases. However, in almost all individuals who survived these severe TBI events, neurologic symptoms following the initial neurological impairment were virtually nonexistent (i.e. no abnormality in mental status after return of consciousness, no lasting neurocognitive deficits, etc.). Indeed, all 12 TBI events suffered by The Punisher, even when severe, resulted in no neurologic deficits following a return of consciousness. Further, significant or long-term structural damage to the face/skull was not appreciated in all but 1 case, even in circumstances where there was substantial disfigurement of other parts of the body from the same general traumatic events. Of course, this phenomenon is far from unique to The Punisher, as consumers of action TV series and movies are well aware. Instead, the authors’ analysis of this one TV show highlights how inaccurately violence, particularly TBI, is presented in media productions and thus to the public as a whole. The authors suggest that the portrayal of the severity (or lack thereof) of TBI in media may augment our perception of TBI and expected outcomes from TBI in real life, and we agree with this supposition. What can be done about this is uncertain, but as neuropathologists and TBI researchers we are uniquely suited to have a seat at the table. Disclaimer The information/content, conclusions, and/or opinions expressed herein do not necessarily represent the official position or policy of, nor should any official endorsement be inferred on the part of, Uniformed Services University, the Department of Defense, the US Veterans Administration, the U.S. Government or the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. Conflicts of Interest The authors do not have any conflict of interest to declare. References 1. Bieniek KF, Cairns NJ, Crary JF, et al. (TBI/CTE Research Group). The second NINDS/NIBIB consensus meeting to define neuropathological criteria for the diagnosis of chronic traumatic encephalopathy. J Neuropathol Exp Neurol. 2021;80(3):210-219. https://doi.org/10.1093/jnen/nlab001 2. McKee AC, Cairns NJ, Dickson DW, et al. The first NINDS/NIBIB consensus meeting to define neuropathological criteria for the diagnosis of chronic traumatic encephalopathy. Acta Neuropathol. 2016;131(1):75-86. https://doi.org/10.1007/s00401-015-1515-z 3. Katz DI, Bernick C, Dodick DW, et al. National Institute of Neurological Disorders and Stroke consensus diagnostic criteria for traumatic encephalopathy syndrome. Neurology. 2021;96(18):848-863. https://doi.org/10.1212/WNL.0000000000011850 4. Montenigro PH, Baugh CM, Daneshvar DH, et al. Clinical subtypes of chronic traumatic encephalopathy: literature review and proposed research diagnostic criteria for traumatic encephalopathy syndrome. Alzheimers Res Ther. 2014;6(5):68. https://doi.org/10.1186/s13195-014-0068-z 5. Schneider ALC, Wang D, Gottesman RF, Selvin E. Prevalence of disability associated with head injury with loss of consciousness in adults in the United States: a population-based study. Neurology. 2021;97(2):e124-e135. https://doi.org/10.1212/WNL.0000000000012148 6. Postupna N, Rose SE, Gibbons LE, et al. The delayed neuropathological consequences of traumatic brain injury in a community-based sample. Front Neurol. 2021;12:624696. https://doi.org/10.3389/fneur.2021.624696 7. Li Y, Li Y, Li X, et al. Head injury as a risk factor for dementia and Alzheimer's disease: a systematic review and meta-analysis of 32 observational studies. PLoS One. 2017;12(1):e0169650. https://doi.org/10.1371/journal.pone.0169650 8. Shively S, Scher AI, Perl DP, Diaz-Arrastia R. Dementia resulting from traumatic brain injury: what is the pathology? Arch Neurol. 2012;69(10):1245-1251. https://doi.org/10.1001/archneurol.2011.3747 9. Shin MK, Vázquez-Rosa E, Koh Y, et al. Reducing acetylated tau is neuroprotective in brain injury. Cell. 2021;184(10):2715-2732.e23. https://doi.org/10.1016/j.cell.2021.03.032 10. Mott FW. The effects of high explosives upon the central nervous system. Lecture I. Lancet. 1916;187(4824):331–338. https://doi.org/10.1016/S0140-6736(00)52963-8 11. Shively SB, Horkayne-Szakaly I, Jones RV, Kelly JP, Armstrong RC, Perl DP. Characterisation of interface astroglial scarring in the human brain after blast exposure: a post-mortem case series. Lancet Neurol. 2016;15(9):944-953. https://doi.org/10.1016/S1474-4422(16)30057-6 12. Hoge CW, Wolf J, Williamson D. Astroglial scarring after blast exposure: unproven causality. Lancet Neurol. 2017;16(1):26. https://doi.org/10.1016/S1474-4422(16)30342-8 13. Schwerin SC, Chatterjee M, Hutchinson EB, et al. Expression of GFAP and tau following blast exposure in the cerebral cortex of ferrets. J Neuropathol Exp Neurol. 2021;80(2):112-128. https://doi.org/10.1093/jnen/nlaa157 14. Miller ST, Cooper CF, Elsbernd P, Kerwin J, Mejia-Alvarez R, Willis AM. Localizing clinical patterns of blast traumatic brain injury through computational modeling and simulation. Front Neurol. 2021;12:547655. https://doi.org/10.3389/fneur.2021.547655 15. Benjamini D, Iacono D, Komlosh ME, Perl DP, Brody DL, Basser PJ. Diffuse axonal injury has a characteristic multidimensional MRI signature in the human brain. Brain. 2021;144(3):800-816. https://doi.org/10.1093/brain/awaa447 16. Churchill NW, Hutchison MG, Graham SJ, Schweizer TA. Acute and chronic effects of multiple concussions on midline brain structures. Neurology. 2021;97(12):e1170-e1181. https://doi.org/10.1212/WNL.0000000000012580 17. Wang Z, Zhang M, Sun C, et al. Single mild traumatic brain injury deteriorates progressive interhemispheric functional and structural connectivity. J Neurotrauma. 2021;38(4):464-473. https://doi.org/10.1089/neu.2018.6196 18. Meier TB, España LY, Kirk AJ, et al. Association of previous concussion with hippocampal volume and symptoms in collegiate-aged athletes. J Neurotrauma. 2021;38(10):1358-1367. https://doi.org/10.1089/neu.2020.7143 19. Tomaiuolo F, Cerasa A, Lerch JP, et al. Brain neurodegeneration in the chronic stage of the survivors from severe non-missile traumatic brain injury: a voxel-based morphometry within-group at one versus nine years from a head injury. J Neurotrauma. 2021;38(2):283-290. https://doi.org/10.1089/neu.2020.7203 20. Donaldson DM, Holtmann H, Nitschke J, et al. The banality of head injury in The Punisher. Lancet Neurol. 2021;20(7):509. https://doi.org/10.1016/S1474-4422(21)00160-5
Copyright: © 2022 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |