|
|
|
Free Neuropathology 3:18 (2022) |
|
Letter |
|
Amygdala granular fuzzy astrocytes as lesions preceding development of argyrophilic grains: data from 239 autopsy cases |
|
Osamu Yokota1,2,3,4, Tomoko Miki1,2,3,4, Chikako Ikeda2,3, Hideki Ishizu3, Takashi Haraguchi4, Akinori Miyashita5, Takeshi Ikeuchi5, Shintaro Takenoshita6, Seishi Terada2 |
|
1 Department of Psychiatry, Kinoko Espoir Hospital, Kasaoka, Japan |
|
Corresponding author: |
|
Submitted: 15 June 2022 Accepted: 21 July 2022 Copyedited by: Irati Bastero Published: 27 July 2022 |
|
Additional resources and electronic supplementary material: supplementary material |
|
Keywords: Amygdala, Argyrophilic grain disease, ARTAG, Blood vessel, Granular fuzzy astrocyte, Tau |
|
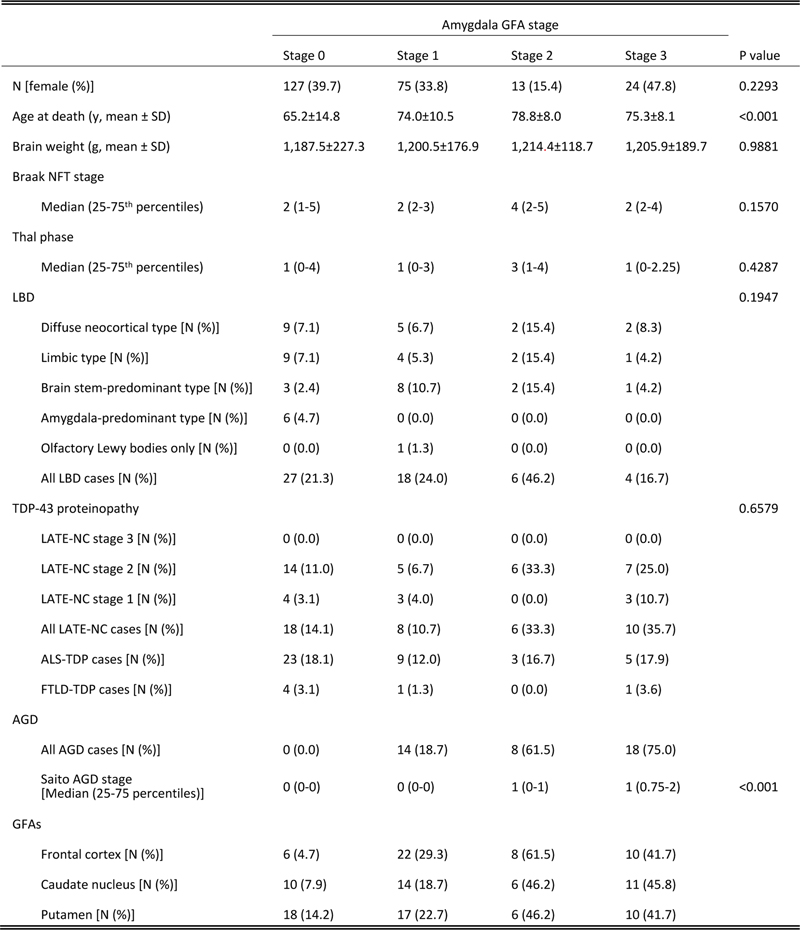
Cases of argyrophilic grain disease (AGD) frequently have astrocytes containing non-argyrophilic tau-positive fine granules in the foot processes sprouting from cell bodies in the amygdala. They were first called bush-like astrocytes by Botez et al. [1], and later they were classified as one of the age-related tau astrogliopathies and re-named granular fuzzy astrocytes (GFAs) [2]. In our previous studies, the formation of GFAs was not simply associated with age alone, and their distributions were influenced by underlying tauopathies [3,4]. Especially in AGD cases, GFAs preferentially develop in the amygdala rather than the frontal cortex and striatum [3]. Kovacs et al. previously noted the possibility that GFAs in the amygdala might be a forerunner of argyrophilic grains [5]. However, there is no comprehensive pathological data regarding the relationship between the frequencies and severities of AGD and GFAs in the amygdala, and whether argyrophilic grains develop in the absence of amygdala GFAs remains unclear. To address these issues, first, we analyzed the relationship between the presence or absence of AGD and the severity of amygdala GFAs in a case series. Then, their spatial relationship was examined using double staining with the Gallyas method and anti-phospho-tau (AT8) immunohistochemistry. Among a total of 1,166 autopsy cases registered in our database, 474 cases that were evaluated using modern standardized methods, including a panel of immunohistochemistry, modified Bielschowsky silver stain, and Gallyas-Braak silver stain from 2001 to 2022, were selected (Supplementary file 1). All cases died in psychiatric hospitals or neurological departments of general hospitals. Of these cases, we extracted 263 cases for which semiquantitative data of the AT8-positive GFAs, as well as the Saito AGD stage [6] (the distribution of argyrophilic grains in the cerebrum) assessed using the Gallyas method, are available. Then, 24 cases having progressive supranuclear palsy, corticobasal degeneration, Pick’s disease, globular glial tauopathies, post-encephalitic parkinsonism, and myotonic dystrophy were excluded because distinct tau-positive astrocytic lesions were noted. Finally, 239 cases were included in the present study. In all of these cases, GFAs were semiquantitatively assessed in the frontal cortex, caudate nucleus, putamen, and amygdala on AT8-stained sections, using the following grading system (GFA stage): stage 0, no lesion in the anatomical region (i.e., the superior frontal gyrus, caudate nucleus, putamen, and amygdala); stage 1, more than one lesion in the anatomical region but less than one lesion per ×200 visual field; stage 2, one lesion per ×200 visual field; or stage 3, two or more lesions per ×200 visual field. Among the 239 cases, 112 had at least one GFA in the amygdala, while 127 lacked amygdala GFAs (amygdala GFA stage 0) (Table 1). The age at death was significantly higher in the amygdala GFA stage 1, 2, and 3 groups than in the amygdala GFA stage 0 group (p<0.001, 0.0025, and 0.0023, Kruskal-Wallis and Steel-Dwass tests). However, the sex ratio, brain weight, Braak stage, Thal phase, proportions of Lewy body disease (LBD) pathological subtypes, and proportions of TAR DNA-binding protein 43 (TDP-43) proteinopathy pathological subtypes did not significantly differ between the four amygdala GFA stage groups. Table 1. Demographic data in all subjects stratified by severity of GFAs
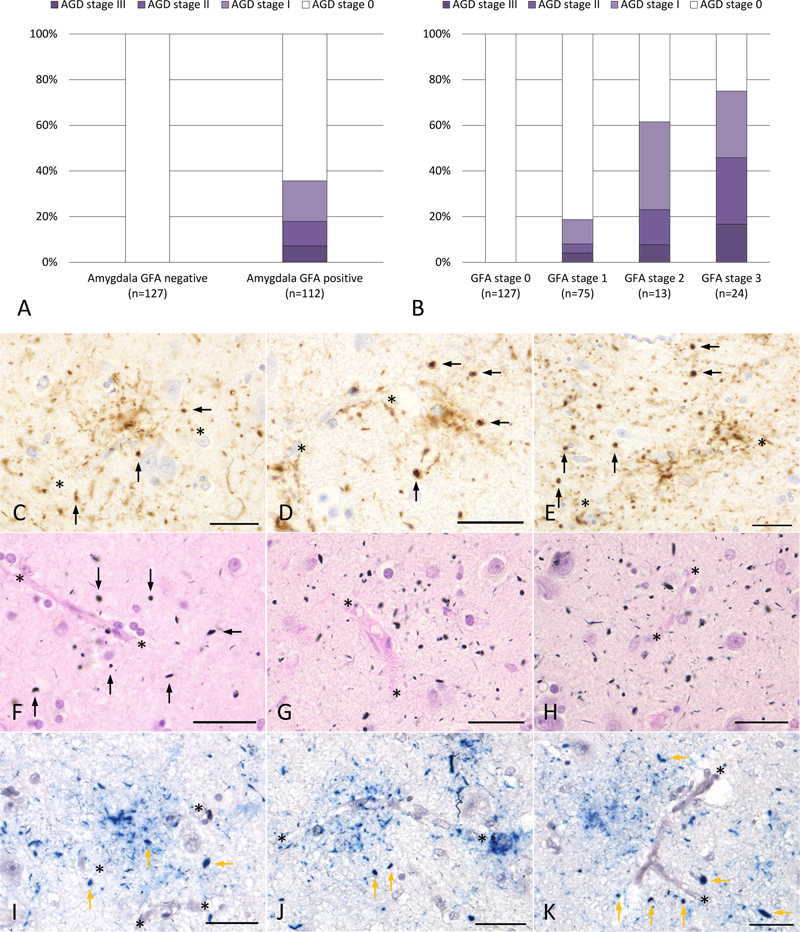
GFA: granular fuzzy astrocyte, AGD: argyrophilic grain disease, N: number of cases, NFT: neurofibrillary tangles, LBD: Lewy body disease, LATE-NC: Limbic-predominant age-related TDP-43 encephalopathy neuropathological change, ALS-TDP: amyotrophic lateral sclerosis with TDP-43-positive inclusions, FTLD-TDP: frontotemporal lobar degeneration with TDP-43-positive inclusions. AGD was noted only when a case had at least one GFA in the amygdala; that is, there was no case that lacked amygdala GFAs but had AGD (Figure 1A). On the other hand, cases having amygdala GFAs did not always have AGD: of all 112 cases having amygdala GFAs, 40 cases (35.7%) had argyrophilic grains in the amygdala (Figure 1A). The frequency of cases with AGD increased parallel to the amygdala GFA stage: 18.7% in GFA stage 1, 61.5% in GFA stage 2, and 75.0% in GFA stage 3 groups (Figure 1B). The Saito AGD stage was significantly correlated with the amygdala GFA stage (ρ=0.5878, p<0.001, Spearman rank-order correlation test). The binomial logistic regression analysis was used to evaluate whether the age at death, Braak stage, Thal phase, frontal lobe GFA stage, caudate nucleus GFA stage, putamen GFA stage, or amygdala GFA stage could be used as possible predictors of the development of AGD, and it demonstrated that the amygdala GFA stage (the standardized partial regression coefficient (β), 1.79; odds ratio, 6.63; 95% confidence interval (CI), 3.57–12.32; p<0.001), the age at death (β, 1.34; odds ratio, 1.09; 95% CI, 1.02–1.16; p<0.001), the frontal lobe GFA stage (β, 0.62; odds ratio, 3.47; 95% CI, 1.06–11.33; p=0.0391), and the putamen GFA stage (β, 0.64; odds ratio, 3.10; 95% CI, 1.005–9.56; p=0.0490) were significant independent predictors of the occurrence of argyrophilic grains.
Figure 1. Relationship between the formation of AGD and amygdala GFAs As previously reported [3,4], GFAs with tau-positive astrocytic endfeet were often in contact with blood vessel walls on AT8-immunostained sections of the amygdala (Figures 1C-1E). In addition, a small number of AT8-positive argyrophilic grains were often scattered around the GFAs (Figures 1C-1E). Although GFAs are not stained by the Gallyas method, a potential association between argyrophilic grains and vessels was also noted on Gallyas-stained sections: a few argyrophilic grains are scattered at a distance around vessels (Figures 1F-1H). Likewise, double staining with the Gallyas method and AT8 immunohistochemistry showed the proximity of argyrophilic grains, GFAs, and blood vessels (Figures 1I-1K). Noteworthy, these phenomena could be observed only in regions where argyrophilic grains were relatively scarce rather than abundant. The findings presented here support the notion that amygdala GFAs may develop prior to the formation of argyrophilic grains in the amygdala [5] and suggest that amygdala GFAs may play some role in the occurrence of argyrophilic grains, which are preferably formed in the dendrospinal portion of neurons [7]. These findings also suggest that at least some cases having amygdala GFAs but lacking argyrophilic grains may be in the earliest ‘pre-grain’ stage in the pathological process of AGD (Supplementary file 2). Whether amygdala GFAs affect cognitive function and psychiatric status, especially in elderly people, also needs to be explored. Finally, Table 1 shows that some cases had GFAs in the frontal cortex, caudate nucleus, and/or putamen even when the case lacked amygdala GFAs and argyrophilic grains (amygdala GFA stage 0). Based on our previously reported findings [3], this fronto-striatal-predominant distribution pattern of GFAs led us to consider the possibility that the case has an early pathological process of progressive supranuclear palsy (PSP). For a better understanding of the relationship between argyrophilic grains, GFAs, subcortical neuronal tau accumulation, and PSP as the pathological disease entity, the sequence of the appearance of these lesions and pathological conditions needs to be further examined. Declarations Ethics approval Autopsy was carried out after written informed consent was obtained from family members, and all experiments in this study were approved by the ethical committees of the Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, National Hospital Organization Minami-Okayama Medical Center, Niigata University, and Zikei Hospital. Competing interests OY is an editorial board member but was not involved in the editorial handling of this manuscript. The other authors declare that they have no conflicts of interest. Funding This work was supported by grants from the Strategic Research Program for Brain Sciences from the Japan Agency for Medical Research and Development (AMED, JP22wm0425019, JP22dk020704) and grants from the Zikei Institute of Psychiatry. Authors’ contributions OY, TM, ShT, and SeT macroscopically and histopathologically assessed all subjects; CI, HI, and TH conducted the autopsies; NH, AM, and TI administered the brain bank; OY and TM drafted the manuscript. All authors reviewed the manuscript. Acknowledgements We thank Ms. Y. Matsuo for her technical assistance. References 1. Botez G, Probst A, Ipsen S, et al.: Astrocytes expressing hyperphosphorylated tau protein without glial fibrillary tangles in argyrophilic grain disease. Acta Neuropathol 1999;98:251-6. https://doi.org/10.1007/s004010051077. 2. Kovacs GG, Ferrer I, Grinberg LT, et al.: Aging-related tau astrogliopathy (ARTAG): harmonized evaluation strategy. Acta Neuropathol 2016;131:87–102. https://doi.org/10.1007/s00401-015-1509-x. 3. Miki T, Yokota O, Haraguchi T, et al.: Factors associated with development and distribution of granular/fuzzy astrocytes in neurodegenerative diseases. Brain Pathol 2020;30:811-830. https://doi.org/10.1111/bpa.12843. 4. Ikeda C, Yokota O, Nagao S, et al.: The relationship between development of neuronal and astrocytic tau pathologies in subcortical nuclei and progression of argyrophilic grain disease. Brain Pathol 2016;26:488-505. https://doi.org/10.1111/bpa.12319. 5. Kovacs GG, Xie SX, Robinson JL, et al.: Sequential stages and distribution patterns of aging-related tau astrogliopathy (ARTAG) in the human brain. Acta Neuropathol Commun 2018;6:50. https://doi.org/10.1186/s40478-018-0552-y. 6. Saito Y, Ruberu NN, Sawabe M, et al.: Staging of argyrophilic grains: an age-associated tauopathy. J Neuropathol Exp Neurol 2004;63:911-918. https://doi.org/10.1093/jnen/63.9.911. 7. Ikeda K, Akiyama H, Kondo H, et al.: A study of dementia with argyrophilic grains. Possible cytoskeletal abnormality in dendrospinal portion of neurons and oligodendroglia. Acta Neuropathol 1995;89:409-414. https://doi.org/10.1007/BF00307644.
Copyright: © 2022 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |