|
|
|
Free Neuropathology 3:16 (2022) |
|
Review |
|
Pigmented ependymoma, a tumor with predilection for the middle-aged adult: case report with methylation classification and review of 16 literature cases |
|
Alexander S. Himstead, BS1,2, Mari Perez-Rosendahl, MD2, Gianna M. Fote, PhD1, Angie Zhang, MD1, Michael G. Kim, MD1, David Floriolli, MD3, Martha Quezado, MD4, Kenneth Aldape, MD4, Drew Pratt, MD4, Zied Abdullaev, PhD4, Edwin S. Monuki, MD, PhD2, Frank P. K. Hsu, MD, PhD1, William H. Yong, MD, FCAP2 |
|
1 Department of Neurosurgery, University of California, Irvine School of Medicine, Orange, CA, USA |
|
Corresponding author: |
|
Submitted: 09 June 2022 Accepted: 21 June 2022 Copyedited by: Mónica Miranda Published: 08 July 2022 |
|
Additional resources and electronic supplementary material: supplementary material |
|
Keywords: Pigmented; Ependymoma; Lipofuscin; Fourth ventricle; Case report; Posterior fossa; Methylation |
|
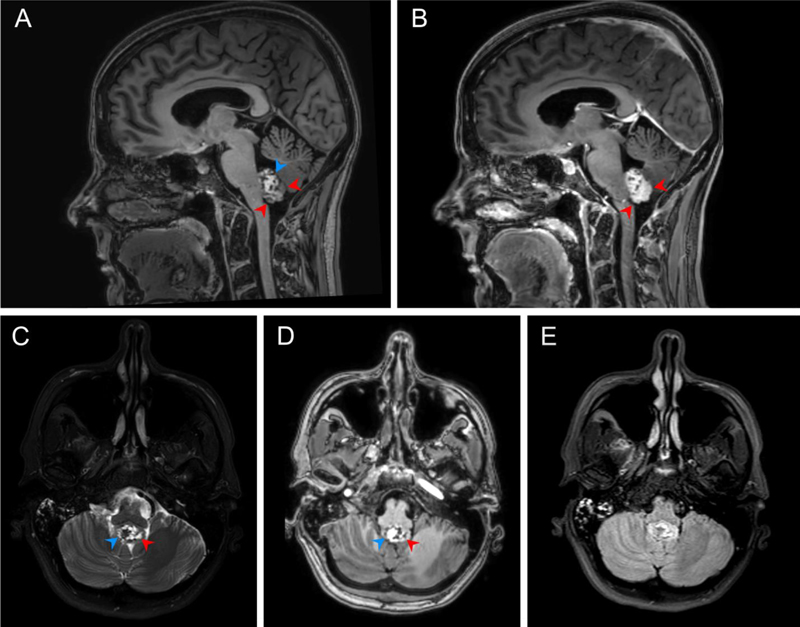
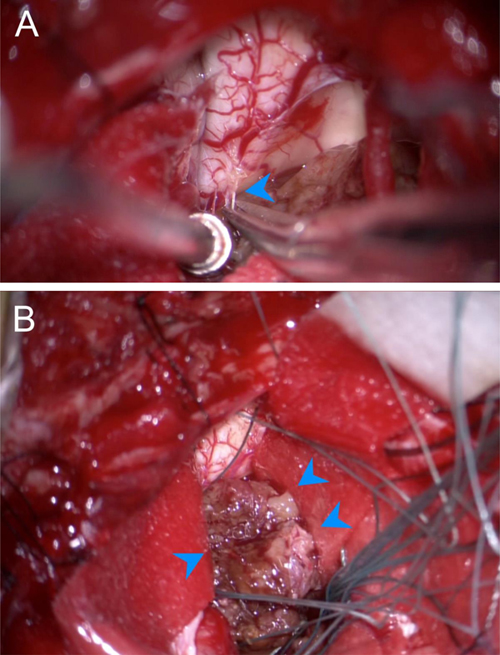
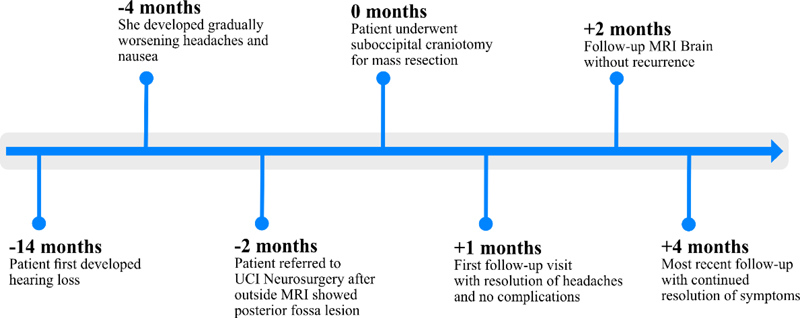
Abstract Ependymomas have rarely been described to contain pigment other than melanin, neuromelanin, lipofuscin or a combination. In this case report, we present a pigmented ependymoma in the fourth ventricle of an adult patient and review 16 additional cases of pigmented ependymoma from the literature. A 46-year-old female showed up with hearing loss, headaches, and nausea. Magnetic resonance imaging revealed a 2.5 cm contrast-enhancing cystic mass in the fourth ventricle, which was resected. Intraoperatively, the tumor appeared grey-brown, cystic, and was adherent to the brainstem. Routine histology revealed a tumor with true rosettes, perivascular pseudorosettes and ependymal canals consistent with ependymoma, but also showed chronic inflammation and abundant distended pigmented tumor cells that mimicked macrophages in frozen and permanent sections. The pigmented cells were positive for GFAP and negative for CD163 consonant with glial tumor cells. The pigment was negative for Fontana-Masson, positive for Periodic-acid Schiff and autofluorescent, which coincide with characteristics of lipofuscin. Proliferation indices were low and H3K27me3 showed partial loss. H3K27me 3 is an epigenetic modification to the DNA packaging protein Histone H3 that indicates the tri-methylation of lysine 27 on histone H3 protein. This methylation classification was compatible with a posterior fossa group B ependymoma (EPN_PFB). The patient was clinically well without recurrence at three-month post-operative follow-up appointment. Our analysis of all 17 cases, including the one presented, shows that pigmented ependymomas are most common in the middle-aged with a median age of 42 years and most have a favorable outcome. However, one patient that also developed secondary leptomeningeal melanin accumulations died. Most (58.8%) arise in the 4th ventricle, while spinal cord (17.6%) and supratentorial locations (17.6%) were less common. The age of presentation and generally good prognosis raise the question of whether most other posterior fossa pigmented ependymomas may also fall into the EPN_PFB group, but additional study is required to address that question. Introduction Primary pigmented tumors of the central nervous system (CNS) are rare entities and often contain melanin.1 Primary pigmented intracranial tumors include melanoma, melanocytoma, schwannomas,2 meningiomas,1 and, less commonly, gliomas,3 neurocytomas,4 ependymomas and choroid plexus tumors.2 Ependymomas are glial neoplasms found, most commonly, intracranially in the posterior fossa of children and within the spinal cord of adults.5 Prognosis primarily depends on location, with intracranial ependymomas harboring worse outcomes than spinal variants.6,7 Pigmented ependymomas are most commonly melanotic,8 although these neoplasms are often incompletely characterized in the literature. Furthermore, cases of pigmentation with neuromelanin and lipofuscin have been previously described.2,9 Nowadays, subtyping of ependymomas includes genetic and methylation profiling, therefore several methylation profiles have emerged which may correlate with clinical prognosis.10 Here, we describe a pigmented ependymoma of the fourth ventricle that contains lipofuscin and has a methylation profile consistent with a posterior fossa group B ependymoma (EPN_PFB). We also review the available published cases pertaining to pigmented ependymomas by characterizing their age distribution, location, clinical features and outcomes. Case History A 46-year-old Hispanic female presented with hearing loss for one year and worsening headaches and nausea for two months. Her physical examination revealed no focal neurological deficits. Magnetic resonance imaging (MRI) revealed a 2.2 x 1.5 x 2.6 cm mass involving the floor of the fourth ventricle, which showed marked intrinsic T1 hyperintensity, variable T2 signal (with areas of both hyperintensity and hypointensity), predominantly hyperintense fluid-attenuated inversion recovery (FLAIR) signal and areas of contrast-enhancement (Fig. 1). After informed consent to surgery and involvement in research (IRB ethics approval deferred as University of California, Irvine policy permits reports of up to 3 individuals), she underwent a suboccipital craniotomy for resection of the mass. Intraoperatively, the tumor appeared as a grey-brown cystic mass within the fourth ventricle that was tightly adherent to the posterior inferior cerebellar arteries and lower brainstem (Fig. 2). Radiographic gross-total resection (GTR) was achieved. The patient’s postoperative course was uncomplicated, and she was without radiographic recurrence and satisfied with her treatment at one- and three-month follow-up appointments (Fig. 3).
Figure 1. A. Sagittal pre-contrast T1 demonstrates an intraventricular mass involving the floor of the fourth ventricle and heterogenous T1 signal with areas of prominent intrinsic T1 hyperintensity (blue arrow), areas isointense to brain (red arrows), and scattered areas of low signal. B. Fat saturated sagittal post-contrast T1 demonstrates enhancement of the previously isointense portions (red arrows) with persistent areas of low signal. C. Axial fat saturated T2 at the level of the lesion demonstrates cystic areas of high T2 signal (red arrow) which correspond to low intensity of pre-contrast T1. D. A prominent low signal area on T2 is intrinsically bright on T1 (blue arrow), suggesting high protein and/or lipid contents. E. Axial FLAIR demonstrates predominantly iso- to hyperintense signal.
Figure 2. Intraoperative photographs of the tumor demonstrating: A. dissection of arachnoid bands tethering the tumor to the floor of the fourth ventricle and B. the macroscopic appearance of the lesion with notable grey-brown color (blue arrows).
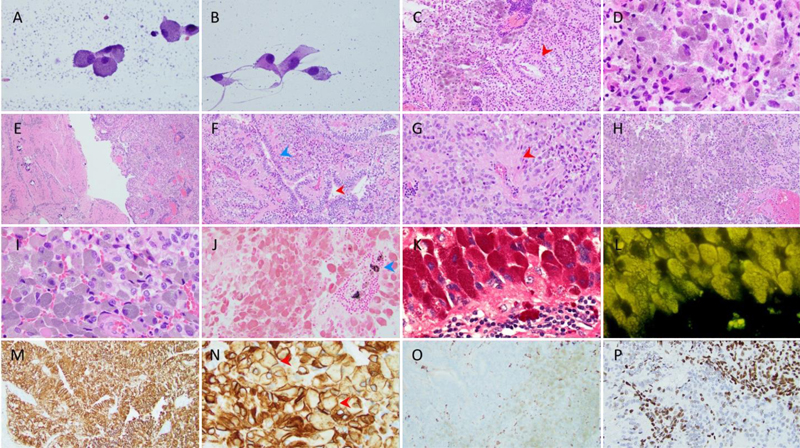
Figure 3. Patient care timeline. Pathology Intraoperative smears showed pigmented cells often with swollen granular cytoplasm mimicking macrophages (Fig. 4A), as well as a population of cells with ovoid nuclei and a moderate amount of cytoplasm with variably epithelioid features (Fig. 4B). Intraoperative frozen sections showed perivascular chronic inflammation, abundant pigmented cells and sheets of tumor cells with epithelial surfaces mimicking glands, but reflecting ependymal rosettes or canals (arrowhead) (Fig. 4C). The pigment was fine and grey-brown in micrographs of the frozen section (Fig. 4D).
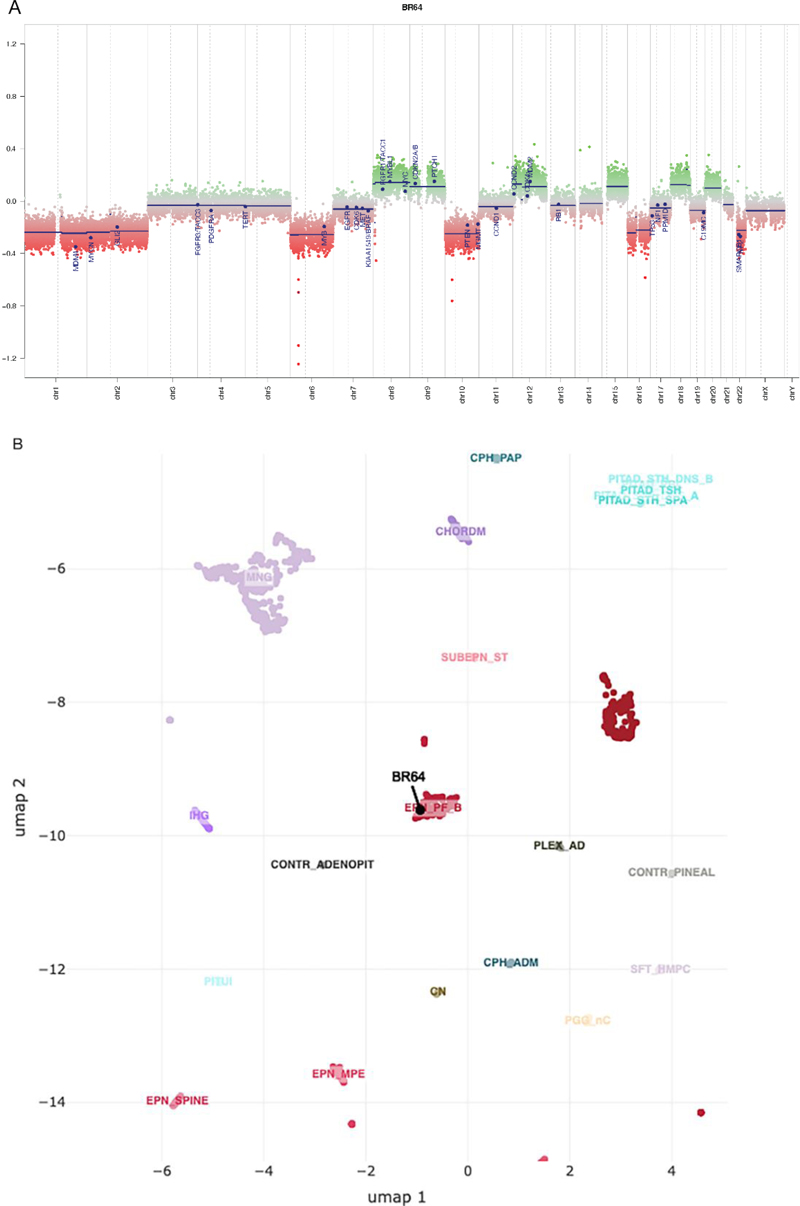
Figure 4. Staining is with hematoxylin and eosin (H&E) unless otherwise specified. A. (400X) Smear- swollen pigmented tumor cells. B. (400X) Smear- unpigmented and pigmented tumor cells. C. (100X) Frozen section- “epithelial” surfaces resembling glands (red arrowhead). D. (400X) Frozen section- Fine, grey-brown pigment. Figures E-I are from permanent sections. E. (40X) Cellular tumor (right fragment) and areas reminiscent of subependymoma gliopil (left fragment). F. (100X) Ependymal canal (blue arrowhead) and pseudopapillary configuration (red arrowhead). G. (200X) Perivascular pseudorosette (red arrowhead). H. (100X), I. (400X) Swollen pigmented cells. J. (200X) Fontana-Masson stain- tumor cells negative; few perivascular macrophages positive (blue arrowhead). K. (600X) PAS stain. L. (600X) Fluorescence microscopy shows autofluorescence. M. (200X), N. (400X) GFAP- pigmented cells immunopositive (red arrowheads). O. (200X) CD163- tumor cells negative; scattered microglia immunopositive. P. (200X) H3K27me3- loss in subset of tumor cells. Clicking into the figure will lead you to the full virtual slide. Permanent sections showed tumor tissue that was mostly cellular (right fragment) with minor areas where the background consisted of an eosinophilic gliopil (left fragment) (Fig. 4E). Ependymal canals (blue arrowhead) were focally prominent, sometimes suggesting a papillary configuration (red arrowhead) (Fig. 4F). Perivascular pseudorosettes could also be seen (Fig. 4G). Swollen cells with grey-brown pigment were abundant in some areas (Fig. 4H, I). The pigmented cells were negative for melanin and neuromelanin by Fontana-Masson (Fig. 4J); only scant focal often coarser and/or larger black-staining pigment was seen extracellularly and in a few perivascular macrophages (arrowhead). These cells stained strongly with PAS (Fig. 4K) and were autofluorescent with fluorescence microscopy (Fig. 4L). Concerning the GFAP staining, the tumor was diffusely and strongly positive (Fig. 4M), as were the swollen pigmented cells, which showed GFAP staining at the cytoplasmic periphery (arrowheads) consistent with a glial origin (Fig. 4N). Both unpigmented and pigmented tumor cells were negative for the macrophage marker CD163; with only scattered, interspersed, small darkly staining microglia (Fig. 4O). Collectively, these findings indicated a lipofuscin-pigmented ependymoma. An H3K27me3 immunostain showed immunonegativity in approximately 20-30% of tumor cells, but did not show global loss (Fig. 4P). Whole slide digital images of frozen H&E (sFig. 1), permanent H&E (sFig. 2), PAS (sFig. 3), GFAP (sFig. 4) and H3K27me3 (sFig. 5) slides are available in the Supplement section. DNA Methylation Arrays and Analysis Methylation profiling was performed at the National Institutes of Health (NIH), Bethesda, MD, USA. Genomic DNA was extracted from formalin-fixed paraffin-embedded (FFPE) tissue sections on slides using an AllPrep DNA/RNA FFPE kit (Qiagen, Venlo, Netherlands). The DNA was bisulfite-converted using the EZ DNA Methylation Kit (Zymo Research, Irvine, CA, USA), and processed to create a beadchip (850K methylation sites) using the Infinium Methylation EPIC kit (Illumina, San Diego, CA, USA). The beadchip was then scanned on the iScan reader (Illumina). Methylation profiling was carried out through an NIH pipeline using UMAP, the NCI-EPIC methylation classifier, and the Heidelberg classifier (brain, versions 11b6 and 12.5), obtained from the German Cancer Research Center in Heidelberg, Germany. The sample was classified as ependymoma, posterior fossa group B with a score of 0.47 on version 11b6, and the same methylation class with a higher score of 0.98 on version 12.5 of the Heidelberg classifier. On the UMAP, this sample embedded with the EPN_PFB cluster (Fig. 5). The consensus methylation profile, in the context of the clinical and histopathologic features, supported EPN_PFB, CNS World Health Organization (WHO) grade II.
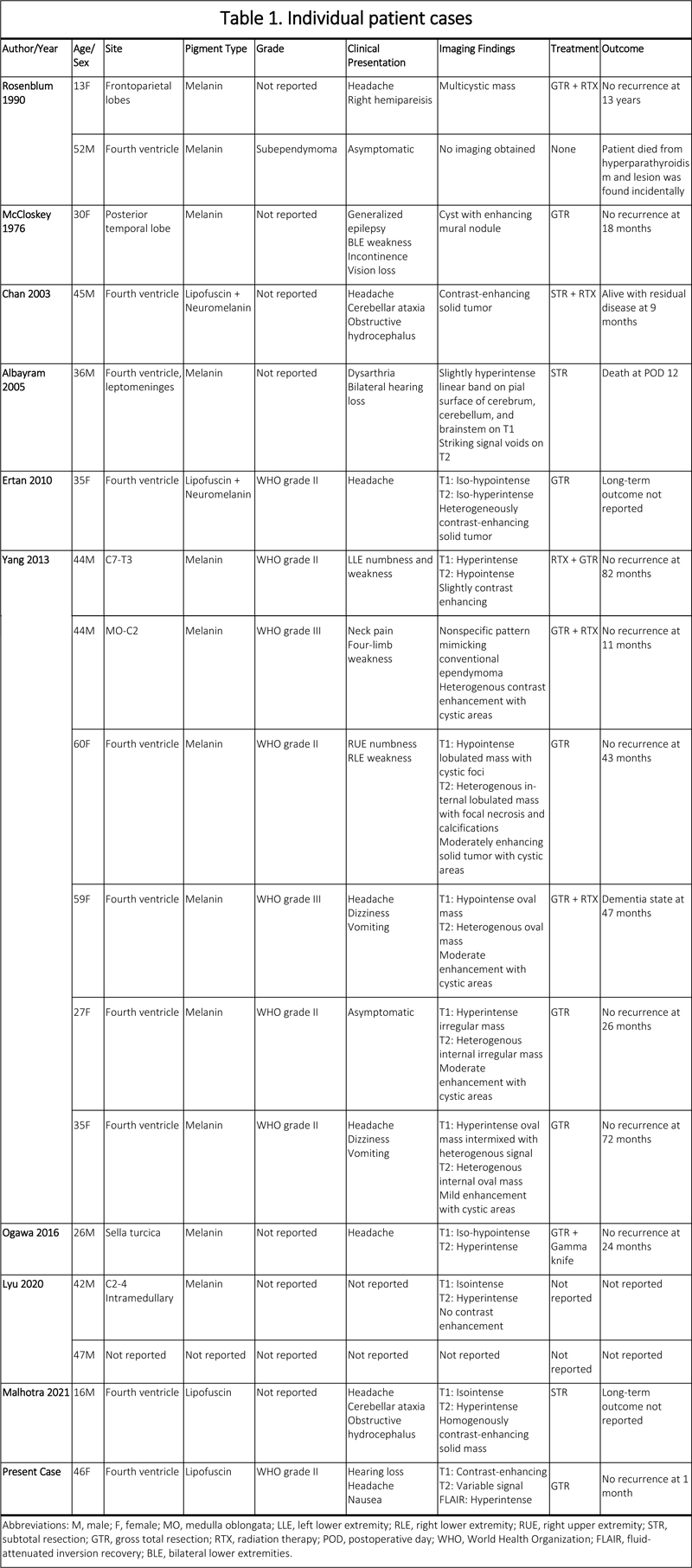
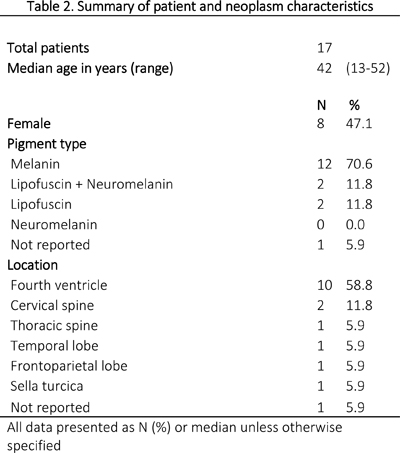
Figure 5. Methylation analysis results. A. Genome-wide copy number profile generated from DNA methylation array signal intensities. The copy number profile shows numeric whole chromosome changes, which are typical for EPN_PFB group. B. The UMAP embedding of DNA methylation array data for select tumor groups. Sample tumor embeds with EPN_PFB tumor cluster. Discussion Ependymomas are glial neoplasms with a slight male predominance that represent, approximately, 2-6% of all intracranial tumors and 50% of intramedullary spinal tumors.11,12 Much less common are pigmented ependymomas.2 These rare tumors may contain three types of pigment: melanin, neuromelanin, or lipofuscin.13 The most common pigment in pigmented ependymomas is melanin, a tyrosine derivative present in the choroid of the eye and, sometimes, in the meninges.13 Rarely, pigmented ependymomas contain neuromelanin, which is likely produced by nonenzymatic oxidation of dopamine or lipofuscin. Lipofuscin arises from iron-catalyzed peroxidation of membrane lipids and lipoproteins within lysosomes, and tends to accumulate with cellular aging.2,13 A recent case report and literature review on pigmented ependymomas describes only one previous case, in which lipofuscin was discovered to be the sole pigment contained within a pigmented ependymoma in a 16-year-old male.2 Here, we report on an additional case of lipofuscin-pigmented ependymoma of the fourth ventricle in a 46-year-old female with the EPN_PFB subtype. Given the rarity of this entity, a literature review was performed using the PubMed and Scopus search engines to identify previously described cases of pigmented ependymoma. Keywords used included “pigment”, “melanin”, “lipofuscin”, “neuromelanin” and “ependymoma”. This yielded 8 total studies2,8,9,14-19 reporting on 16 total patients with pathologically confirmed pigmented ependymoma (Table 1). Melanin was the most common pigment found in these ependymomas (n=12, 70.6%), followed by lipofuscin and neuromelanin (n=2, 11.8%) and lipofuscin alone (n=2, 11.8%). In one case, the pigment composition was not reported.16 Only two studies reported the tumor grade using the WHO classification.8,15 Six cases were WHO grade II, and two were WHO grade III anaplastic ependymoma according to the WHO schema at that time.
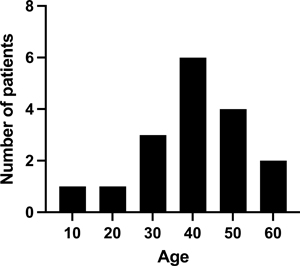
Pigmented ependymomas tend to occur in young adults, most commonly in the 4th ventricle, and present with symptoms caused by local mass effect. The primary treatment described was resection variably with adjuvant radiation therapy, and gross-total resection was reported in all but 5 cases (29.4%). The average age at time of diagnosis was 38.6 years and the median age was 42 years (range 13-52) (Fig. 6). There was a slight male predominance with 9 out of 17 male patients (52.9%). The most common location was the fourth ventricle (n=10, 58.8%), followed by the cervical spine (n=2, 11.8%), the thoracic spine, temporal lobe, frontoparietal lobe, and sella turcica (n=1, 5.9% each) (Table 2).
Figure 6. Histogram demonstrating age distribution of patients with pigmented ependymomas.
The primary clinical presentation was based on mass effect from the tumor location. Several patients with fourth ventricular tumors presented with symptoms of obstructive hydrocephalus (n=4). One patient was asymptomatic. Another developed right upper extremity numbness and right lower extremity weakness. Only one noteworthy case described a posterior fossa melanotic ependymoma complicated by secondary pial accumulation of melanin, resulting in dysarthria, hearing loss and death of the patient twelve days after subtotal resection.14 This was the only death reported in the literature and may be related to the secondary leptomeningeal pigment accumulation. The typical treatment for these tumors was attempted GTR, with adjuvant radiation therapy in six cases. There was one case where the patient was intact after resection, but developed hydrocephalus in the setting of adjuvant radiotherapy and devolved into a coma.8 In all other cases, the patients were alive without recurrence at last follow-up, with a mean follow up of 43.7 months. There are three distinct molecular variants of posterior fossa ependymoma, including posterior fossa group A ependymoma (EPN_PFA), EPN_PFB, and subependymoma, distinguished by their DNA methylation profile. Patients with EPN_PFB are typically adults, whereas EPN_PFA is more likely to be diagnosed in infants. Given the age of onset (adult) and typical lack of recurrence, we hypothesize that the methylation profiles of the posterior fossa pigmented ependymomas described in the literature are likely to be EPN_PFB in most cases. The molecular subgroup has been demonstrated to be a powerful independent predictor of outcomes.10 A recent study found that EPN_PFB was associated with an excellent 10-year overall survival (OS) rate of 96.1% after GTR, whereas EPN_PFA, the other posterior fossa variant, had worse outcomes; 5-year OS after GTR was 65.2% in females and 45.5% in males. Furthermore, EPN_PFA was a highly significant predictor of poor progression-free survival (hazard ratio [HR] 2.14; 95% confidence interval [CI] 1.31 to 3.49; p=0.002) and overall survival (HR 4.30; 95% CI 1.88 to 9.87; p<0.001) in this cohort.10 In addition to differences in methylation profile, EPN_PFA and EPN_PFB differ by protein expression of trimethylated histone H3K27 (H3K27me3).20,21 A study of 112 childhood ependymomas showed that 100% of EPN_PFA ependymomas had H3K27me3 loss defined as staining in less than 80% of cells.20 In contrast, only 1 out of 40 EPN_PFB ependymomas (2.5%) had less than 80% H3K27me3 immunopositivity.20 In a later study, two out of 15 EPN_PFB tumors (13.3%) showed H3K27me3 loss with immunopositivity in 10% and 60% of cells respectively.22 The specificity for EPN_PFB is 100%, but sensitivity is only 86.7% using the 80% immunopositivity cutoff.22 While all 29 EPN_PFA tumors showed H3K27me3 loss, the amount of “loss” was quite variable. A majority (62%) of EPN_PFA tumors showed H3K27me3 immunopositivity that ranged from 5-50%; another 38% of EPN_PFA tumors expressed H3K27me3 in less than 5% of cells.22 Our case, which demonstrated an estimated 70-80% H3K27me3 immunopositivity, is in the vicinity of the original 80% cutoff for EPN_PFB and is at a level of expression above that of most EPN_PFA tumors. The only previous case of ependymoma containing only lipofuscin pigment was reported by Malhotra et al. in 2021.2 They describe a fourth ventricular mass in a 16-year-old male that demonstrated perivascular pseudorosettes, ependymal canals, and tumor cells with plump cytoplasm filled with a greyish granular pigment and a high mitotic count (5 in 10 high-power fields in hotspots). Similar to the present case, the cells stained positively for PAS, but were negative for Fontana-Masson. In addition, the cells autofluoresced. Two 4th ventricle tumors demonstrated the presence of both lipofuscin and neuromelanin. The basis of the excessive intracellular lipofuscin accumulation is unclear. Ultimately, the prognostic significance of lipofuscin-pigmented ependymomas has yet to be determined given the small number of cases and limited long-term follow-up. Nonetheless, this literature review suggests a generally good prognosis in pigmented ependymoma, especially if GTR is achieved. Conclusion Here, we present an additional case of lipofuscin-pigmented ependymoma of the fourth ventricle and review the literature pertaining to these unique, uncommon neoplasms. Pigmented ependymomas occur most commonly in the 4th ventricle and in middle-aged patients, typically contain melanin, and seem to be associated with good long-term outcomes, especially when gross-total resec-tion is achieved. Secondary leptomeningeal melanin accumulations may portend a worse prognosis. Further study, molecular profiling, and long-term follow-up are required to better understand the natural history and recommended treatment for this rare central nervous system neoplasm. Acknowledgments We thank Dr. Jack Reid for assistance in creating whole slide digital images. References 1. Smith AB, Rushing EJ, Smirniotopoulos JG. Pigmented lesions of the central nervous system: radiologic-pathologic correlation. Radiographics. 2009;29(5): 1503-1524. https://doi.org/10.1148/rg.295095109. 2. Malhotra A, Rao S, Santhoshkumar R, Muralidharan N, Mitra S, Shetty S. Pigmented ependymoma of the fourth ventricle-a curious entity: report of a rare case with review of literature. International Journal of Surgical Pathology. 2021;29(1): 80-84. https://doi.org/10.1177/1066896920926700. 3. Vajtai I, Yonekawa Y, Schäuble B, Paulus W. Melanotic astrocytoma. Acta Neuropathol. 1996;91(5): 549-553. https://doi.org/10.1007/s004010050465. 4. Ng TH, Wong AY, Boadle R, Compton JS. Pigmented central neurocytoma: case report and literature review. The American Journal of Surgical Pathology. 1999;23(9): 1136-1140. https://doi.org/10.1097/00000478-199909000-00019. 5. Brown NJ, Wilson B, Lien BV, et al. Citation analysis of the most influential ependymoma research articles illustrates improved knowledge of the molecular biology of ependymoma. Neurosurgical Review. 2021;45: 1041-1088. https://doi.org/10.1007/s10143-021-01579-1. 6. Boström A, von Lehe M, Hartmann W, et al. Surgery for spinal cord ependymomas: outcome and prognostic factors. Neurosurgery. 2011;68(2): 302-308; discussion 309. https://doi.org/10.1227/NEU.0b013e3182004c1e. 7. Cage TA, Clark AJ, Aranda D, et al. A systematic review of treatment outcomes in pediatric patients with intracranial ependymomas. Journal of Neurosurgery: Pediatrics. 2013;11(6): 673-681. https://doi.org/10.3171/2013.2.Peds12345. 8. Yang C, Li G, Fang J, Wu L, Deng X, Xu Y. Clinical analysis of primary melanotic ependymoma in the central nervous system: case series and literature review. Acta Neurochirurgica. 2013;155(10): 1839-1847. https://doi.org/10.1007/s00701-013-1810-1. 9. Chan AC, Ho LC, Yip WW, Cheung FC. Pigmented ependymoma with lipofuscin and neuromelanin production. Archives of Pathology & Laboratory Medicine. 2003;127(7): 872-875. https://doi.org/10.5858/2003-127-872-pewlan. 10. Ramaswamy V, Hielscher T, Mack SC, et al. Therapeutic impact of cytoreductive surgery and irradiation of posterior fossa ependymoma in the molecular era: a retrospective multicohort analysis. Journal of Clinical Oncology. 2016;34(21): 2468-2477. https://doi.org/10.1200/jco.2015.65.7825. 11. Iwasaki Y, Hida K, Sawamura Y, Abe H. Spinal intramedullary ependymomas: surgical results and immunohistochemical analysis of tumour proliferation activity. British Journal of Neurosurgery. 2000;14(4): 331-336. https://doi.org/10.1080/026886900417315. 12. Rawlings CE, 3rd, Giangaspero F, Burger PC, Bullard DE. Ependymomas: a clinicopathologic study. Surgical Neurology. 1988;29(4): 271-281. https://doi.org/10.1016/0090-3019(88)90158-9. 13. Double KL, Dedov VN, Fedorow H, et al. The comparative biology of neuromelanin and lipofuscin in the human brain. Cellular and Molecular Life Sciences. 2008;65(11): 1669-1682. https://doi.org/10.1007/s00018-008-7581-9. 14. Albayram S, Urger E, Oz B, Kafadar A, Islak C, Kocer N. MR imaging of pial melanosis secondary to a posterior fossa melanotic ependymoma. American Journal of Neuroradiology. 2005;26(4): 804-808. https://doi.org/15814924. 15. Ertan Y, Sarsik B, Ozgiray E, Kitis O, Dalbasti T, Akalin T. Pigmented ependymoma with signet-ring cells and Rosenthal fibers: a rare variant of ependymoma. Neuropathology. 2010;30(1): 71-75. https://doi.org/10.1111/j.1440-1789.2009.01031.x. 16. Lyu L, Zou L, Jiang Y, et al. Clinical characteristics and treatment outcomes of pigmented tumors in central nervous system: focusing on melanocytic tumors. Journal of Clinical Neuroscience. 2020;81: 83-89. https://doi.org/10.1016/j.jocn.2020.09.009. 17. McCloskey JJ, Parker JC, Jr., Brooks WH, Blacker HM. Melanin as a component of cerebral gliomas: the melanotic cerebral ependymoma. Cancer. 1976;37(5): 2373-2379. https://doi.org/10.1002/1097-0142(197605)37:5<2373::aid-cncr2820370529>>3.0.co;2-2 18. Ogawa Y, Watanabe M, Jokura H, Tominaga T. Primary intrasellar melanotic ependymoma successfully treated by combined transsphenoidal and gamma knife surgeries. International Journal of Clinical and Experimental Medicine. 2016;9 (1): 371-375. 19. Rosenblum MK, Erlandson RA, Aleksic SN, Budzilovich GN. Melanotic ependymoma and subependymoma. The American Journal of Surgical Pathology. 1990;14(8): 729-736. https://doi.org/10.1097/00000478-199008000-00005. 20. Panwalkar P, Clark J, Ramaswamy V, et al. Immunohistochemical analysis of H3K27me3 demonstrates global reduction in group-A childhood posterior fossa ependymoma and is a powerful predictor of outcome. Acta Neuropathologica. 2017;134(5): 705-714. https://doi.org/10.1007/s00401-017-1752-4. 21. Bayliss J, Mukherjee P, Lu C, et al. Lowered H3K27me3 and DNA hypomethylation define poorly prognostic pediatric posterior fossa ependymomas. Science Translational Medicine. 2016;8(366): 366ra161. https://doi.org/10.1126/scitranslmed.aah6904. 22. Fukuoka K, Kanemura Y, Shofuda T, et al. Significance of molecular classification of ependymomas: C11orf95-RELA fusion-negative supratentorial ependymomas are a heterogeneous group of tumors. Acta Neuropathologica Communications. 2018;6(1): 134. https://doi.org/10.1186/s40478-018-0630-1.
Copyright: © 2022 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |