|
|
|
Free Neuropathology 3:5 (2022) |
|
Review |
|
Neuromuscular disease: 2022 update |
|
Marta Margeta1 |
|
1 Department of Pathology, University of California, San Francisco, CA, USA |
|
Address for correspondence: |
|
Submitted: 16 February 2022 Accepted: 02 March 2022 Copyedited by: Henry Robbert Published: 04 March 2022 |
|
Keywords: COVID-19, Guillain-Barré syndrome, MLIP, VWA1, Optic neuropathy, Autophagy, Peripheral neuropathy, Systemic sclerosis, Microvessels, Idiopathic inflammatory myopathy, Gene expression profiling, Pompe disease |
|
Abstract This review highlights ten important advances in the neuromuscular disease field that were reported in 2021. As with prior updates in this article series, the overarching topics include (i) advances in understanding of fundamental neuromuscular biology; (ii) new / emerging diseases; (iii) advances in understanding of disease etiology and pathogenesis; (iii) diagnostic advances; and (iv) therapeutic advances. Within this general framework, the individual disease entities that are discussed in more detail include neuromuscular complications of COVID-19 (another look at the topic first covered in the 2021 review), autosomal recessive myopathy caused by MLIP mutations, autosomal recessive neuromuscular disease caused by VWA1 mutations, Leber’s hereditary optic neuropathy, myopathies with autophagic defects, tRNA synthetase-associated Charcot-Marie-Tooth disease, systemic sclerosis-associated myopathy, humoral immune endoneurial microvasculopathy, and late-onset Pompe disease. In addition, the review highlights a few other advances (including new insights into mechanisms of muscle and nerve regeneration and the use of gene expression profiling to better characterize different subtypes of immune-mediated myopathies) that will be of significant interest for clinicians and researchers who specialize in neuromuscular disease. Abbreviations ARS - aminoacyl-tRNA synthetase, ASS - anti-synthetase syndrome, ASSM - anti-synthetase syndrome-associated myositis, AVM - autophagic vacuolar myopathy, CASA - chaperone-assisted selective autophagy, COVID-19 - Coronavirus disease 2019, CK - creatine kinase, CMT - Charcot-Marie-Tooth disease, DM - dermatomyositis, ERT - enzyme replacement therapy, GAA - acid α-glucosidase, GBS - Guillain-Barré syndrome, HIEM - humoral immune endoneurial microvasculopathy, HMGCR - 3-hydroxy-3-methylglutaryl-CoA reductase, IIM - idiopathic inflammatory myopathy, IMNM - immune-mediated necrotizing myopathy, ISR - integrated stress response, LHON - Leber’s hereditary optic neuropathy, LOPD - late-onset Pompe disease, M6P - mannose-6-phosphate, MCT1 - monocarboxylate transporter 1, MLIP - muscular A-type lamin-interacting protein, MMCP - minimal myositis with capillary pathology, MSA - myositis specific antibody, MSP - multiple system proteinopathy, MuSC - muscle stem cells, MxA - Myxovirus (Influenza Virus) Resistance 1, Interferon-Inducible Protein P78, Nampta - nicotinamide phosphoribosyl transferase a, NMD - neuromuscular disease, sIBM - sporadic inclusion body myositis, SSc - systemic sclerosis, VWA1 - von Willebrand factor A containing 1 protein.
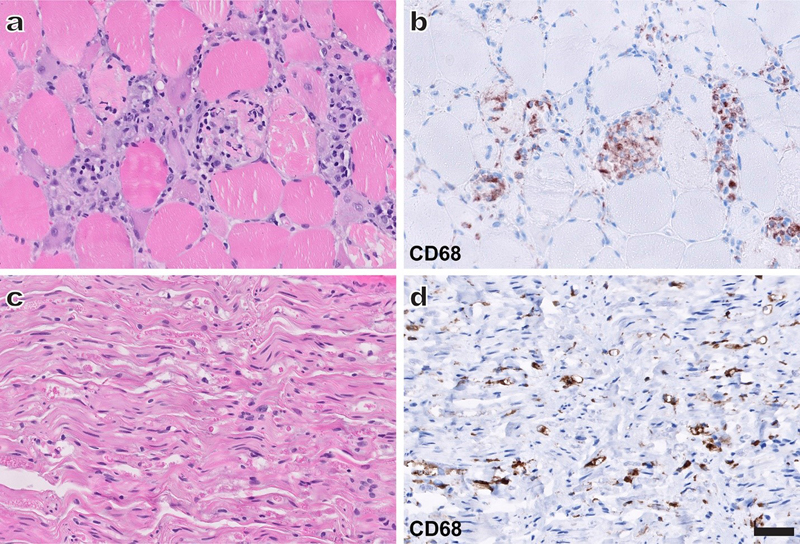
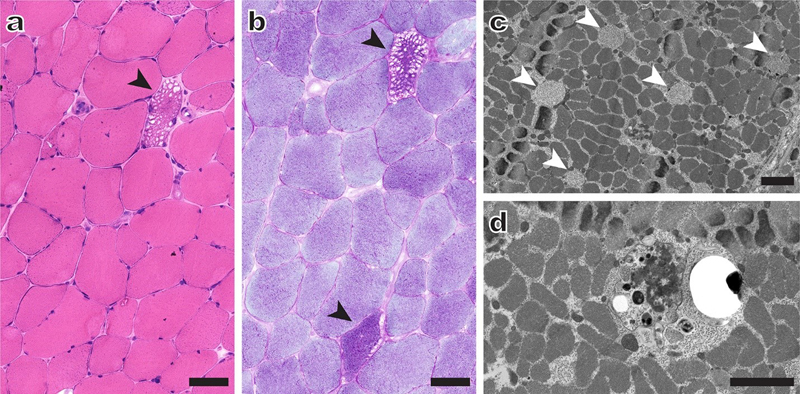
In this annual update, I will briefly describe ten neuromuscular field advances from last year that I consider to be most important and/or interesting; as in the earlier updates (Margeta, 2020b, 2021), these advances will be grouped into different “discovery clusters” and listed in no particular order. ADVANCES IN FUNDAMENTAL NEUROMUSCULAR BIOLOGY WITH IMPLICATIONS FOR NEUROMUSCULAR DISEASE 1. Revisiting the role of macrophages in nerve and muscle regeneration In the last year’s review (Margeta, 2021), I highlighted the 2020 discovery of a crosstalk between macrophages and satellite cells in skeletal muscle repair. Excitingly, two studies published in 2021 extended that work by further dissecting the molecular mechanisms by which macrophages promote regeneration not only in skeletal muscle (Ratnayake et al., 2021) but also in peripheral nerves (Jha et al., 2021). Together with other recent work in the field of regenerative medicine, these two studies provide evidence that macrophages – which are readily detectable within necrotic muscle fibers (Fig. 1a-b) and adjacent to degenerating peripheral nerve axons (Fig. 1c-d) – play a major role in the PNS repair, extending well beyond the long-recognized phagocytic clearance of necrotic cellular debris at injury sites.
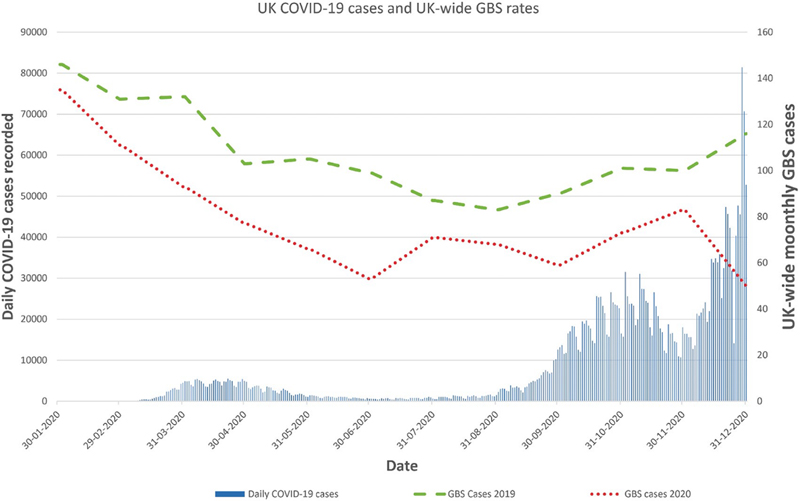
Figure 1. Macrophages home on degenerating muscle and nerve fibers. A representative field from an H&E-stained muscle section (a) shows muscle fibers in varying stages of necrosis and repair, starting with early coagulative necrosis, progressing through myophagocytosis, and ending with regeneration mediated by macrophage-activated satellite cells; in this case, the fiber injury was immune-mediated, but similar changes are seen in all necrotizing myopathies regardless of the underlying etiology. The CD68 stain of the same area (b) highlights macrophages within necrotic muscle fiber segments (myophagocytosis). A representative field from an H&E-stained peripheral nerve section (c) shows a marked loss of large myelinated axons and abundant digestion chambers (fragments of degenerating axons) in a case of acute axonal neuropathy. The CD68 stain of the same microscopic field (d) highlights endoneurial macrophages associated with degenerating axon fragments. The stains were performed on formalin-fixed, paraffin-embedded tissue; scale bar, 50 μm. Ratnayake and colleagues used sophisticated genetic and pharmacologic approaches to delineate the macrophage-stem cell interactions that are required for muscle wound repair in both zebrafish and mice (Ratnayake et al., 2021). Using the zebrafish laser-ablation injury model, they showed that a subset of tissue-resident macrophages that are recruited to the wound following injury remained at the injury site, creating a “dwelling” macrophage population that had spherical morphology (in contrast to transient macrophages, which had a stellate appearance); these dwelling macrophages formed intimate connections with muscle stem cells (MuSC) that were reminiscent of dendritic cell-T cell immunological synapses, forming a transient pro-proliferative stem cell niche that persisted until MuSC underwent cell division. Based on their gene expression profiles, dwelling macrophages were shown to be a heterogenous cell population; however, the authors identified a single “mature” subpopulation (defined by expression of markers associated with the anti-inflammatory macrophage phenotype, such as arginase 2 and matrix metalloproteinase-9) that mediated muscle repair by stimulating MuSC proliferation. To promote MuSC mitogenesis, these mature dwelling macrophages (which constitute ~70% of all dwelling macrophages) secreted nicotinamide phosphoribosyl transferase a (Nampta), which bound to the chemokine receptor CCR5 expressed by MuSC; interestingly, this mitogenic effect of Nampta was independent of its enzymatic activity. The zebrafish findings were replicated in mice using the volumetric muscle loss model, which simulates irrecoverable muscle injury that occurs following trauma, tumor excision, or infarction (Quarta et al., 2017; Sicari et al., 2012): delivery of human recombinant NAMPT (the human analogue of zebrafish Nampta) into the excisional muscle defect using a fibrin hydrogel led to a complete restoration of muscle architecture, with an increase in the number of proliferating satellite cells and centrally nucleated, regenerating muscle fibers relative to the control condition (fibrin hydrogel without NAMPT). While these results are very promising from the tissue engineering standpoint, it remains to be seen whether a similar approach can be used to promote muscle fiber regeneration in muscle dystrophies and other muscle diseases that show a significant loss of muscle volume. The study by Jha and colleagues (Jha et al., 2021) focused on the role of macrophage metabolism in the peripheral nerve repair following mechanical injury, and their nerve regeneration findings in many ways echo the muscle regeneration findings made by Ratnayake et al. Using the murine sciatic nerve crush model of Wallerian degeneration, Jha et al. showed that the activity of monocarboxylate transporter 1 (MCT1, encoded by SLC16A1 gene) in macrophages, but not in dorsal root ganglion neurons, Schwann cells, or perineurial cells, plays a key role in axon regeneration. Selective deletion of MCT1 from macrophages did not affect macrophage recruitment to the portion of the nerve distal to the site of injury; instead, it impaired the ability of recruited macrophages to phagocytose axon and myelin debris. In addition, MCT1 deletion led to a decrease in the expression of macrophage transcription factor ATF3, thereby attenuating macrophage reprogramming into a pro-regenerative, anti-inflammatory phenotype characterized by high expression of arginase 1 and chitinase-like 3. Excitingly, the authors also showed that i.v. treatment with bone marrow-derived wt macrophages fully restored peripheral nerve regeneration in mice with macrophage-selective MCT1 deletion, while macrophage-specific MCT1 upregulation led to improved nerve regeneration. Taken together, these findings suggest that adoptive transfer of patient-derived macrophages engineered to upregulate their MCT1 activity could be used to treat severe peripheral nerve injuries. However, this study has one very significant caveat: while both anti-regenerative and pro-regenerative effects of various experimental manipulations could be demonstrated on the tissue level (by quantifying regenerating axon clusters, relative thickness of axon myelin sheaths, and the number and distribution of neuromuscular junctions in the gastrocnemius muscle), they were not accompanied by parallel measures of behavioral recovery. One possible explanation for this discrepancy is that behavioral recovery actually preceded tissue recovery in this mouse model, suggesting that alternate recovery / behavioral compensation pathways are important, at least in rodents; nonetheless, this animal model discrepancy needs to be resolved before exploring the efficacy of macrophage-based therapies for human axonal neuropathies. NEWLY DEFINED / EMERGING NEUROMUSCULAR DISEASES 2. Neuromuscular complications of COVID-19: What have we learned after one more year of the pandemic? COVID-19, the novel infectious disease caused by SARS-CoV-2, primarily targets the respiratory system but can also affect many other tissues and organs, including the PNS. In the last year’s review (Margeta, 2021), I summarized what was known about the neuromuscular complications of COVID-19 at the end of 2020; given the preliminary nature of those investigations, I decided to revisit this topic in the current review, providing an update on what has been learned since then. One area of intense interest within the neuromuscular field has been the possible link between COVID-19 and Guillain-Barré syndrome (GBS), an acute immune-mediated polyneuropathy characterized by ascending weakness, mild-moderate sensory abnormalities, and pain. Most GBS cases are triggered by a bacterial or viral infection that precedes neurologic symptoms by 1-3 weeks; the strongest association is seen with Campylobacter jejuni bacterium (~100 GBS cases / 100 000 C. jejuni infections) and with Zika virus (~50 GBS cases / 100 000 Zika virus infections). While small early studies from Italy and Spain suggested that GBS could also be triggered by a preceding SARS-CoV-2 infection (Filosto et al., 2021; Fragiel et al., 2021), no such link was found in a more comprehensive epidemiologic study performed in the UK (Keddie et al., 2021) [for a more detailed discussion of the 2020 data, see the last year’s review (Margeta, 2021)]. Discrepancies between these initial studies prompted animated discussion among the GBS experts, but also led to additional investigations undertaken by several different groups; taken as a whole, this new evidence provides further support for a lack of a strong link between COVID-19 and GBS. For example, the data originally reported by Keddie at al. reflected the first UK COVID-19 surge (in March and April 2020); extension of the same study until the end of 2020 showed essentially the same findings, with a large increase in the number of COVID-19 cases in the fall of 2020 that was accompanied by a decrease, rather than an increase, in the number of GBS cases during the same time period [(Lunn et al., 2021) and Fig. 2]. Moreover, as reported by the same group of investigators in a very recently published medRχiv preprint (Keh et al., 2022), this disassociation between COVID-19 and GBS numbers has persisted into 2021, with a clear uptick in GBS cases observed in March and April of 2021 (secondary to COVID-19 vaccination; further discussed below), but no similar increase was seen in August and September of 2021, during the delta variant-associated COVID-19 surge. (No data is yet available for the most recent COVID-19 surge caused by the omicron variant of SARS-CoV-2.) A similar lack of association between COVID-19 and GBS was observed by a team of investigators in Singapore (Umapathi et al., 2021). In contrast, a weak association between SARS-CoV-2 infection and GBS (1.5 excess GBS cases per 100 000 SARS-CoV-2-positive tests) was reported by a different group of UK investigators (Patone et al., 2021); however, that study was based on the hospital coding data, which are not always entirely accurate, and included GBS cases that were diagnosed on the same day as COVID-19 (suggesting a coincidental rather than causative relationship). Finally, no excess GBS cases were observed by researchers of the International GBS Outcome Study consortium, which includes GBS experts from China and Japan in addition to several European countries. While this study was not designed for systematic GBS surveillance, a significant increase in the GBS case incidence should have led to an observable increase in the study inclusion rate; instead, the inclusion rate in the first 5 months of 2020 was comparable to inclusion rates in 2017, 2018 and 2019 (Luijten et al., 2021). Taken together, the preponderance of data available to date suggests that a preceding SARS-CoV-2 infection is not a major risk factor for development of GBS; however, it remains possible that rare GBS cases could be triggered by infection with this virus.
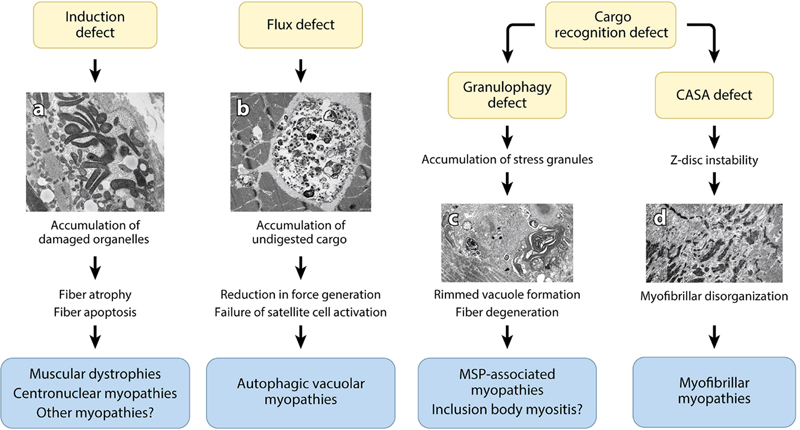
Figure 2. Daily UK infections with COVID-19 by PCR (blue bars) and monthly cases of GBS. 2020 = red dotted line, 2019 = green dashed line, secondary y-axis. The graphs demonstrate no visible increase in GBS in the last quarter of 2020 with a rise in case numbers between 30% and 1000% more than in March/April. Note significant alterations in testing occurred in the UK in April 2020 resulting in the subsequent enhanced detection of most symptomatic cases. Hospital admissions were 30% higher on 1 January 2021 than in April 2020. Sources: COVID cases (left axis, blue bars) https://coronavirus.data.gov.uk/details/cases; NHSE National Immunoglobulin Database courtesy MDSAS, Manchester, UK. [With publisher’s permission, this figure and its legend are reproduced from (Lunn et al., 2021).] In contrast to a lack of definite association between GBS and COVID-19, there is a clear link between GBS and the first dose of the ChAdOx1 nCoV-19 (AstraZeneca) adenoviral COVID-19 vaccine, with an excess risk of ~0.4-0.6 GBS cases for each 100 000 administered vaccine doses (Keh et al., 2022; Patone et al., 2021). Interestingly, a similar excess GBS risk was seen in the US during the 1976-77 flu vaccination campaign, with 0.5-0.6 GBS cases observed for each 100 000 doses of the “swine flu” vaccine given that year; the risk attributable to later influenza vaccines has been significantly lower (~0.1 GBS cases for each 100 000 vaccines), and no increase in the GBS risk has been observed with the mRNA-based COVID vaccines, BNT162b2/tozinameran (Pfizer) and mRNA-1273 (Moderna). Given that all these COVID-19 vaccines target the spike protein of SARS-CoV-2, the differences among them suggest that the excess GBS risk is attributable to the adenoviral vector rather than the SARS-CoV-2 spike protein antigen; supporting this hypothesis, a warning about a link between the adenovirus-based Ad26.COV2.S (J&J) COVID-19 vaccine and GBS was announced by the US Food and Drug Administration in July 2021 (https://fda.gov/news-events/press-announcements/coronavirus-covid-19-update-july-13-2021), although no formal scientific study about this association has been published to date. What about COVID-19-associated myopathy? Although initial studies were extremely limited, they suggested that weakness and high creatine kinase (CK) levels seen in a significant subset of COVID-19 patients were immune-mediated rather than due to direct viral infection of skeletal muscle [reviewed in (Margeta, 2021)]. Based on the two large autopsy case-control studies published since then (Aschman et al., 2021; Suh et al., 2021), this initial impression was essentially correct. Aschman and colleagues examined deltoid and quadriceps muscles from 43 patients with COVID-19 and compared them to the same muscles sampled from 11 severely ill patients negative for SARS-CoV-2. They found that ~60% of patients who died with severe COVID-19 showed evidence of immune-mediated muscle pathology including some combination of mild-severe inflammation (mostly consisting of CD8+ T cells and macrophages), degenerating muscle fibers, and MHC-I and MHC-II upregulation in muscle fiber sarcolemma (the latter mostly seen in chronic cases). Three samples showed perifascicular upregulation of MHC-I and MHC-II; however, no sarcoplasmic upregulation of dermatomyositis (DM) marker MxA [Myxovirus (Influenza Virus) Resistance 1, Interferon-Inducible Protein P78; also known as Mx1] was seen in any of the specimens. (Interestingly, some COVID-19 samples showed increased MxA expression in the endomysial capillaries, possibly reflecting a nonspecific response to systemic viral infection.) In addition, a few COVID-19 samples showed evidence of small and medium-vessel angiitis. Although SARS-CoV-2 RNA was detectable by PCR in some muscle homogenates, immunohistochemistry against SARS-CoV-2 spike protein was negative in all cases and no viral particles were demonstrated on electron microscopy (Aschman et al., 2021). Very similar findings were reported by Suh et al., who studied psoas muscles from 35 patients who died following COVID-19 infection and 10 severely ill patients who were COVID-19-negative. In addition to diffuse type 2 fiber atrophy (which was present in almost all cases and controls), these authors found evidence of immune-mediated muscle pathology in ~70% of COVID-19 cases, with necrotizing myopathy in 9 patients, T cell- and macrophage-mediated myositis in 8 patients, and isolated diffuse or multifocal MHC-I upregulation in additional 8 patients. Like Aschman et al., Suh et al. observed perifascicular pattern of MHC-I upregulation without concurrent sarcolemmal MxA upregulation in one COVID-19 case, while MxA expression restricted to endomysial capillaries was seen in 8 COVID-19 cases. Immunohistochemistry against SARS-CoV-2 nucleocapsid protein was negative in all 35 COVID-19 cases. In contrast to the findings in these autopsy studies, direct viral infection of muscle fibers was recently documented by both immunohistochemistry and electron microscopy in muscle biopsies from two of three COVID-19 patients with critical illness myopathy and persistent SARS-CoV-2 positivity on PCR testing (Dodig et al., 2022). It is currently unclear what accounts for the discrepancy between these three studies; one possibility is that the difference reflects the sample type used (muscle biopsy vs. autopsy), although that does not seem likely given (1) that SARS-CoV-2 viral infection can be demonstrated by both immunohistochemistry and electron microscopy in the lungs of autopsied COVID-19 patients and (2) that no SARS-CoV-2 was definitively detected in other muscle biopsies from COVID-19 patients reported to date. More likely, this difference can be attributed to the effects of a long-standing and persistent SARS-CoV-2 infection, which was documented in the patients described by Dodig et al. but is not a common feature of COVID-19. Importantly, and regardless of the specific reason for the rarity of this finding, the study by Dodig and coauthors demonstrates that direct SARS-CoV-2 infection of skeletal muscle can occur, and raises the possibility that such infection is present in the early stages of COVID-19 in many patients, acting as a trigger for the subsequent immune-mediated muscle pathology that develops in some instances. 3. Autosomal recessive myopathy caused by truncating mutations of MLIP (muscular A-type lamin-interacting protein) Unexplained persistent elevation of serum CK levels points to a chronic myopathic process that is likely genetic in origin, but identifying the specific underlying etiology can be challenging if no other symptoms and signs are present to narrow the differential diagnosis. When chronic hyperCKemia is associated with exercise intolerance and exercise-induced rhabdomyolysis, the underlying problem is usually metabolic; if, on the other hand, chronic CK elevation is accompanied by muscle weakness and wasting, the patient likely has a muscular dystrophy. Two interesting papers published in 2021 (Lopes Abath Neto et al., 2021; Salzer-Sheelo et al., 2021) uncovered a novel autosomal recessive myopathy that is caused by loss-of-function mutations in MLIP (muscular A-type lamin-interacting protein; also known as muscular LMNA-interacting protein) and is clinically characterized by persistent basal hyperCKemia. Among the twelve affected individuals identified to date, eight developed symptoms in childhood (with symptom onset between 8 months and 7 years of age); their clinical findings included exertional myalgia, episodes of rhabdomyolysis (occasionally exercise-induced, but without clear trigger in most cases), and/or mild progressive proximal muscle weakness in addition to chronically elevated CK levels. The remaining four individuals were identified based on genetic screening of the subject cohort enrolled in the University of Maryland study of Old Order Amish; based on the evaluation of banked serum specimens (available for 3 of 4 individuals), those patients, who currently range from 24 to 67 years in age, also have chronic hyperCKemia, but no other known neuromuscular symptoms. Muscle biopsies were performed for 7 of 8 clinically affected patients and showed a wide spectrum of histopathologic findings, ranging from mild nonspecific features to necrotizing and – less frequently – dystrophic changes. Thus, it is not yet entirely clear whether to classify this new disease as a metabolic myopathy or a muscular dystrophy; while muscular dystrophy is more likely, the final classification will require careful clinical follow-up and repeat muscle biopsies of the known symptomatic individuals (who currently range from 5-19 years of age), as well as identification of additional patients by genetic testing of individuals with otherwise unexplained chronic hyperCKemia. MLIP is a ubiquitously expressed, alternatively spliced protein (23-57 kDa) that directly interacts with lamins A/C (two intermediate filaments, both derived from the LMNA gene, that are the main constituents of the nuclear envelope); its expression is highest in the heart, skeletal muscle, and brain, but its function remains poorly understood (Ahmady et al., 2011). In a murine model, MLIP deletion in the heart led to metabolic abnormalities, abnormal adaptation to stress, and accelerated progression from compensated cardiac hypertrophy to decompensated heart failure (Cattin et al., 2015; Huang et al., 2015). In contrast, MLIP deletion in murine skeletal muscle led to increased central nucleation but no obvious neuromuscular phenotype (Liu et al., 2020). In humans, variants in the MLIP genetic locus [a single coding missense variant (NM_138569, c.475G>A, p.Val159Ile) and several noncoding variants] have been shown to increase the risk of dilated cardiomyopathy (Esslinger et al., 2017); however, prior to studies by Lopes Abath Neto et al. and Salzer-Sheelo et al., it was not known whether MLIP mutations can directly cause human disease. Twelve affected individuals from 8 unrelated families that are described in these two studies all carry either homozygous or heterozygous biallelic truncating mutations of MLIP gene, with mutation hotspots in exons 4 and exons 9; while the molecular consequences of these mutations still need to be fully elucidated, initial work suggests that they lead to nonsense-mediated mRNA decay and presumed loss of protein expression [although the latter is likely specific for individual splice variants and has therefore been difficult to establish (Lopes Abath Neto et al., 2021)]. Interestingly, 1 of 8 affected children and all 4 affected adults with biallelic MLIP mutations showed evidence of mild cardiac involvement, raising the possibility that MLIP deficiency causes cardiac abnormalities in humans as well as mice; this is particularly intriguing given the broad spectrum of human disease associated with LMNA mutations, which includes cardiomyopathy in addition to muscular dystrophy, peripheral neuropathy, lipodystrophy, and premature aging (Ho and Hegele, 2019). Future work will be required to fully define the nature and scope of skeletal and cardiac muscle phenotypes caused by MLIP deficiency and to elucidate whether MLIP interaction with lamins A/C plays an important role in the pathogenesis of this new human disease. 4. Autosomal recessive neuromuscular disease caused by mutations in VWA1 (von Willebrand factor A containing 1 protein) In the past, a disease was typically defined based on its unique clinicopathologic features, with the underlying etiology and pathogenesis established later. In the era of comprehensive genetic testing, this traditional sequence is being inverted: new genetic diseases are identified and defined based on their etiology, and future work is required to fully define their clinicopathologic features. As with the MLIP-associated recessive myopathy described in discovery #2, two different research groups (Deschauer et al., 2021; Pagnamenta et al., 2021) used a genetic approach to identify a novel autosomal recessive neuromyopathy caused by mutations in VWA1 (von Willebrand factor A containing 1 protein), also known as WARP (von Willebrand factor A domain-related protein). Deschauer et al. started their study in a more “conventional” manner, by performing exome sequencing of 10 individuals with presumed genetic neuromuscular disease but without genetic diagnosis; 2 of these 10 patients turned out to carry biallelic truncating mutations in VWA1, a gene not previously associated with human disease but with high expression in peripheral nerve and skeletal muscle tissues. Follow-up analyses of the patients’ families and additional “unsolved” patient cohorts identified 13 additional individuals with biallelic VWA1 mutations; 5 of 6 identified mutations are predicted to result in protein truncation, and all 6 are predicted to result in a loss of protein function. Pagnamanta et al. used a slightly different approach: they identified VWA1 as a potentially interesting gene based on its high expression in the PNS and searched the data from the 100K Genome Project (Turnbull et al., 2018) for individuals carrying biallelic VWA1 variants. This analysis ultimately yielded 10 unrelated patients that fit the inclusion criteria, with 7 additional individuals identified through follow-up studies of other patient cohorts. Interestingly, 15 of these 17 patients (from 14 of 15 separate families) carry the same truncating VWA1 mutation (10-bp insertion, NM_022834, c.62_71dup; pGly25ArgfsTer74) in either homozygous or heterozygous state; this mutation was also identified in 3 of 6 families described by Deschauer et al., and is estimated by Pagnamanta et al. to have arisen in Europe ~8000 years ago. Interestingly, the same 10-bp tandem repeat is deleted (rather than duplicated) in other affected individuals, suggesting that it is prone to de novo alterations. What is the clinicopathologic phenotype of the VWA1-associated neuromuscular disease? The affected individuals typically develop slowly progressive non-length dependent axonal motor neuropathy that presents with distal weakness and foot deformities, often in early childhood; however, proximal weakness with scapular winging and mildly elevated CK level is sometimes also present, and it is not entirely clear whether this myopathic involvement represents a separate phenotype of VWA1 deficiency, or whether myopathic changes are secondary to the primary neuropathic process. Muscle biopsies were evaluated for a subset of cases (7 of 32 patients across both studies had biopsies that were available for review), showing a similarly complex picture: well-developed chronic neurogenic changes were accompanied by some myopathic features (including fiber size variation, internal nucleation, endomysial fibrosis, fiber lobulation and/or whirling, and mitochondrial alterations) but no basement membrane abnormalities. VWA1 is a 445 aa extracellular matrix protein that contains the N-terminal von Willebrand factor A domain followed by two fibronectin type III repeats; it is expressed in the cartilage and in the basement membranes of peripheral nerves (endoneurium), skeletal muscle (endomysium), and the CNS vasculature, where it interacts with collagen VI and perlecan (two proteins that are also associated with genetic NMD) (Allen et al., 2009). VWA1-null mice show a delayed response to painful stimuli and impairment of fine motor coordination; histologically, their peripheral nerves show aberrant fusion of Schwann cell basement membranes, while their skeletal muscles and other VWA1-expressing tissues show no obvious abnormalities (Allen et al., 2009). Knockdown of zebrafish vwa1 gene (zebrafish VWA1 analogue) leads to dose-dependent abnormalities of motor neuron development, with reduced axon branching of primary motor neurons, axon truncation of secondary motor neurons, and reduced number of neuromuscular junctions, as well as some muscle fiber disorganization (Pagnamenta et al., 2021). Taking together the human and animal model data, it is clear that VWA1-deficiency affects motor neuron axons and leads to neuropathic changes in the affected musculature; however, it remains to be established whether these abnormalities represent a developmental or degenerative disease, and whether there is a separate but concurrent myopathic phenotype. In addition, it needs to be elucidated how the subtle basement membrane abnormalities lead to these neuromuscular phenotypes. ADVANCES IN UNDERSTANDING OF ETIOLOGY AND PATHOGENESIS OF NEUROMUSCULAR DISEASES 5. Impaired repair of mitochondrial respiratory chain complex 1 causes autosomal recessive variant of Leber’s hereditary optic neuropathy Leber’s hereditary optic neuropathy (LHON), first defined as a clinical entity in 1871, is a degenerative disease of retinal ganglion cells and their axons that presents with subacute bilateral painless loss of central vision. Most LHON cases are maternally inherited; three point mutations in mitochondrial DNA (mtDNA), each of which alters the coding sequence of a different subunit of mitochondrial respiratory chain complex I, account for ~90% of the maternally inherited cases, with other mtDNA mutations accounting for additional ~5%. However, approximately 5% of LHON patients carries no pathogenic mtDNA mutations; in their groundbreaking work published last year, Stenton et al. showed that many of these previously unresolved LHON cases carry biallelic missense mutations in the gene encoding DNAJC30 chaperone (Stenton et al., 2021). Among 33 individuals with DNAJC30-mutated, autosomal recessive form of LHON (arLHON) characterized by Stenton and colleagues, 29 carry the same missense mutation (NM-032317, c152A>G, pTyr51Cys; estimated to have arisen in Eastern Europe ~85 generations / ~2100 years ago); 2 additional missense DNAJC30 mutations were identified in the remaining 4 patients. Clinically, arLHON cases are indistinguishable from mtLHON cases, although arLHON has a significantly earlier age of onset (19.9+/-7.9 vs. 30.7+/-15.0 years). Like mtLHON, arLHON is characterized by incomplete disease penetrance, with some homozygous mutation carriers not expressing the clinical phenotype. Interestingly, mutation penetrance is sex-dependent in both mitochondrial and autosomal recessive forms of LHON, with disease prevalence 5-10 times higher in male compared to female mutation carriers; both incomplete penetrance and male predominance are unusual for an autosomal recessive disease, and the mechanism(s) underlying these phenomena are yet to be elucidated. Importantly, arLHON patients have a better response to treatment with idebenone [a coenzyme Q10 analogue that bypasses complex I and is currently approved for LHON treatment in Europe (Amore et al., 2021)] than mtLHON patients; this difference in the treatment response highlights the clinical significance of early molecular diagnosis of arLHON cases. Notably, these genetic and clinical findings were replicated by another very recent study (Kieninger et al., 2022), which also identified two additional DNAJC30 pathogenic variants. How do DNAJC30 mutations cause LHON? All three initially identified variants are located in the J domain, a conserved portion of DNAJC30 with homology to the heat shock family of proteins. Muscle biopsies from arLHON patients showed a small but significant defect in complex I activity (but no change in complex IV and complex V activities), and this complex I-specific defect was recapitulated in patient-derived fibroblast cell lines and DNAJC30-knockout HEK293 cells. Interestingly, the functional defect of complex I was accompanied by a small but consistent increase (rather than decrease) in the expression level of complex I subunits, with no corresponding increase in the level of mRNAs that encode these subunits. The increase in the complex I subunit expression level was accompanied by a decrease in the turnover of subunits that comprise the N-module, which normally have the highest turnover rate due to a high degree of oxidative damage (Szczepanowska et al., 2020). Taken together, these data indicate that DNAJC30 maintains structure and function of complex I by facilitating exchange of oxidatively damaged subunits comprising its N-module; impairment of this repair mechanism leads to accumulation of damaged type I complexes, functional complex I defect, and LHON clinical phenotype. Interestingly, DNAJC30 was also shown to interact with several subunits of complex V / ATP-synthase (Tebbenkamp et al., 2018); however, clinical significance of that finding is unclear given that muscle biopsies from patients with DNAJC30 mutations show no changes in complex V abundance and no functional complex V deficits. It is worth noting that complex I dysfunction is thought to play an important role in the pathogenesis of Parkinson disease, cancer, and diabetes; a long-term clinical follow up of arLHON patients will be necessary to determine whether they are at increased risk for these common age-associated disorders. 6. Autophagy defects in skeletal myopathies: The etiologic spectrum widens Degradative macroautophagy (hereafter referred to as autophagy) is a conserved catabolic pathway required for cellular adaptation to nutrient deprivation and for degradation of damaged intracellular organelles and insoluble protein aggregates. Autophagy is a highly regulated cellular process that involves multiple steps (starting with autophagy induction and ending with degradation of sequestered cargo by lysosomal hydrolases), disruption of each can lead to human disease [reviewed in detail in (Margeta, 2020a)]. From the muscle pathology perspective, the most recognizable autophagy defect involves inhibition of the bulk autophagic flux, which results in the autophagic vacuolar myopathy (AVM) phenotype; however, defects of autophagy induction and cargo sequestration can also result in muscle disease (Fig. 3). Several new diseases with autophagic impairment were identified in 2021, expanding the spectrum of etiologies that cause skeletal myopathy through dysregulation of autophagy; interestingly, however, all of them map on one of the four previously identified pathogenetic pathways illustrated in Fig. 3.
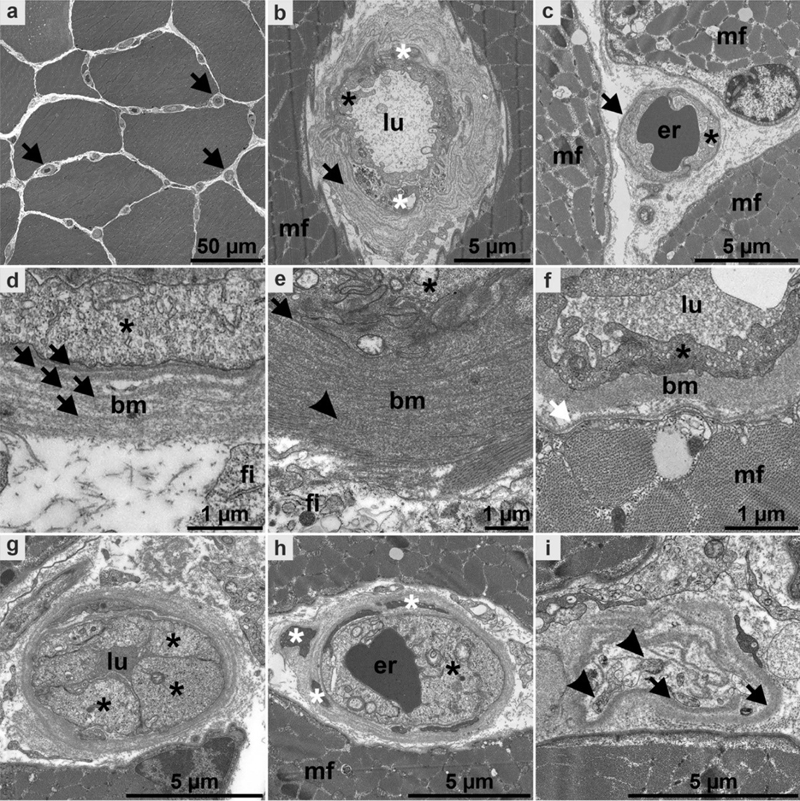
Figure 3. The role of autophagic defects in the pathogenesis of skeletal myopathies. In myopathies with autophagy induction defects, the accumulation of damaged cellular organelles activates signaling cascades that contribute to fiber atrophy and apoptosis; however, there is no accumulation of autophagosomes. In contrast, autophagic vacuolar myopathies are caused by defects in the general autophagic flux that lead to a massive accumulation of autophagosomes and undigested cargo, ultimately resulting in a reduction of the mechanical force generated during muscle contraction (i.e., muscle weakness) and a failure of muscle regeneration. Finally, cargo recognition defects lead to two different, defect-specific disease phenotypes: A granulophagy defect results in rimmed vacuole formation and inclusion body myopathy, while a CASA defect causes myofibrillar myopathy by impairing Z-disc stability. The electron micrographs illustrate (a) subsarcolemmal accumulation of damaged mitochondria that show marked variation in their size and shape; (b) an autophagic vacuole with an accumulation of undigested, electron-dense autophagic cargo; (c) a rimmed vacuole with a rim of autophagic material and a center that consists of aggregated proteins; and (d) myofibrillar disorganization with streaming of the Z-disc material. [This figure and its legend are reproduced from (Margeta, 2020a) with permission from the Annual Review of Pathology: Mechanisms of Disease, Volume 15 © 2020 by Annual Reviews, http://www.annualreviews.org/.] When there is a block of autophagy induction, autophagosomes do not normally form and therefore cannot significantly accumulate; however, there is accumulation of damaged and degenerating intracellular organelles, which ultimately leads to fiber atrophy and apoptosis. The autophagy induction defect plays an important role in the pathogenesis of at least some muscular dystrophies and congenital myopathies; however, the complete block of autophagy induction is embryonically or perinatally lethal in animal models, and no human disease has previously been attributed to mutations in one of the core autophagy genes (Margeta, 2020a). That changed in 2021, when Collier at al. identified five independent families with autosomal recessive mutations in ATG7 (a core autophagy-related protein that is required for lipidation of LC3, the key step in induction of degradative autophagy); the affected individuals have a complex developmental disorder that commonly includes cerebellar hypoplasia, corpus callosum abnormalities, facial dysmorphism, and mild proximal myopathy (Collier et al., 2021). Muscle biopsies were performed on a few affected individuals and showed mild myopathic changes mimicking those seen in the autophagy-deficient murine muscle, with moderate mitochondrial abnormalities, lipofuscin accumulation, subsarcolemmal accumulation of autophagic cargo receptor p62/SQSTM1 (encoded by SQSTM1 gene), and diminished levels of LC3-II (the lipidated, autophagosome-bound form of LC3); while some autophagosomes were present, there was no accumulation of autophagic vacuoles. Intriguingly, another potential myopathy with impaired autophagy induction was reported last year by Napolitano and co-authors (Napolitano et al., 2021): while these authors classified their patient 6 as having an AVM, his muscle biopsy showed high p62 and low LC3-II (as would be expected with the autophagy initiation defect) rather than high levels of both p62 and LC3-II (as would be expected in a true AVM caused by the autophagic flux defect). Interestingly, that individual was found to carry a potentially deleterious variant in TBC1D5 gene, which has not previously been associated with human disease but was shown to regulate autophagy initiation (Popovic and Dikic, 2014). Specific classification of TBC1D5-associated myopathy aside, Napolitano et al. showed that the AVM pathology mimicking late-onset Pompe disease (LOPD) can be associated with mutations in genes not previously associated with this clinicopathologic phenotype (such as titin, dysferlin, plectin, and perilipin 3, among others); this highlights the importance of genetic diagnosis for LOPD, which can be treated by enzyme replacement therapy (ERT; further discussed in advance #10) – a treatment that is unlikely to be effective if the underlying molecular defect is not acid α-glucosidase (GAA) deficiency. Cargo recognition defects, which result in selective (rather than global) autophagy dysfunction, can also cause muscle disease: impairment of granulophagy (autophagy of stress granules, which are ribonucleoprotein foci that form under cellular stress and, if persistent, need to be degraded via autophagy) leads to an inclusion body myopathy phenotype, while impairment of chaperone-assisted selective autophagy (CASA), which is critical for the Z-disc maintenance, results in myofibrillar myopathy (Fig. 3). Each of these phenotypes has been associated with mutations in many different genes; in 2021, two new genes were added to this ever-growing list. In the first study, Leoni et al. showed that autosomal dominant missense variants in annexin A11, a 505 aa calcium-dependent phospholipid-binding protein, lead to hereditary inclusion body myopathy, amyotrophic lateral sclerosis, and frontotemporal lobar degeneration (Leoni et al., 2021); given that other mutations in ANXA11 (annexin A11-encoding gene) were previously shown to cause amyotrophic lateral sclerosis and frontotemporal degeneration (Zhang et al., 2018), ANXA11 is now the sixth gene known to cause multiple system proteinopathy (MSP type 6). The other 5 genes associated with the MSP phenotype encode either RNA-binding proteins that form stress granules (HNRNPA2B1, HNRNPA1, and MATR3 genes) or autophagy-associated regulatory proteins (VCP and SQSTM1 genes); while the precise function of annexin 11 still needs to be elucidated, it most likely falls in the latter category given that other annexin A proteins play a role in autophagy regulation (Xi et al., 2020). Interestingly, rimmed vacuoles in MSP-6 patients are positive for annexin 11 in addition to TDP-43, while rimmed vacuoles in sporadic inclusion body myositis (sIBM) and other inclusion body myopathies are annexin 11-negative (Leoni et al., 2021). In the second study, Johari and colleagues showed that autosomal dominant missense mutations in SMPX (small muscle protein X-linked) cause distal myopathy with protein inclusions (Johari et al., 2021). SMPX is a small (88 aa), proline-rich protein that is highly expressed in slow muscle fibers and cardiomyocytes, where it localizes to costameres and intermyofibrillar spaces; its function is currently unknown, but loss-of-function SMPX mutations cause non-syndromic hearing loss without muscle weakness. Muscle biopsies from patients with SMPX-related distal myopathy, who do not have hearing loss, showed LC3-positive rimmed vacuoles, abundant SMPX-and p62-positive sarcoplasmic inclusions, as well as SMPX-negative inclusions that were positive for αB-crystallin and myotilin in addition to CASA chaperones BAG3 and HSPB8; however, there was no significant myofibrillar disarray on electron microscopy. Thus, it is not yet clear whether this new disease should be classified as a rimmed vacuolar (inclusion body) myopathy or as a myofibrillar myopathy; while a lot of additional work is needed to fully elucidate its pathogenesis, initial experiments suggest that SMPX may affect stress granule dynamics (Johari et al., 2021). Thus, it will be interesting to see whether SMPX mutations can also cause other diseases in the MSP spectrum, either alone or in combination with mutations in other MSP-associated genes. 7. Activation of the integrated stress response plays a key role in the pathogenesis of tRNA synthetase-associated subtypes of axonal Charcot-Marie-Tooth disease Non-syndromic inherited sensory-motor peripheral neuropathies, also known as Charcot-Marie-Tooth (CMT) diseases, are broadly classified into demyelinating, axonal, and intermediate subtypes, each of which is associated with a large number of causative genes and with more than one mode of inheritance (Stavrou et al., 2021; Zhang et al., 2021). Within the axonal CMT category, an interesting and relatively recently recognized disease subset is caused by mutations in aminoacyl-tRNA synthetases (ARSs), which are ubiquitously expressed enzymes that charge amino acids onto their cognate tRNAs during protein synthesis. Of 20 ARSs, 5 have been associated with autosomal dominant forms of axonal CMT disease [YARS (tyrosyl-RS; CMTDIC), GARS (glycyl-RS; CMT2D), AARS (alanyl-RS; CMT2N), HARS (histidyl-RS; CMT2W), and MARS (methionyl-RS; CMT2U)], while two (WARS / tryptophanyl-RS and KARS / lysyl-RS) have been associated with hereditary motor neuropathy type 9 (HMN9) and autosomal recessive intermediate CMT disease CMTRIB, respectively. (Of note, GARS mutations can cause HMN5A in addition to CMT2D, while HARS mutations can cause HMN2 in addition to CMT2W.) Not much was known about pathogenesis of ARS-associated forms of CMT until last year, when two fascinating studies were published back-to-back in Science, together providing important mechanistic insights and therapeutic promise for this subcategory of inherited neuropathies (Spaulding et al., 2021; Zuko et al., 2021). Spaulding et al. used three different mouse models of GARS-CMT (CMT2D) and one mouse model of YARS-CMT (CMTDIC) to investigate molecular pathways that are affected by mutant gene expression (Spaulding et al., 2021). In all four investigated mouse models, they found that the integrated stress response (ISR) was selectively activated in alpha motor neurons and a subset of sensory neurons; the ISR activation preceded neurologic symptom onset, was associated with increased expression of genes regulated by transcription factor ATF4, and required sensor kinase GCN2. [The ISR is a conserved cellular signaling pathway that alters gene expression program in response to various cellular stressors, including protein homeostasis defects, nutrient deprivation, viral infection, and oxidative stress (Costa-Mattioli and Walter, 2020). These stresses are sensed by four specialized kinases (PERK, GCN2, PKR and HRI), activation of which ultimately leads to phosphorylation of the eukaryotic translation initiation factor eIF2 and general reduction in protein synthesis along with an increase in translation of specific mRNAs, such as ATF4. If these adaptive responses fail to mitigate cellular stress, the ISR triggers programmed cell death.] Genetic deletion of GCN2 completely rescued the neuropathy phenotype in the GARS mutant mice, with beneficial effects of deletion observed behaviorally, physiologically (as improved sciatic nerve conduction velocity), and pathologically (as ameliorated axon loss, increased axon diameter, and decreased muscle denervation). While only one of three GARS-CMT mouse models was tested in these genetic studies, similar results were observed in a different GARS-CMT model following pharmacologic inhibition of GCN2, with treatment that was initiated at disease onset (2 weeks of age); interestingly, the effect of pharmacologic GCN2 inhibition was greater in male than female mice, but the reason for this sex difference is currently unclear. In a parallel study, Zuko et al. investigated mechanisms underlying inhibition of global protein synthesis that was previously documented in 6 different GARS-CMT and YARS-CMT mouse lines and could not be rescued by overexpression of wt GARS or YARS. While manipulation of translation initiation and upstream regulatory pathways had no significant effect, overexpression of tRNAGly rescued both the protein synthesis deficit and neuropathy phenotype in two Drosophila models of GARS-CMT. These findings were replicated in two mouse models of GARS-CMT, with tRNAGly overexpression resulting in an essentially complete behavioral, physiologic, and pathologic rescue of peripheral neuropathy (Zuko et al., 2021). In addition, Zuko and colleagues showed that inhibition of global protein synthesis in this mouse model was due to tRNAGly sequestration by mutant GARS, which led to ribosome stalling at Gly codons; as a result, the neuropathy in GARS-CMT mice was worsened by concurrent deletion of the ribosome rescue factor GTPBP2, which by itself does not lead to nerve damage. Finally, connecting the dots between the two studies, Zuko et al. showed that tRNAGly overexpression abrogated activation of the ISR in the GARS-CMT mouse model, indicating that depletion of the normal tRNAGly pool and consequent ribosome stalling are the upstream signals that lead to the ISR activation. Taken together, these two studies suggest that ARS mutations cause autosomal dominant axonal CMT disease through a toxic gain-of-function mechanism: by binding more tightly to their cognate tRNAs, they deplete the free tRNA pool, ultimately leading to ribosome stalling, aberrant ISR activation, and axonal degeneration. Despite the very comprehensive nature of this work, additional questions need to be answered. For example, it remains to be shown whether the same (or similar) molecular mechanism plays a role in the pathogenesis of the AARS-, HARS-, and MARS-associated CMT, and in axonal CMT more broadly. In addition, it is not clear which downstream effect of the ISR activation (protein synthesis inhibition or the ATF4 pathway activation) leads to axonal degeneration. Nonetheless, and very excitingly, this work opens a new direction for the CMT treatment development: manipulation of the ISR is emerging as a promising therapeutic avenue for several age-associated diseases, including neurodegeneration and cancer (Costa-Mattioli and Walter, 2020), and at least some subtypes of axonal CMT can now be added to that list. [As an aside, ARS enzymes also play an important role in anti-synthetase syndrome (ASS), where they are targeted by disease-causing autoantibodies (histidyl-RS is targeted by anti-Jo-1 antibodies, alanyl-RS by anti-PL12 antibodies, glycyl-RS by anti-EJ antibodies, lysyl-RS by anti-SC antibodies, and tyrosyl-RS by anti-YRS antibodies; Witt et al., 2016). ASS and CMT disease have entirely different clinical manifestations, so the underlying pathogenetic mechanisms are likely also different despite this common link; while there is some evidence that protein translation is affected in ASS – see advance #9 – it remains to be established whether the ISR activation and/or protein synthesis inhibition play a role in the ASS pathogenesis.] ADVANCES IN NEUROMUSCULAR DISEASE DIAGNOSTICS 8. Microvascular pathology in immune-mediated neuromuscular disease Major vascular pathology (such as vasculitis or amyloid vasculopathy) has long been recognized as an important cause of neuromuscular disease, and vessel evaluation on routine stains is a standard component of diagnostic neuromuscular pathology workup. The role of microvascular pathology is less well understood, but some microvascular abnormalities [such as deposition of C5b9 (complement membrane attack complex) in the endomysial capillaries] are included in the diagnostic criteria for several idiopathic inflammatory myopathies (IIMs) including DM, anti-synthetase syndrome-associated myositis (ASSM), and immune-mediated necrotizing myopathy (IMNM). Two studies published last year (Siegert et al., 2021; Trikamji and Pestronk, 2021) expanded the spectrum of microvascular abnormalities seen in immune-mediated neuromuscular disorders, highlighting that careful evaluation of endomysial and endoneurial microvessels (arterioles and capillaries) can increase the diagnostic yield of muscle and nerve biopsies. Systemic sclerosis (SSc) is a systemic autoimmune disease characterized by fibrosis of skin and internal organs, vasculopathy, and evidence of immune system dysregulation; skeletal muscle involvement is variable, with some patients developing a superimposed specific IIM or less specific “overlap myositis”, while others (~20%) have a poorly understood muscle disease specific to SSc. To better define the latter disease entity, Siegert et al. performed detailed retrospective evaluation of muscle biopsies from 18 SSc patients with muscle symptoms (derived from a larger cohort of 367 SSc patients) using routine light microscopy as well as semi-quantitative large scale electron microscopy [described as advance #9 in last year’s review (Margeta, 2021)]. Two thirds of evaluated SSc biopsies (12 of 18) showed a novel morphologic pattern (which the authors termed “minimal myositis with capillary pathology”; MMCP) characterized by sparse endomysial T cells, rare necrotic and regenerating muscle fibers, diffuse MHC-I and focal MHC-II upregulation, and enlarged capillaries with prominent pericytes but no capillary C5b9 deposition; ultrastructurally, MMCP cases showed well-developed but mild capillary pathology, including thickening and reduplication of basement membranes, reactive endothelial changes, and capillary ensheathment by pericyte processes (Fig. 4). Similar but more severe capillary alterations were seen in other 6 SSc muscle biopsies, which also showed additional capillary abnormalities (such as tubuloreticular inclusions) and more prominent inflammatory changes; therefore, capillary pathology is a uniform feature of MMCP cases but is not pathognomonic for this condition, and must be interpreted in the context of other muscle biopsy findings. Interestingly, MMCP SSc cases were clinically less severe than non-MMCP SSc cases, with higher frequency of localized (versus diffuse) skin sclerosis, less prominent internal organ involvement, and lower CK levels; however, these muscle abnormalities developed early in the disease course, with mean disease duration of 3 years at the time of biopsy (<1 year in 6 of 12 cases).
Figure 4. Ultrastructural characterization of skeletal muscle biopsies with histological minimal myositis with capillary pathology (MMCP) phenotype. Entire ultrathin sections were recorded by large-scale digitization at 7.3 nm pixel size; digitally magnified regions of interests (ROI) of patients 3 (a, d, g–l), 8 (b, m), 6 (e), 2 (f), 18 (n; severe necrotizing myositis with capillary pathology and fibrosis), 1 (o) and non-diseased control (c). a Markedly thickened capillaries can be clearly identified at low magnification (arrows). b Capillary with pronounced thickening and reduplication (arrow) of the basement membrane (BM) as well as ensheathment by pericyte processes (white asterisk), mildly activated endothelium (black asterisk), lumen (lu), adjacent muscle fiber (mf). c Healthy capillary with thin BM (arrow): note that no reduplication is apparent, endothelium with no signs of activation (asterisk), lumen with erythrocyte (er). Different types of BM (bm) thickening were detected (d–f): Distinct reduplication (d; arrows), endothelium (asterisk), fibroblast (fi); fuzzy appearance with less pronounced reduplication (e): note that the BM (arrow) directly underneath the endothelium (asterisk) is clearly visible, fibrous long spacing collagen (arrowhead); homogeneous thickened BM (f), capillary lumen (lu), neighboring muscle fiber (mf) with basal lamina (white arrow). Different types of endothelial activation (g–i): Increased size and number of endothelial cells (g; asterisk, lu lumen), note the granular appearance of the cytoplasm, probably mostly due to ribosomes; prominent endothelial membrane organelles (h; black asterisk, er erythrocyte in lumen), note the prominent and mostly small pericyte processes demonstrating mild ensheathment (white asterisks); degraded capillary (i), showing some remaining membrane structures, probably of endothelial or pericyte origin (arrowheads), almost empty BM “sack” with mild reduplication (arrows). [This figure and its legend were adopted from Figure 3 in (Siegert et al., 2021); this use is permitted under the Creative Commons Attribution 4.0 International License.] While at least some aspects of microvascular pathology are routinely evaluated in muscle biopsies, the same is not true for nerve biopsies; the 2021 study by Trikamji and Pestronk suggests that this approach to nerve biopsy processing should probably change. These authors have retrospectively analyzed a cohort of 16 patients with a motor-sensory axonal polyneuropathy and complement deposition in endoneurial microvessels, detected by C5b9 immunohistochemistry performed on nerve cryosections. This patient cohort showed unique clinicopathologic features that could reflect a new / previously unrecognized autoimmune neuropathy, which the authors termed “humoral immune endoneurial microvasculopathy” (HIEM). Clinically, HIEM patients showed progressive asymmetric distal weakness that was more prominent in lower extremities; there was no evidence of a systemic inflammatory process. Pathologically, there was a patchy / asymmetric axon loss that preferentially affected myelinated axons, with rare digestion chambers and rare regenerating axon clusters but no significant inflammation; strong C5b9 staining was seen surrounding the endothelium in all or nearly all endoneurial microvessels, and was also detectable in endomysial capillaries in the majority of paired muscle biopsies (Trikamji and Pestronk, 2021). A potentially confounding factor is that similar capillary changes were previously documented in nerve and muscle biopsies from diabetic patients (Yell et al., 2018); 56% of the patients in the HIEM cohort also had diabetes, and the mean age of onset was lower in diabetic than non-diabetic patients. However, and very compellingly, 15 of 16 HIEM patients showed a measurable strength improvement following a short course of corticosteroid therapy; this would not be expected if the observed nerve pathology was mainly due to chronic (and likely irreversible) diabetic neuropathy. While very intriguing, these findings need to be replicated in other patient cohorts, with corticosteroid treatment effectiveness confirmed by double-blind clinical trials. In addition, both nerve and muscle biopsies from HIEM patients should be evaluated by electron microscopy: it is possible that ultrastructural evaluation will yield additional useful clues, either from pathogenetic or diagnostic perspective. Nonetheless, Trikamji and Pestronk’s findings suggest that a portion of each nerve biopsy should be frozen for specialized immunohistochemical studies, which is currently not a standard operating protocol in the majority of neuromuscular pathology laboratories: in addition to enabling identification of potentially treatable HIEM patients, such processing would also facilitate detection of immunoglobulin deposits that are important for accurate classification of amyloid and vasculitic neuropathies. 9. Gene expression profiling in idiopathicinflammatory myopathies Based on the current clinicoseropathologic criteria, IIMs are divided into four distinct subcategories [DM, ASSM, IMNM, and sIBM; for a brief overview of the diagnostic criteria and other recent advances in the IIM field, see the 2020 update in this article series (Margeta, 2020b)]. An interesting study published last year (Amici et al., 2021) has used a gene expression profiling approach to take a deeper look into these disorders; while the current data is mainly interesting from the standpoint of disease pathogenesis, this study also provides a glimpse into the use of transcriptomic profiles for disease diagnostics. The authors used RNA-sequencing data from 119 IIM muscle biopsies [39 DM cases, 18 ASSM cases, 49 IMNM cases, and 13 sIBM cases; all ASSM cases were positive for anti-Jo-1 antibodies, while the DM and IMNM groups were heterogenous with respect to the patient’s serologic status, with 5-40 cases per myositis-specific antibody (MSA) subgroup] and 20 normal muscle biopsies to generate transcriptome maps and identify gene expression modules that are dynamically regulated in IIMs. Some of the results were not surprising; for example, DM biopsies showed activation of the type 1 interferon-inducible gene module, which was not significantly upregulated in other IIM subtypes, while sIBM cases were unique in showing consistent overexpression of T cell genes. Other findings, however, were novel and somewhat surprising. For example, two gene modules – the stress response acute phase response module and the neutrophil degranulation module – were upregulated across all IIM subtypes (including IMNM cases, which generally lack significant inflammation), as was the cytoskeleton remodeling module, which includes TGF-β and could be related to endomysial fibrosis seen in many long-standing IIM cases; in contrast, the large muscle function, redox metabolism, and ubiquitination gene module was downregulated across all IIM subtypes. Expression changes in some gene modules were more specific and characteristic for individual IIM subtypes: for example, the previously mentioned upregulation of the type 1 interferon-induced gene module in DM cases was strongly correlated with downregulation of the titin transcript, while the ASSM cases showed upregulation of the RNA binding, splicing, and translation genes. In addition to studying gene expression changes across different IIM subtypes, the authors of this study converted individual trascriptomic profiles into images suitable for computational analysis by a convolutional neural network. Unsupervised hierarchical clustering by neural network-derived features led to an interesting hierarchy of different patient subgroups, with the severe DM cases clustering closer to the ASSM cases and severe IMNM cases than to the mild DM and IMNM cases; one severe anti-Mi-2 DM case was even misclassified within the ASSM group. This finding is congruent with the experience on a diagnostic muscle pathology service, where one can occasionally see a significant histopathologic overlap between anti-Mi-2 DM, ASSM, and severe IMNM (Fig. 5). Interestingly, in the group of 119 IIM cases studied by Amici at al., disease severity did not correlate with a specific MSA subtype; instead, both mild and severe cases were seen in each MSA-defined subgroup. If validated by future studies and found to correlate with the response to therapy and/or patient outcomes, this finding suggests that transcriptomic analysis might be able to extract clinically useful information not captured by serotype / disease subtype, and that gene expression profiling therefore may at some point become a routine component of diagnostic muscle biopsy work-up. Excitingly, the authors of this study have shared the source code and model weights on their website (https://github.com/mendillolab), and this tool can be used by other researchers who perform muscle transcriptomics to further test and improve their algorithm.
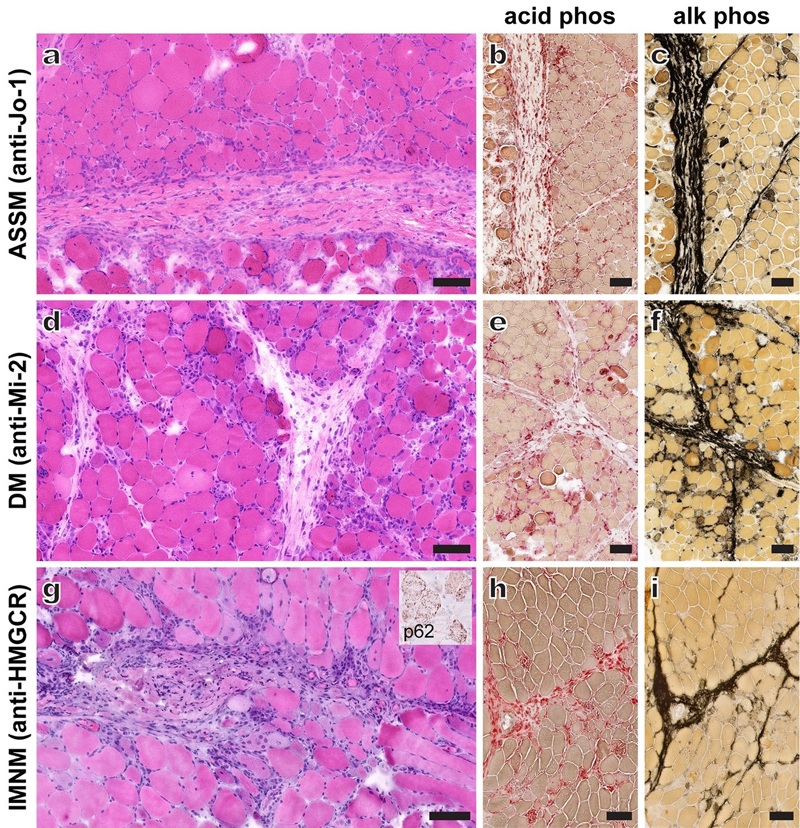
Figure 5. Histologic overlap between ASSM (a-c), anti-Mi-2 DM (d-f), and a severe case of anti-HMGCR IMNM (g-i). A typical ASSM case shows perifascicular fiber atrophy and necrosis (a) along with marked perimysial abnormalities [edema, fragmentation, macrophage-rich inflammation (best visualized on acid phosphatase stain; b) and a linear pattern of alkaline phosphatase positivity (c)]. Anti-Mi-2-associated DM often leads to a more severe muscle involvement than other DM subtypes and can histologically mimic ASSM; in this example (d-f), there was a prominent perimysial involvement including macrophage-rich inflammation (e) and strong alkaline phosphatase staining (f). Markers of type 1 interferon response (such as MxA) can help differentiate DM from ASSM, but in the UCSF experience MxA upregulation is often weak in anti-Mi-2 DM cases. Typical IMNM cases show little to no inflammation and are generally easily distinguished from other autoimmune myopathies; however, severe cases (such as the one shown in g-i) can be diagnostically challenging. This anti-HMGCR IMNM case showed abundant macrophage-rich inflammatory infiltrate in the perimysium (h) along with well-developed perimysial alkaline phosphatase positivity (i); the only clue to the correct diagnosis was dense punctate p62 staining of muscle fibers (inset in g), which is not typically seen in either DM or ASSM. Representative cryosection images are shown for all three cases; scale bars, 100 μm. ADVANCES IN NEUROMUSCULAR DISEASE TREATMENT 10. Clinical trials: Late-onset Pompe disease revisited Pompe disease is an autosomal recessive metabolic disorder caused by loss-of-function mutations in GAA, the lysosomal glycogen-catabolizing enzyme; depending on the level of residual GAA activity, the disease can present in infancy, childhood, or adulthood. While early onset Pompe disease is a systemic disorder that affects multiple organs systems, LOPD primarily affects skeletal musculature and is characterized by progressive weakness of the axial, limb-girdle, and respiratory muscles; pathologically, vacuolated muscle fibers show an accumulation of membrane-bound as well as free glycogen and a build-up of autophagic debris (Fig. 6), so this disease is currently classified as an AVM (Fig. 6). ERT with alglucosidase alfa, recombinant form of human GAA, was approved in 2006, constituting a breakthrough in Pompe disease management; however, most LOPD patients on this therapy experience a short-term improvement followed by progressive decline. The failure of ERT in LOPD is thought to primarily reflect inefficient delivery of alglucosidase alfa to skeletal muscle lysosomes: efficient lysosomal targeting is based on binding of mannose 6-phosphate (M6P)-glycans and bis-M6P-glycans within the recombinant protein to the cation-independent M6P receptor in the target tissue, and only a minor fraction of originally developed recombinant GAA contains bis-M6P ligands.
Figure 6. Muscle biopsy findings in LOPD. A representative H&E-stained cryosection (a) shows largely unremarkable skeletal muscle with a single highly vacuolated muscle fiber in this microscopic field (black arrowhead). The same microscopic field from a PAS (periodic acid-Schiff)-stained cryosection (b) shows two vacuolated muscle fibers with mild glycogen accumulation (black arrowheads); the less vacuolated fiber at the bottom of the image shows no obvious changes on the corresponding H&E-stained section (a). Electron microscopy shows an increase in the lysosomal (membrane-bound) glycogen (white arrowheads in c) as well as accumulation of free sarcoplasmic glycogen accompanied by electron dense autophagic debris (d). The focal nature of these pathologic findings is typical for LOPD, although the degree of muscle fiber involvement varies from case to case. Scale bars: a and b, 60 μm; c and d, 2 μm. To try circumventing this problem, two new versions of recombinant GAA were developed and tested against the current standard of care (alglucosidase alfa), with the results of both clinical trials published last year in Lancet Neurology (Diaz-Manera et al., 2021; Schoser et al., 2021). To generate the first investigational drug, avalglucosidase alfa, synthetic bis-M6P-glycane-containing oligosaccharides were chemically conjugated to recombinant human GAA; the safety and efficacy of this drug was evaluated by the COMET study, a phase 3, randomized, double-blind clinical trial involving 55 sites in 20 countries (Diaz-Manera et al., 2021). The second investigational drug, cipaglucosidase alfa, is a novel recombinant human GAA with a high bis-M6P glycan content that is co-administered with a pharmacologic chaperone (miglustat) to increase its bioavailability; the safety and efficacy of this drug combination was evaluated by the PROPEL study, also a phase 3, randomized, double-blind clinical trial that involved 62 sites in 24 countries (Schoser et al., 2021). The COMET trial enrolled 100 ERT-naïve LOPD patients who were randomized into equally sized avalglucosidase alfa and alglucosidase alfa groups; the PROPEL trial, on the other hand, had a parallel group design (28 ERT-naïve participants and 95 participants previously treated with alglucosidase alfa), with two thirds of participants in each subgroup receiving cipaglucosidase alfa + miglustat and one third receiving alglucosidase alfa + placebo. While the details of the study design differed slightly between the two trials, they had similar duration (49 weeks for COMET and 52 weeks for PROPEL) and their outcomes were quite similar: (1) the safety of both investigational drugs was high, with no new safety signals reported; (2) neither investigational drug was inferior to alglucosidase alfa, the current standard of care; and (3) while there was a trend toward increased efficacy for both investigational drugs, neither reached a statistically significant primary end-point. Given the very promising results of prior preclinical (mouse model) studies and initial phase 1/2 trials (Meena et al., 2020; Puertollano and Raben, 2021), these results are somewhat disappointing. Intriguingly, however, the cipaglucosidase alfa + miglustat treatment was significantly more effective than the alglucosidase alfa + placebo treatment in the ERT-experienced subgroup of the PROPEL study, which is arguably most representative of the segment of the LOPD patient population with the greatest need for new and more effective LOPD therapies. Both trials have now moved into their last phase (open label extended treatment period), the aim of which is to assess the long-term safety and efficacy of these new drugs; it will be interesting to see whether the difference in the efficacy profile between either investigational drug and alglucosidase alfa becomes greater over time or whether they will show a similar loss of efficacy over time. In addition, it will be interesting to directly compare the two new LOPD drugs and determine whether one of them is superior to the other with respect to the size of initial improvement, effect duration, or both. Most importantly, however, the modest results of these large and expensive clinical trials indicate that the cure for LOPD remains elusive and highlight the need for a novel, ideally more effective and durable, LOPD treatment approach going forward. Disclosure statement The author receives research support from Astellas Gene Therapies (formerly known as Audentes Therapeutics, Inc) as a member of the muscle biopsy review committee for the ASPIRO (NCT03199469) and FORTIS (NCT04174105) clinical trials, which are evaluating the safety and efficacy of gene transfer therapy for X-linked myotubular myopathy (ASPIRO) and LOPD (FORTIS). Acknowledgements I am grateful to Drs. Nigel G. Laing, Gina Ravenscroft, and Benedikt Schoser for helpful input during the conceptualization stage of this review. In addition, I would like to thank Ms. Christine Lin for assistance with figure preparation. References Ahmady, E., Deeke, S.A., Rabaa, S., Kouri, L., Kenney, L., Stewart, A.F., and Burgon, P.G. (2011). Identification of a novel muscle A-type lamin-interacting protein (MLIP). J Biol Chem 286, 19702-19713. Allen, J.M., Zamurs, L., Brachvogel, B., Schlotzer-Schrehardt, U., Hansen, U., Lamande, S.R., Rowley, L., Fitzgerald, J., and Bateman, J.F. (2009). Mice lacking the extracellular matrix protein WARP develop normally but have compromised peripheral nerve structure and function. J Biol Chem 284, 12020-12030. Amici, D.R., Pinal-Fernandez, I., Christopher-Stine, L., Mammen, A.L., and Mendillo, M.L. (2021). A network of core and subtype-specific gene expression programs in myositis. Acta Neuropathol 142, 887-898. Amore, G., Romagnoli, M., Carbonelli, M., Barboni, P., Carelli, V., and La Morgia, C. (2021). Therapeutic options in hereditary optic neuropathies. Drugs 81, 57-86. Aschman, T., Schneider, J., Greuel, S., Meinhardt, J., Streit, S., Goebel, H.H., Buttnerova, I., Elezkurtaj, S., Scheibe, F., Radke, J., et al. (2021). Association between SARS-CoV-2 infection and immune-mediated myopathy in patients who have died. JAMA Neurol 78, 948-960. Cattin, M.E., Wang, J., Weldrick, J.J., Roeske, C.L., Mak, E., Thorn, S.L., DaSilva, J.N., Wang, Y., Lusis, A.J., and Burgon, P.G. (2015). Deletion of MLIP (muscle-enriched A-type lamin-interacting protein) leads to cardiac hyperactivation of Akt/mammalian target of rapamycin (mTOR) and impaired cardiac adaptation. J Biol Chem 290, 26699-26714. Collier, J.J., Guissart, C., Olahova, M., Sasorith, S., Piron-Prunier, F., Suomi, F., Zhang, D., Martinez-Lopez, N., Leboucq, N., Bahr, A., et al. (2021). Developmental consequences of defective ATG7-mediated autophagy in humans. N Engl J Med 384, 2406-2417. Costa-Mattioli, M., and Walter, P. (2020). The integrated stress response: From mechanism to disease. Science 368, eaat5314. Deschauer, M., Hengel, H., Rupprich, K., Kreiss, M., Schlotter-Weigel, B., Grimmel, M., Admard, J., Schneider, I., Alhaddad, B., Gazou, A., et al. (2021). Bi-allelic truncating mutations in VWA1 cause neuromyopathy. Brain 144, 574-583. Diaz-Manera, J., Kishnani, P.S., Kushlaf, H., Ladha, S., Mozaffar, T., Straub, V., Toscano, A., van der Ploeg, A.T., Berger, K.I., Clemens, P.R., et al. (2021). Safety and efficacy of avalglucosidase alfa versus alglucosidase alfa in patients with late-onset Pompe disease (COMET): a phase 3, randomised, multicentre trial. Lancet Neurol 20, 1012-1026. Dodig, D., Tarnopolsky, M.A., Margeta, M., Gordon, K., Fritzler, M.J., and Lu, J.Q. (2022). COVID-19-associated critical illness myopathy with direct viral effects. Ann Neurol, ePub ahead of print. Esslinger, U., Garnier, S., Korniat, A., Proust, C., Kararigas, G., Muller-Nurasyid, M., Empana, J.P., Morley, M.P., Perret, C., Stark, K., et al. (2017). Exome-wide association study reveals novel susceptibility genes to sporadic dilated cardiomyopathy. PLoS One 12, e0172995. Filosto, M., Cotti Piccinelli, S., Gazzina, S., Foresti, C., Frigeni, B., Servalli, M.C., Sessa, M., Cosentino, G., Marchioni, E., Ravaglia, S., et al. (2021). Guillain-Barre syndrome and COVID-19: an observational multicentre study from two Italian hotspot regions. J Neurol Neurosurg Psychiatry 92, 751-756. Fragiel, M., Miro, O., Llorens, P., Jimenez, S., Pinera, P., Burillo, G., Martin, A., Martin-Sanchez, F.J., Garcia-Lamberechts, E.J., Jacob, J., et al. (2021). Incidence, clinical, risk factors and outcomes of Guillain-Barre in Covid-19. Ann Neurol 89, 598-603. Ho, R., and Hegele, R.A. (2019). Complex effects of laminopathy mutations on nuclear structure and function. Clin Genet 95, 199-209. Huang, Z.P., Kataoka, M., Chen, J., Wu, G., Ding, J., Nie, M., Lin, Z., Liu, J., Hu, X., Ma, L., et al. (2015). Cardiomyocyte-enriched protein CIP protects against pathophysiological stresses and regulates cardiac homeostasis. J Clin Invest 125, 4122-4134. Jha, M.K., Passero, J.V., Rawat, A., Ament, X.H., Yang, F., Vidensky, S., Collins, S.L., Horton, M.R., Hoke, A., Rutter, G.A., et al. (2021). Macrophage monocarboxylate transporter 1 promotes peripheral nerve regeneration after injury in mice. J Clin Invest 131, e141964. Johari, M., Sarparanta, J., Vihola, A., Jonson, P.H., Savarese, M., Jokela, M., Torella, A., Piluso, G., Said, E., Vella, N., et al. (2021). Missense mutations in small muscle protein X-linked (SMPX) cause distal myopathy with protein inclusions. Acta Neuropathol 142, 375-393. Keddie, S., Pakpoor, J., Mousele, C., Pipis, M., Machado, P.M., Foster, M., Record, C.J., Keh, R.Y.S., Fehmi, J., Paterson, R.W., et al. (2021). Epidemiological and cohort study finds no association between COVID-19 and Guillain-Barre syndrome. Brain 144, 682-693. Keh, R.Y.S., Scanlon, S., Datta-Nemdharry, P., Donegan, K., Cavanagh, S., Foster, M., Skelland, D., Palmer, J., Machado, P.M., Keddie, S., et al. (2022). COVID-19 vaccination and Guillain-Barré syndrome: analyses using the National Immunoglobulin Database. medRxiv, 2021.2012.2014.21267418. Kieninger, S., Xiao, T., Weisschuh, N., Kohl, S., Ruther, K., Kroisel, P.M., Brockmann, T., Knappe, S., Kellner, U., Lagreze, W., et al. (2022). DNAJC30 disease-causing gene variants in a large Central European cohort of patients with suspected Leber's hereditary optic neuropathy and optic atrophy. J Med Genet. Leoni, T.B., Gonzalez-Salazar, C., Rezende, T.J.R., Hernandez, A.L.C., Mattos, A.H.B., Coimbra Neto, A.R., da Graca, F.F., Goncalves, J.P.N., Martinez, A.R.M., Taniguti, L., et al. (2021). A novel multisystem proteinopathy caused by a missense ANXA11 variant. Ann Neurol 90, 239-252. Liu, J., Huang, Z.P., Nie, M., Wang, G., Silva, W.J., Yang, Q., Freire, P.P., Hu, X., Chen, H., Deng, Z., et al. (2020). Regulation of myonuclear positioning and muscle function by the skeletal muscle-specific CIP protein. Proc Natl Acad Sci U S A 117, 19254-19265. Lopes Abath Neto, O., Medne, L., Donkervoort, S., Rodriguez-Garcia, M.E., Bolduc, V., Hu, Y., Guadagnin, E., Foley, A.R., Brandsema, J.F., Glanzman, A.M., et al. (2021). MLIP causes recessive myopathy with rhabdomyolysis, myalgia and baseline elevated serum creatine kinase. Brain 144, 2722-2731. Luijten, L.W.G., Leonhard, S.E., van der Eijk, A.A., Doets, A.Y., Appeltshauser, L., Arends, S., Attarian, S., Benedetti, L., Briani, C., Casasnovas, C., et al. (2021). Guillain-Barre syndrome after SARS-CoV-2 infection in an international prospective cohort study. Brain 144, 3392-3404. Lunn, M.P., Carr, A.C., Keddie, S., Pakpoor, J., Pipis, M., and Willison, H.J. (2021). Reply: Guillain-Barre syndrome, SARS-CoV-2 and molecular mimicry and Ongoing challenges in unravelling the association between COVID-19 and Guillain-Barre syndrome and Unclear association between COVID-19 and Guillain-Barre syndrome and Currently available data regarding the potential association between COVID-19 and Guillain-Barre syndrome. Brain 144, e47. Margeta, M. (2020a). Autophagy defects in skeletal myopathies. Annu Rev Pathol 15, 261-285. Margeta, M. (2020b). Top ten discoveries of the year: Neuromuscular disease. Free Neuropathol 1, 4. Margeta, M. (2021). Neuromuscular disease: 2021 update. Free Neuropathol 2, 3. Meena, N.K., Ralston, E., Raben, N., and Puertollano, R. (2020). Enzyme replacement therapy can reverse pathogenic cascade in Pompe disease. Mol Ther Methods Clin Dev 18, 199-214. Napolitano, F., Terracciano, C., Bruno, G., De Blasiis, P., Lombardi, L., Gialluisi, A., Gianfrancesco, F., De Giovanni, D., Tummolo, A., Di Iorio, G., et al. (2021). Novel autophagic vacuolar myopathies: Phenotype and genotype features. Neuropathol Appl Neurobiol 47, 664-678. Pagnamenta, A.T., Kaiyrzhanov, R., Zou, Y., Da'as, S.I., Maroofian, R., Donkervoort, S., Dominik, N., Lauffer, M., Ferla, M.P., Orioli, A., et al. (2021). An ancestral 10-bp repeat expansion in VWA1 causes recessive hereditary motor neuropathy. Brain 144, 584-600. Patone, M., Handunnetthi, L., Saatci, D., Pan, J., Katikireddi, S.V., Razvi, S., Hunt, D., Mei, X.W., Dixon, S., Zaccardi, F., et al. (2021). Neurological complications after first dose of COVID-19 vaccines and SARS-CoV-2 infection. Nat Med 27, 2144-2153. Popovic, D., and Dikic, I. (2014). TBC1D5 and the AP2 complex regulate ATG9 trafficking and initiation of autophagy. EMBO Rep 15, 392-401. Puertollano, R., and Raben, N. (2021). New therapies for Pompe disease: are we closer to a cure? Lancet Neurol 20, 973-975. Quarta, M., Cromie, M., Chacon, R., Blonigan, J., Garcia, V., Akimenko, I., Hamer, M., Paine, P., Stok, M., Shrager, J.B., et al. (2017). Bioengineered constructs combined with exercise enhance stem cell-mediated treatment of volumetric muscle loss. Nat Commun 8, 15613. Ratnayake, D., Nguyen, P.D., Rossello, F.J., Wimmer, V.C., Tan, J.L., Galvis, L.A., Julier, Z., Wood, A.J., Boudier, T., Isiaku, A.I., et al. (2021). Macrophages provide a transient muscle stem cell niche via NAMPT secretion. Nature 591, 281-287. Salzer-Sheelo, L., Fellner, A., Orenstein, N., Bazak, L., Lev-El Halabi, N., Daue, M., Smirin-Yosef, P., Van Hout, C.V., Fellig, Y., Ruhrman-Shahar, N., et al. (2021). Biallelic truncating variants in the muscular A-type lamin-interacting protein (MLIP) gene cause myopathy with hyperCKemia. Eur J Neurol, ePub ahead of print. Schoser, B., Roberts, M., Byrne, B.J., Sitaraman, S., Jiang, H., Laforet, P., Toscano, A., Castelli, J., Diaz-Manera, J., Goldman, M., et al. (2021). Safety and efficacy of cipaglucosidase alfa plus miglustat versus alglucosidase alfa plus placebo in late-onset Pompe disease (PROPEL): an international, randomised, double-blind, parallel-group, phase 3 trial. Lancet Neurol 20, 1027-1037. Sicari, B.M., Agrawal, V., Siu, B.F., Medberry, C.J., Dearth, C.L., Turner, N.J., and Badylak, S.F. (2012). A murine model of volumetric muscle loss and a regenerative medicine approach for tissue replacement. Tissue Eng Part A 18, 1941-1948. Siegert, E., Uruha, A., Goebel, H.H., Preusse, C., Casteleyn, V., Kleefeld, F., Alten, R., Burmester, G.R., Schneider, U., Hoppner, J., et al. (2021). Systemic sclerosis-associated myositis features minimal inflammation and characteristic capillary pathology. Acta Neuropathol 141, 917-927. Spaulding, E.L., Hines, T.J., Bais, P., Tadenev, A.L.D., Schneider, R., Jewett, D., Pattavina, B., Pratt, S.L., Morelli, K.H., Stum, M.G., et al. (2021). The integrated stress response contributes to tRNA synthetase-associated peripheral neuropathy. Science 373, 1156-1161. Stavrou, M., Sargiannidou, I., Christofi, T., and Kleopa, K.A. (2021). Genetic mechanisms of peripheral nerve disease. Neurosci Lett 742, 135357. Stenton, S.L., Sheremet, N.L., Catarino, C.B., Andreeva, N.A., Assouline, Z., Barboni, P., Barel, O., Berutti, R., Bychkov, I., Caporali, L., et al. (2021). Impaired complex I repair causes recessive Leber’s hereditary optic neuropathy. J Clin Invest 131, e138267. Suh, J., Mukerji, S.S., Collens, S.I., Padera, R.F., Jr., Pinkus, G.S., Amato, A.A., and Solomon, I.H. (2021). Skeletal muscle and peripheral nerve histopathology in COVID-19. Neurology 97, e849-e858. Szczepanowska, K., Senft, K., Heidler, J., Herholz, M., Kukat, A., Hohne, M.N., Hofsetz, E., Becker, C., Kaspar, S., Giese, H., et al. (2020). A salvage pathway maintains highly functional respiratory complex I. Nat Commun 11, 1643. Tebbenkamp, A.T.N., Varela, L., Choi, J., Paredes, M.I., Giani, A.M., Song, J.E., Sestan-Pesa, M., Franjic, D., Sousa, A.M.M., Liu, Z.W., et al. (2018). The 7q11.23 protein DNAJC30 interacts with ATP synthase and links mitochondria to brain development. Cell 175, 1088-1104 e1023. Trikamji, B., and Pestronk, A. (2021). Treatable, motor-sensory, axonal neuropathies with C5b-9 complement on endoneurial microvessels. Muscle Nerve 63, 506-515. Turnbull, C., Scott, R.H., Thomas, E., Jones, L., Murugaesu, N., Pretty, F.B., Halai, D., Baple, E., Craig, C., Hamblin, A., et al. (2018). The 100 000 Genomes Project: bringing whole genome sequencing to the NHS. BMJ 361, k1687. Umapathi, T., Er, B., Koh, J.S., Goh, Y.H., and Chua, L. (2021). Guillain-Barre syndrome decreases in Singapore during the COVID-19 pandemic. J Peripher Nerv Syst 26, 235-236. Witt, L.J., Curran, J.J., and Strek, M.E. (2016). The diagnosis and treatment of antisynthetase syndrome. Clin Pulm Med 23, 218-226. Xi, Y., Ju, R., and Wang, Y. (2020). Roles of Annexin A protein family in autophagy regulation and therapy. Biomed Pharmacother 130, 110591. Yell, P.C., Burns, D.K., Dittmar, E.G., White, C.L., 3rd, and Cai, C. (2018). Diffuse microvascular C5b-9 deposition is a common feature in muscle and nerve biopsies from diabetic patients. Acta Neuropathol Commun 6, 11. Zhang, H., Zhou, Z.W., and Sun, L. (2021). Aminoacyl-tRNA synthetases in Charcot-Marie-Tooth disease: A gain or a loss? J Neurochem 157, 351-369. Zhang, K., Liu, Q., Liu, K., Shen, D., Tai, H., Shu, S., Ding, Q., Fu, H., Liu, S., Wang, Z., et al. (2018). ANXA11 mutations prevail in Chinese ALS patients with and without cognitive dementia. Neurol Genet 4, e237. Zuko, A., Mallik, M., Thompson, R., Spaulding, E.L., Wienand, A.R., Been, M., Tadenev, A.L.D., van Bakel, N., Sijlmans, C., Santos, L.A., et al. (2021). tRNA overexpression rescues peripheral neuropathy caused by mutations in tRNA synthetase. Science 373, 1161-1166.
Copyright: © 2022 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |