|
|
|
Free Neuropathology 3:3 (2022) |
|
Review |
|
Neuroinflammation: 2022 update |
|
Hans Lassmann1 |
|
1 Center for Brain Research, Medical University of Vienna, Austria |
|
Address for correspondence: |
|
Submitted: 20 January 2022 Accepted: 08 February 2022 Copyedited by: Shino Magaki Published: 10 February 2022 |
|
Keywords: COVID-19, Multiple sclerosis, Alzheimer’s disease, Microglia, Neurodegeneration |
|
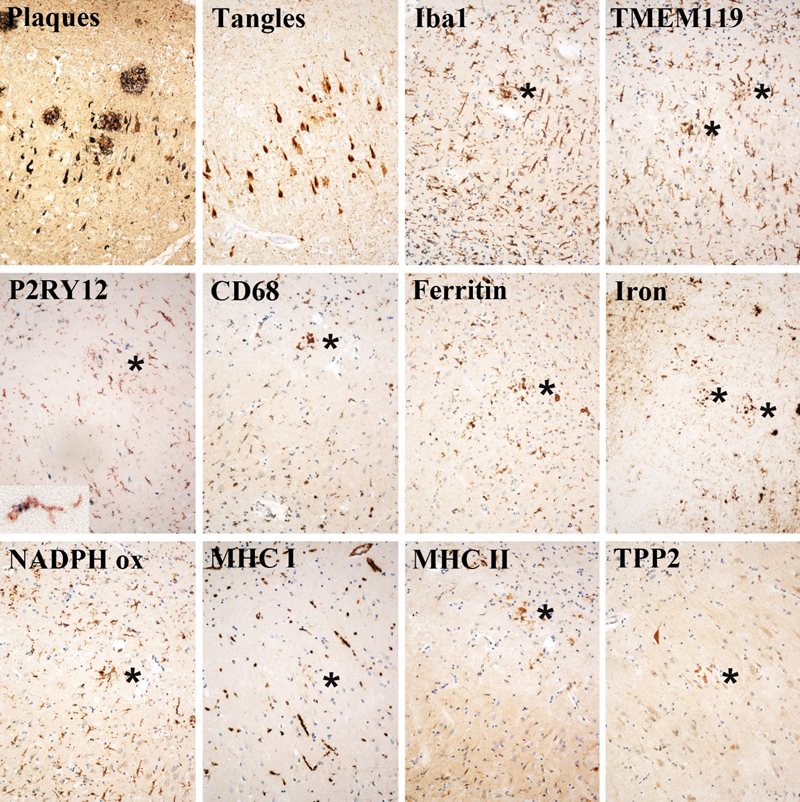
Abstract Besides important progress in the understanding of the pathological substrate of COVID-19-associated brain disease, major insights into mechanisms of neurodegeneration in human disease have been provided in neuropathological studies published in 2021. Recently developed techniques, which allow the simultaneous detection of a large battery of different molecules within single cells, have proven useful in the analysis of disease mechanisms in experimental and human neuroinflammatory conditions. They have elucidated protective and detrimental effects of activated microglia, which act in a stage and context-dependent manner in the induction and propagation of neurodegeneration. In addition, they emphasize the importance of synaptic damage and of selective neuronal vulnerability in the respective diseases. The results provide important new insights with high clinical relevance. Introduction Many manuscripts published in 2021 focused on neuropathological aspects of brain diseases, and it is thus difficult to select studies for a review article providing an update on their immunopathology. The manuscripts were identified by the frequent screening of the journals of neuropathology, neuroimmunology and clinical neurology, supplemented by the search for articles in PubMed, dealing with immunopathology of human diseases. Obviously, all aspects related to the COVID-19 pandemic raised major attention, and key elements of this work deserve to be presented here. In addition, I have focused this year mainly on aspects of neurodegeneration, which not only describe a specific feature in a single disease, but have relevance for a broad spectrum of different disorders. COVID-19 and the brain Not quite unexpected, a major focus in neuropathological research in 2021 focused on the changes in the central nervous system (CNS) present in patients with COVID-19. Insight into the nature of the respective damage in the nervous system is of critical importance to develop strategies to prevent neurological disease complications. In addition, it may provide a new understanding of the pathogenetic substrate of the Long COVID Syndrome. Consensus was reached during 2021 that two different pathologies dominate in patients who died in the course of COVID-19: vascular hypoxic/ischemic brain lesions and global microglia activation (Matschke et al. 2020, Maiese et al. 2021, Pajo et al. 2021, Al-Sarraj et al. 2021). Vascular pathology included endotheliitis, associated with a variable degree of focal ischemic or hemorrhagic lesions and diffuse or focal hypoxic alterations of neurons and glia (Thakur et al. 2021, Lee et al. 2021, Fabbri et al. 2021). Microglia activation was most prominent in the brain stem and the hippocampus. It consisted of a diffuse increase of microglia density with cellular activation and the appearance of microglia nodules (Thakur et al. 2021, Maiese et al. 2021). Overall, neither the vascular changes nor the patterns of microglia activation are considered specific for SARS-CoV-2 infection, but can also be found in other virus infections of the CNS, in conditions of systemic immune activation or sepsis and in patients dying in intensive care units (Thakur et al. 2021, Al-Sarraj et al. 2021). Thus, systemic cytokine storm in the course of the disease together with episodes of general hypoxia or metabolic derangement are likely to be at least in part responsible for the respective damage in the nervous system. Since the mean age of the patients in the larger autopsy series was beyond seventy years, it was not a surprise that about half of them exhibited pathologies related to age-related neurodegenerative diseases. All these pathological changes are also in line with the overall clinical appearance of neurological complications of COVID-19 (Thakur et al. 2021). The prevalence and potential role of direct SARS-CoV-2 infection in the CNS is still controversial (Al-Sarraj et al. 2021). In the majority of cases no virus RNA or antigen in the CNS has been detected, and when it was present, the virus titers were low even in cases with persistent active infection in the respiratory organs (Maiese et al. 2021, Thakur et al. 2021, Fabbri et al. 2021). This, however, does not exclude a transient endothelial infection, which triggers endotheliitis and vascular occlusion at early lesion stages (Kirschenbaum et al. 2021, Nalugo et al. 2021). Another potential route of virus invasion of the brain may occur through the olfactory system. However, a recent very systematic analysis of experimental and clinical data on this topic came to the conclusion that brain infection via olfactory nerves and a trans-neuronal spreading of infection through the olfactory system is unlikely (Butowt et al. 2021). Yet, neuronal spread of the virus by retrograde axonal transport in sensory nerves from the infected mucosa is still an option in some cases. Importantly, this study also pinpoints to the limits of experimental research in this topic, since those models, which mimic human disease best, are induced in animal species, which are only poorly suitable for currently available immunological and molecular research tools (Butowt et al. 2021). An important question is whether structural brain damage in the disease course of COVID-19 could in part explain long-term sequelae of the disease (Long COVID; Baig 2021). Ischemic changes and microglial activation were seen in 40% and 80% of brains, respectively. However, only 17% of these patients had neurological manifestations that were severe enough to involve a neurological consultant during life (Thakur et al. 2021). This suggests that brain damage in the course of COVID-19 is more frequent and widespread than reflected in clinically overt neurological disease. This is in line with the results of a very large clinical study on a cohort of more than 10,000 COVID-19 patients from the Philippines, which describes a high prevalence of mild neurological deficits (Espiritu et al. 2021). Clinically, mild cognitive impairment, encephalopathy and cerebrovascular disease were the most common manifestations. The high incidence of microglia activation in the hippocampus and brain stem may be related to neuropsychiatric symptoms in COVID-19 survivors, including memory disturbances, somnolence and fatigue (Thakur et al. 2021). The immunopathology of the COVID-19 brain The studies discussed above describe the basic neuropathology of the central nervous system of patients with COVID-19, but they have not addressed the phenotype of the immune reaction within the brain, and its relation to a possible infection with SARS-CoV-2. This gap has recently been filled by a broad and systematic study, which was performed on a large sample of brain autopsies from COVID-19 patients, in comparison to patients who died in intensive care units under conditions of respiratory distress or to patients with multiple sclerosis (Schwabenland et al. 2021). The study used imaging mass spectrometry, which allows simultaneous detection of multiple antigens, their spatial distribution in relation to lesion architecture and their vicinity to other immune or resident cells within the tissue. Searching for SARS-CoV-2 antigen within the brain tissue, the study reached similar conclusions, as described above, by showing only sparse virus antigen in the central nervous system. When present, it was mainly seen in endothelial cells of cerebral vessels. Displaying leukocyte-related molecules revealed a remarkable inflammatory reaction in the brain. It was characterized by cell clusters, representing different stages of microglia activation and perivascular myeloid cells recruited from the circulation. Most profound pro-inflammatory microglia activation was seen in the microglia nodules. Microglia and myeloid cell activation was associated with infiltration of the tissue by T-lymphocytes with a dominance of CD8+ cells, but a very low number of B-cells and plasma cells. In comparison to other diseases, neuroinflammation was more pronounced than in patients who died in intensive care units under respiratory distress only, but the inflammatory reaction in patients with multiple sclerosis was much more severe. Considering the immensely rich spectrum of immunological details described in this study, a number of conclusions have been reached. There is apparent evidence for a SARS-CoV-2 infection in the vessel walls, in particular affecting endothelial cells, and this is associated with a perivascular inflammatory reaction with blood brain barrier damage, mainly composed of CD8+ T-lymphocytes and recruited myeloid cells. However, in contrast to other previous studies thrombotic changes in inflamed vessels were absent. The inflammatory process concurred with global microglia activation and the formation of microglia nodules. The latter were the sites for most intense microglia activation and within the nodules CD8+ T-cells closely interacted with activated microglia, possibly providing pro-inflammatory as well as immunoregulatory signals. Whether such microglia nodules are a secondary phenomenon of the profound inflammatory reaction in the tissue or drive the inflammation through (virus) antigen recognition remains unresolved. Analysis of virus antigen expression did not provide evidence for virus entry into the brain through retrograde axonal transport from mucosal sites or through olfactory nerves. Despite the ground-breaking nature of this study, there are still a number of limitations. The major open question relates to the mechanisms of microglia activation. Although the authors did not find positive evidence, a potential role of direct SARS-CoV-2 infection in the brain tissue is not completely excluded. To finally prove or disprove a neuronal transport of virus into the brain and its direct role in microglia activation and neurodegeneration, the analysis of much earlier stages in the infectious process, disease stages which are rarely encountered in human autopsies, may be required. Similarly, a final view on similarities and differences of the inflammatory process between COVID-19 and multiple sclerosis requires the analysis of much larger numbers of samples from different disease and lesion stages. Finally, there are still some technical issues which have to be resolved in the future. The technology used here depicts phenotypic cell clusters, but whether these separations are functionally meaningful has yet to be shown. Furthermore, when the expression profiles of the different markers in imaging mass spectrometry, as shown for instance in the supplementary Figure 3B in this study, are compared with the experience obtained during the last decades with conventional immunocytochemistry, there are some obvious discrepancies, which raise some questions regarding specificity controls for each individual marker used in the imaging mass spectrometry panel. Selective vulnerability of neuron subpopulations in inflammatory or demyelinating conditions Acute and partially reversible neurological deficit is a common feature of inflammatory brain diseases. This can be mediated through disturbance of electrical conduction or through demyelination or synaptic loss, and can be compensated by remyelination or synaptic plasticity. In contrast, neuronal damage and loss is the prime substrate of permanent and irreversible neurological deficit. An interesting but controversial issue is whether there is a selective vulnerability of certain neuronal subpopulations, and when this is the case, what its mechanisms and consequences are. As an example, in cortical lesions in multiple sclerosis (MS) several groups have provided evidence that the GABAergic interneurons are prime targets for neurodegeneration (Dutta et al. 2006, Clements et al. 2008), while in another study a predominant degeneration of CUX2 positive excitatory neurons was observed and GABAergic interneurons were unaffected (Schirmer et al. 2019). These contradicting data need to be resolved. Two large and very well-performed studies have re-addressed the question of selective vulnerability of cortical neurons in inflammatory demyelinating disease in 2021, and both came to the conclusion that the specific subpopulation of GABAergic parvalbumin-containing inhibitory interneurons is lost preferentially in the MS cortex (Magliozzi et al. 2021, Zoupi et al. 2021). This is in agreement with previous human and experimental studies, which also showed a preferential loss of parvalbumin positive interneurons in autoimmune encephalomyelitis and in toxic demyelination (Falco et al. 2014, Lapato et al. 2017). Importantly, the loss of these neurons was associated with a significant and selective reduction of GABAergic presynaptic terminals in the cortex (Zoupi et al. 2021). In an attempt to clarify the underlying mechanisms, the authors also analyzed an experimental rodent model with focal primary cortical demyelination, induced by a chronic application of a lysolecithin-containing hydrogel. The authors conclude that demyelination triggers the loss of these particular neurons, and this may be related to their particular features of axonal myelination (Zoupi et al. 2021). In the other study (Magliozzi et al. 2021) it was shown that the extent of loss of parvalbumin-containing neurons correlated with the extent of meningeal inflammation. Since meningeal inflammation also determines the extent of cortical demyelination in MS lesions, demyelination may be the driving force of neurodegeneration also in this study. The observation that parvalbumin (PV) containing interneurons are preferentially destroyed in inflammatory and/or demyelinating diseases has clinical implications. Parvalbumin is liberated during cell death and reaches the cerebrospinal fluid, where it may serve as a paraclinical marker for active neurodegeneration (Magliozzi et al. 2021). Furthermore, loss of GABAergic interneurons in the course of inflammatory demyelination results in an altered excitatory/inhibitory balance, clinically manifested by epileptic seizures (Potter et al. 2016, Lapato et al. 2017). Thus, the selective vulnerability of inhibitory interneurons may be one of the explanations for the occurrence of epileptic seizures in multiple sclerosis and other inflammatory brain diseases (Koch et al. 2008, Nicholas et al. 2016, Langenbruch et al. 2019). Loss of GABAergic interneurons involves complement and results in specific brain region dependent functional consequences A similar selective loss of GABAergic interneurons was observed in the hippocampus of multiple sclerosis patients, mainly affecting the CA2 subfield. In line with the results discussed above this was also associated with an even more prominent loss of GABAergic synaptic terminals. Since excitatory glutamatergic terminals were unaffected, a dysbalance between excitatory and inhibitory synaptic input was noted (Ramaglia et al. 2021). Essentially similar findings were obtained in the demyelinated hippocampus in the rodent cuprizone model (Ramaglia et al. 2021). This allowed a detailed analysis of neurobiological mechanisms of neurodegeneration and its functional consequences. Synaptic degeneration was associated with profound precipitation of the complement component C1q, which significantly correlated with synaptic pathology and the extent of demyelination, but was not associated with the presence of pathogenic autoantibodies. A key role of complement in synaptic plasticity and degeneration has been observed in a variety of studies before (Schartz and Tenner 2020). Early complement components, such as C1q or C3, are produced in part in neurons and their production is enhanced in conditions of neurodegeneration. These proteins are transported in the axons to the terminals and focally accumulate at sites of axonal or synaptic damage (Michailidou et al. 2016). Their removal by microglia is a prerequisite for synaptic plasticity and axonal regeneration. In pathological conditions this mechanism is enhanced (Michailidou et al. 2016) and the subsequent complement/microglia interaction may result in substantial axonal and synaptic loss, followed by retrograde neuronal degeneration (Schartz and Tenner 2020). The neurophysiological consequences of the loss of GABAergic interneurons and synapses in the CA2 region was a disturbance of the excitatory/inhibitor balance and a loss of feed-forward inhibition of pyramidal neurons. In concomitant behavioral investigations it turned out that these functional changes were mainly reflected in a disturbance of social memory tasks, which were not accompanied by a general learning impairment or by changes of motor activities (Ramaglia et al. 2021). In summary, this study, too, shows a selective vulnerability of GABAergic interneurons in MS and cuprizone lesions and suggests that these changes are a potential consequence of demyelination. However, no loss of PV-containing GABAergic interneurons has been seen in another study in hippocampal MS lesions despite extensive demyelination (Kiljan et al. 2019), suggesting that demyelination alone is unlikely to be responsible. A similar preferential loss of parvalbumin reactive neurons has also been seen in a mouse model of autoimmune encephalomyelitis, which is driven by inflammation, but largely lacks primary demyelination in the cortex (Falco et al. 2014). Furthermore, hypoxic/ischemic damage is associated with a preferential loss of PV-containing GABAergic interneurons (Fowke et al. 2018, Stolp et al. 2019, Vaes et al. 2020, Povysheva et al. 2019) and a similar selective vulnerability has also been observed in a mouse model of Alzheimer’s disease (Petrache et al. 2019) Thus, the key question arises whether there are common mechanisms of brain injury shared between these different conditions. All of these conditions are associated with microglia activation, reflected by the expression of NADPH oxidase in activated microglia (Zrzavy et al. 2017, 2018). The beneficial effect of its pharmacological blockade indicates a role of oxidative injury in the induction of neuronal damage (Yuan et al. 2015) by mitochondrial injury and subsequent energy deficiency (Mahad et al. 2015). In such a state of “virtual hypoxia” (Dutta et al. 2013) additional demyelination amplifies damage due to the increased energy demand of denuded axons. Microglia phenotype in relation to Alzheimer’s disease (AD) pathology Research performed during the last decade brought microglia into a central position in the cascade of events triggering neurodegeneration. In Alzheimer’s disease the concept was originally proposed following the observation that activated microglia cumulate in amyloid plaques (McGeer et al. 1988) and that a variety of different pro-inflammatory cytokines and mediators are expressed in the AD cortex (Eikelenboom and Stam 1982, McGeer et al. 1988, Dickson and Rogers 1992). More recently, systematic genome wide association studies (GWAS) identified numerous risk genes for AD susceptibility, and many of these genes code for molecules involved in microglia function (Lambert et al. 2013, Lewcock et al. 2020). These results encouraged new studies on the phenotype of microglia in Alzheimer’s disease using the new opportunities offered by single cell transcriptomics and proteomics (Mathys et al. 2019, Lewcock et al. 2020). This allowed the identification of a disease-associated microglia phenotype (DAM), which was characterized by the loss of homeostatic phenotypic markers and the expression of a large array of different activation markers (Figure 1).
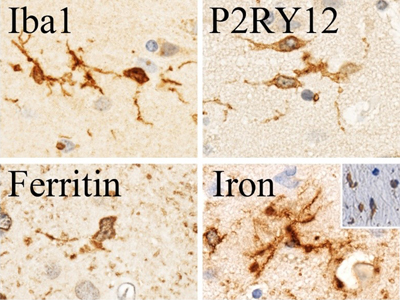
Figure 1: Microglia activation in Alzheimer’s disease: Microglia in the cortex of AD patients are activated within the amyloid plaques and also in surrounding cortical parenchyma. Within the plaques (labeled with *) the activation is more advanced showing an ameboid microglia phenotype and a higher expression of markers associated with phagocytosis (CD68), antigen presentation (MHC), oxidative injury (NADPH oxidase and iron storage (ferritin, iron)), and proteolysis (TPP2). A key step in this activation is the induction of the Trem2/ApoE pathway, which occurs in response to programed neuronal cell death (Krasemann et al. 2017). A variety of different molecules, identified by GWAS in AD patients, are related to this pathway, and loss of function mutations of Trem2 are associated with earlier onset and more severe disease. Functional studies revealed that loss of Trem2 function arrests microglia in a homeostatic state, reduces phagocytosis and inhibits the focal stabilization of Aβ deposits (Lewcock et al. 2020). All these data support the view that activated microglia within plaques play a neuroprotective role by inhibiting the spread of soluble Aβ oligomers. However, microglia in the AD cortex are also activated outside of Aβ plaques, where they are also associated with degeneration and loss of neurons and synapses. Whether these microglia cells have other activation profiles compared to the plaque-associated microglia has been addressed in a recent systematic study using single nuclei transcriptomics (Gerrits et al. 2021). The authors confirmed the phenotype of the plaque-associated microglia. In addition, however, they identified several new phenotypic microglia clusters, which were associated with the severity of cortical tau-pathology. This shows for the first time that the activation patterns of microglia are heterogeneous in the AD cortex in a context-dependent manner. These data indicate that tau-related neurodegeneration is triggered or associated with microglia activation steps, which differ from those responsible for their protective role in plaques. Only a minority of the molecules identified in these neurodegeneration-associated clusters are so far functionally characterized, some of them, however, seem to be related to mechanisms of tissue plasticity and repair. Thus, the final role of this new neurodegeneration-associated microglia phenotype is currently unresolved. Despite the highly innovative approach of recent studies using single cell transcriptomics and proteomics, such studies have major limitations. They identify a large battery of cluster-associated molecules, but only a small fraction of them is functionally defined at the present time. Their functional characterization has to be performed in experimental models, but this approach has limitations. Although basic activation steps of microglia are similar between different species, there are major differences in the molecular phenotypes of activated microglia between rodents and humans (Wimmer et al. 2018), and further differences in their patterns of activation are seen in human disease in comparison to those in AD models (Sobue et al. 2021). Another problem is related to the annotation of specific molecules to specific cell types. As an example, molecules of the NADPH oxidase complex, which are prominently expressed in human microglia and are clearly associated with oxidative injury in a variety of different diseases (Fischer et al. 2012), are surprisingly absent from the microglia activation list in recent single cells transcriptomic studies. Why this is the case is not clear. It may be that these molecules are not included in the list of microglia genes, since they are prominently expressed in granulocytes and thus annotated as granulocyte markers. The other possibility is that they are not included, since the gene lists have originally been defined in mouse models, and NADPH oxidase, in contrast to humans, is not prominently expressed in mouse microglia. Protective or detrimental action of microglia in Alzheimer’s disease: Context or lesion stage dependent? As discussed above, heterogeneous clusters of activated microglia are prominent in the AD cortex and they are associated with deposits of Aβ in the plaques (Lewcock et al. 2020). Whether activated microglia promote or ameliorate disease is unclear and can only partly be addressed in humans. The identification of Trem2 loss of function mutations as risk genes in AD suggests that microglia activation is protective by inhibiting Aβ spread into the cortical parenchyma. However, experimental models suggest a more complex role of microglia. Thus, microglia depletion before the onset of amyloid deposition in AD mouse models reduces plaque formation, possibly by inhibiting synapse degeneration, the liberation of amyloid precursor protein (APP) and its cleavage into Aβ fragments in the course of synapse degeneration (Delizannis et al. 2021). In addition, microglia seem to play a fundamentally different role in neurodegeneration in the AD brain. This was recently observed in transgenic mice expressing familial Alzheimer’s disease and human tau mutations (5xFAD/PS19 mice), in which tau tangles were precipitated by stereotactic seed injections of synthetic preformed tau fibrils into the hippocampus (Lodder et al. 2021). These animals developed severe Aβ plaque pathology in addition to profound tau-tangle pathology in the hippocampus and cerebral cortex, and both pathologies were associated with a disease-associated microglia phenotype (DAM). Microglia in the central nervous system can be depleted by chronic treatment of the animals with PLX 3397, a drug which selectively inhibits the colony stimulating factor 1 receptor (CSF1R). Interestingly, this treatment had a differential effect on plaque or tangle-associated microglia. While the diffuse microglia infiltration, which was associated with tau-pathology, was completely eliminated, the plaque-associated activated microglia was unaffected. This selective elimination of diffuse microglia in the cortical parenchyma resulted in a significant attenuation of the propagation of tau-pathology and neurodegeneration. From all these data one can conclude that microglia in the AD brain exert different functions, depending upon the stage of the cortical lesions and the nature of the damage. The initial stage of Aβ plaque formation is propagated, but the spread of mature plaques into the surrounding tissue is ameliorated by activated microglia. When there is a predisposition for tau phosphorylation, Aβ deposition propagates tau-tangles, and this process is further enhanced by activated microglia. This heterogenous scenario of microglia function in AD pathogenesis is a challenge for the development of anti-inflammatory treatment strategies. Iron and microglia in Alzheimer’s disease Microglia activation is seen in human AD as well as in mouse AD models and their basic activation pattern is similar, but not identical between these two conditions (Krasemann et al. 2017, Keren-Shaul et al. 2017, Mathys et al. 2019). Most importantly, most rodent models of AD differ from human disease in the absence or the extent of neurodegeneration. One difference between human and rodent neuropathology is the age-related accumulation of iron in the brain (Connor et al. 1992, Hametner et al. 2013), which is largely absent in rodents, at least at ages of the animals generally investigated in AD models. Iron accumulation in human microglia is increased in neurodegenerative diseases, and it is associated with a pro-inflammatory activation of the cells (Mehta et al. 2013, Hametner et al. 2013, van Duijn et al. 2017), possibly related to its pro-oxidative function. Furthermore, the phenotype of dystrophic microglia, present in human AD but largely absent in rodent models, is restricted to iron and ferritin-loaded cells (Lopes et al. 2008, Hametner et al. 2013; Figure 2).
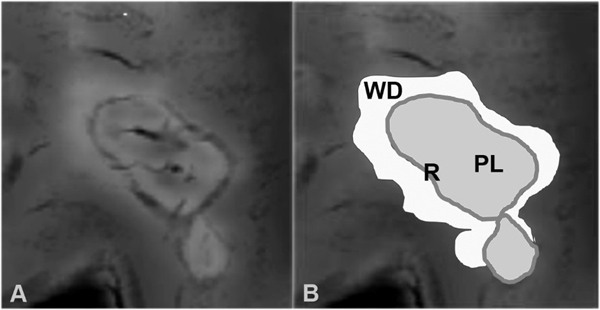
Figure 2: Iron accumulation and microglia senescence: Microglia, identified with the pan- microglia marker Iba1 in the cortex of AD patients may display a homeostatic phenotype, expressing P2RY12 and showing a normal ramification of their cell processes. Another fraction of microglia contains high levels of iron stored together with ferritin. These cells frequently show a dystrophic phenotype with loss and clumping of cell processes. The insert in the iron figure shows double staining for iron (brown) and the microglia/macrophage marker CD68 (blue). An important missing piece of knowledge was a detailed phenotypic and functional characterization of different microglia populations in the AD brain in relation to their iron content. This information is now provided by a recent study, describing the microglia activation profile in the cortex of AD patients using multispectral immunofluorescence (Kenkhuis et al. 2021). As described before, the study confirmed the increased microglia infiltration and activation in the AD cortex, the association of activated microglia with Aβ-plaques and the ferritin and iron accumulation in the microglia cytoplasm. Fine mapping of microglia was performed by cluster analysis. This revealed microglia clusters, which were mainly associated with AD lesions, and these clusters had in common the high ferritin content and the downregulation of various markers of the homeostatic microglia phenotype. The high ferritin content was associated with a phenotypic change of the cells towards dystrophic microglia. In contrast, microglia in the surrounding normal-appearing brain tissue were grouped in clusters with high or variable expression of homeostatic markers and low expression of ferritin. Thus, this study identifies disease-associated microglia through their iron and ferritin content. This was also reflected by the association of this microglia phenotype with disease severity, Apo-E genotype and the accumulation of Aβ plaques and neurofibrillary tangles in the brain. The major limitation of this study is the selection of AD cases, which is dominated by patients at later disease stage (Braak stage V to VI). Thus, it remains unclear whether iron accumulation and its binding to ferritin is a secondary phenomenon in the formation of Aβ plaques. Thus, iron uptake in microglia at the expense of microglia dystrophy may reflect removal of free iron from the extracellular space in an attempt to ameliorate oxidative injury. However, iron in microglia may activate microglia in a pro-inflammatory manner, which contributes to oxidative damage in the lesions. The iron content in the brain can be visualized and quantified in magnetic resonance imaging (MRI), using specific sequences such as R2* or quantitative susceptibility mapping (QSM) (Bulk et al. 2018). Using this technology, the authors also showed that the increased iron content in the sections is also correlated with an increased MRI signal (Kenkhuis et al. 2021). Dynamics of chronic microglia-associated neurodegeneration The possibility to detect accumulation of iron-loaded microglia in vivo by magnetic resonance imaging offers a very attractive tool to monitor the dynamics of active lesions and neurodegeneration in human disease. This is exemplified in multiple sclerosis, where the presence of an iron rim around the lesion identifies it as chronic active (Bagnato et al. 2011, Mehta et al. 2013, Hametner et al. 2013; Figure 3). Furthermore, such lesions show more pronounced tissue damage and neurodegeneration in comparison to those lacking an iron ring, and the presence of such lesions is associated with an aggressive clinical disease course (Absinta et al. 2016, Weber et al. 2021). Pathological data on the distribution of tissue degradation products in such iron lesions suggested that they expand very slowly, but the time course of their dynamic evolution was unknown. This has changed when prospective longitudinal MRI studies using iron sensitive sequences were performed, which provide data on dynamic changes in MS lesions over a time period of up to 7 years (Dal Bianco et al. 2017, 2021). Brain lesions without an iron rim shrank during the first 3 years and then their volume stabilized. In contrast, iron ring lesions slowly expanded over 3 to 5 years, before their size stabilized. These data indicate that chronic neurodegeneration in progressive multiple sclerosis is a very slow process, gradually developing over years, while demyelination and neurodegeneration in acute relapses develop within weeks.
Figure 3: Slowly expanding iron ring lesions in the MS brain can be visualized on MRI with iron sensitive imaging sequences. The typical presentation of such lesions reveals high iron signal in one or several central veins and in a rim at the lesion edge, reflecting iron-containing activated microglia. The iron rim (R) demarcates the demyelinated plaque (PL); the abnormal MRI signal around the iron rim is due to Wallerian Degeneration (WD). Direct neuropathological analysis of MRI scanned tissue blocks showed that the iron ring seen in MRI always reflects the iron-loaded microglia at the edge of active plaques, while the T2 signal of the lesions gradually expands outside the ring (Dal Bianco et al. 2017, 2021). These lesion changes reflect an expanding halo of secondary Wallerian degeneration around a destructive lesion (Figure 3). Thus, the quantitative lesion load, determined on MRI, not necessarily indicated lesion load, but also Wallerian degeneration in the normal appearing white matter. All these data highlight the importance of studies, directly correlating MRI changes with neuropathology and integrating this information into long term longitudinal prospective studies. It is expected that a similar approach will also provide significant new information for age-related neurodegenerative diseases. Is there evidence for involvement of T-cells in neurodegenerative disease? Neuropathological studies have provided evidence that cells of the adaptive immune system infiltrate the brain, in particular at sites of ongoing neurodegeneration in diseases such as Alzheimer’s disease or Parkinson’s disease (Togo et al. 2002, Brochard et al. 2009, Evans et al. 2019). These cells are mainly T-cells, including MHC Class II restricted CD4+ and MHC Class I restricted CD8+ cells. The key question, which is currently unresolved, is whether these cells actively contribute to tissue injury, are neuroprotective or are just passively recruited bystanders. This question has recently been addressed in an experimental model of Parkinson’s disease, induced by local injection of an adeno-associated virus vector, inducing the over-expression of α-synuclein in the substantia nigra of mice (Williams et al. 2021). In this model CD4+ and CD8+ T-cells infiltrate the midbrain, and this is associated with activation of myeloid cells, including microglia, and the degeneration and loss of tyrosine hydroxylase positive nigral neurons. The T-cell infiltrates are associated with the local expression of pro-inflammatory and in part also regulatory cytokines. Most importantly, T-cell receptor or CD4 deficient mice revealed a reduced activation of immune effector cells and also an ameliorated neurodegeneration in the substantia nigra. This study thus provides evidence that adaptive immune reactions, mainly mediated by MHC Class II restricted CD4+ T-cells, contribute to the propagation of neurodegeneration in this model. The results support the view that attempts to therapeutically modulate the T-cell immune response (Weiner et al. 2011, Mayo et al. 2016) could be effective. Direct support is provided by the observation that fingolimod, a drug which reduces the infiltration of immune cells into the central nervous system and is effective in the treatment of multiple sclerosis patients, ameliorates disease in the respective Parkinson’s disease model (Williams et al. 2021). Despite these findings, which suggest a pathogenic role of T-cells in Parkinson’s disease and other neurodegenerative diseases, it remains unresolved whether this is mediated by autoimmunity. No proof is provided that the T-cell immune reaction is directed against a specific autoantigen, such as for instance α-synuclein (Williams et al. 2021). Thus, local overexpression of α-synuclein may attract non-specifically T-cells into the brain. Since the normal immune repertoire contains T-cells against a variety of different brain auto-antigens (Wekerle et al. 1996), their activation in the lesions may just represent a non-specific consequence of the inflammatory response. Also, the mechanism of damage of neurons in the substantia nigra remains unresolved. Involvement of microglia and macrophages, which are activated by the T-cell mediated immune response, is likely to amplify neurodegeneration, but innate immunity alone will not specifically and selectively target dopaminergic neurons (Lassmann and van Horssen 2011). Finally, the amelioration of neuronal damage in animals treated with fingolimod does not necessarily prove immune mediated damage, since the modulation of sphingosine 1 phosphate receptors may also have direct neuroprotective effects (Colombo and Farina 2022). Thus, the study by Williams et al. (2021) supports a possible involvement of T-cell mediated mechanisms in neurodegeneration in Parkinson’s disease, but further research is necessary to clarify the underlying mechanisms. The local inflammatory response in gliomas: Good or bad or irrelevant? It is generally accepted that local inflammation is present in the malignant gliomas, but it is largely unresolved whether this is beneficial or detrimental for the patients (Jack and Lu 2015). Overall, there is an immunosuppressive environment within gliomas due to the production of anti-inflammatory cytokines, such as transforming growth factor β (TGF-β) in the tumor cells (Binnewies et al. 2018, Brown et al. 2018). The extent of TGF-β expression is, however, variable between patients and one expects that lower levels of immunosuppression is associated with inflammation, immune attack of tumor cells and good clinical prognosis in patients. Alternatively, high density of inflammatory cells within the tumor may be secondary to more aggressive tissue damage and associated with a less favorable prognosis. In addition, the inflammatory response itself may be dominated by pro-inflammatory activated cytotoxic effector cells or by regulatory T-cells and myeloid-derived suppressor cells, and this, too, may influence tumor progression and functional outcome (Kmiecik et al. 2013, 2014, Gabriely et al. 2017). Several studies have so far analyzed the phenotype of tumor-infiltrating inflammatory cells and its relation to clinical outcome, but the results are variable and in part contradictory (Charles et al. 2012, Szulzewsky et al. 2015, Orrego et al. 2018, Martinez et al. 2009, Zhang et al. 2019). This is mainly due to the fact that the studies were performed by immunocytochemistry, which does not allow the simultaneous analysis of a large spectrum of different immune cells. This problem was addressed in a recent study by applying flow cytometry of dissociated cells from a large number of biopsy samples from carefully characterized glioblastoma patients (Gonzales-Tablas Pimenta et al. 2021). By using novel state-of-the-art techniques of multi-antibody and multi-color labeling, a simultaneous quantitative evaluation of all different leukocyte populations was possible. As shown before, the study revealed that on average only a quarter of the total cell population were CD45+ immune cells, two thirds of them being tumor-associated macrophages of hematogenous or microglia origin and granulocytes. The lymphocyte population mainly consisted of MHC Class I restricted CD8+ and MHC Class II restricted CD4+ T-cells. The infiltration by regulatory T-cells, B-lymphocytes and natural killer cells (NK cells) was very low. Immunosuppressive cytokines, such as TGF-β and interleukin 10 (Il10) were mainly seen within tumor cells and in low incidence in myeloid derived suppressor cells. The broad spectrum of markers used simultaneously in this study allowed to define three patient clusters with distinct immune infiltration. In the first, immune cell infiltration was sparse and dominated by tumor-associated macrophages. In the second, the tissue infiltration was profound, but consisted mainly of myeloid cells with little contribution of lymphocytes. In the third, the immune infiltration, too, was high containing high amounts of tumor-associated macrophages, granulocytes and T-lymphocytes. The latter patient cohort showed a significantly worse clinical prognosis compared to the other groups. This study represents an important first step for a comprehensive characterization of the local immune response in gliomas in correlation to clinical prognosis and tumor genotype. This approach will also be essential to interpret the effects of new immunotherapies in gliomas. Conclusions Mechanisms of adaptive and innate immunity appear to be involved in the propagation of neurodegeneration in many different diseases, including inflammatory conditions such as multiple sclerosis or classical neurodegenerative disorders. These mechanisms can now be studied in a holistic approach with modern technologies of single cell transcriptomics and proteomics. Microglia plays a central role. Depending upon the type and stage of their activation they have beneficial or detrimental roles. The effects are in part reproduced in experimental animal models, but there are major differences in microglia function between humans and rodents. Importantly, microglia-associated neuronal damage results in a preferential vulnerability of GABAergic interneurons, which results in an altered excitatory/inhibitory balance and this may in part explain the association of brain inflammation with seizures. References Absinta M, Sati P, Schindler M, Leibovitch EC, Ohayon J, Wu T, Meani A, Filippi M, Jacobson S, Cortese IC, Reich DS. Persistent 7-tesla phase rim predicts poor outcome in new multiple sclerosis patient lesions. J Clin Invest. 2016;126:2597-2609. https://doi.org/10.1172/JCI86198 Epub 2016 Jun 6. PMID: 27270171; PMCID: PMC4922708. Al-Sarraj S, Troakes C, Hanley B, Osborn M, Richardson MP, Hotopf M, Bullmore E, Everall IP. Invited Review: The spectrum of neuropathology in COVID-19. Neuropathol Appl Neurobiol. 2021;47:3-16. https://doi.org/10.1111/nan.12667 Epub 2020 Oct 20. PMID: 32935873. Bagnato F, Hametner S, Yao B, van Gelderen P, Merkle H, Cantor FK, Lassmann H, Duyn JH. Tracking iron in multiple sclerosis: A combined imaging and histopathological study at 7 Tesla. Brain. 2011;134:3602-3615. https://doi.org/10.1093/brain/awr278 PMID: 22171355; PMCID: PMC3235560. Baig AM. Chronic long-COVID syndrome: A protracted COVID-19 illness with neurological dysfunctions. CNS Neurosci Ther. 2021;27:1433-1436. https://doi.org/10.1111/cns.13737 Epub 2021 Oct 9. PMID: 34626096; PMCID: PMC8611765. Binnewies M, Roberts EW, Kersten K, Chan V, Fearon DF, Merad M, Coussens LM, Gabrilovich DI, Ostrand-Rosenberg S, Hedrick CC, Vonderheide RH, Pittet MJ, Jain RK, Zou W, Howcroft TK, Woodhouse EC, Weinberg RA, Krummel, MF. Understanding the tumor immune microenvironment (TIME) for effective therapy. Nat Med. 2018;24:541–550. https://doi.org/10.1038/s41591-018-0014-x Epub 2018 Apr 23. PMID: 29686425; PMCID: PMC5998822 Brochard V, Combadière B, Prigent A, Laouar Y, Perrin A, Beray-Berthat V, Bonduelle O, Alvarez-Fischer D, Callebert J, Launay JM, Duyckaerts C, Flavell RA, Hirsch EC, Hunot S. Infiltration of CD4+ lymphocytes into the brain contributes to neurodegeneration in a mouse model of Parkinson disease. J Clin Invest. 2009;119:182-192. https://doi.org/10.1172/JCI36470 Epub 2008 Dec 22. PMID: 19104149; PMCID: PMC2613467. Brown NF, Carter TJ, Ottaviani D, Mulholland P. Harnessing the immune system in glioblastoma. Br J Cancer. 2018;119:1171–1181. https://doi.org/10.1038/s41416-018-0258-8 PMID: 30393372; PMCID: PMC6251037. Bulk M, Kenkhuis B, van der Graaf LM, Goeman JJ, Natté R, van der Weerd L.Postmortem T2*- weighted MRI imaging of cortical iron reflects severity of Alzheimer’s disease. J Alzheimers Dis. 2018;65:1125–1137. https://doi.org/10.3233/JAD-180317 PMID: 30103327; PMCID: PMC6218127. Butowt R, Meunier N, Bryche B, von Bartheld CS. The olfactory nerve is not a likely route to brain infection in COVID-19: A critical review of data from humans and animal models. Acta Neuropathol. 2021;141:809-822. https://doi.org/10.1007/s00401-021-02314-2 Epub 2021 Apr 26. PMID: 33903954; PMCID: PMC8075028. Charles NA, Holland EC, Gilbertson R, Glass R, Kettenmann H. The brain tumor microenvironment. Glia. 2012;60:502-514. https://doi.org/10.1002/glia.21264 PMID: 22379614. Clements RJ, McDonough J, Freeman EJ. Distribution of parvalbumin and calretinin immunoreactive interneurons in motor cortex from multiple sclerosis post-mortem tissue. Exp Brain Res. 2008;187:459-465. https://doi.org/10.1007/s00221-008-1317-9 Epub 2008 Feb 23. PMID: 18297277. Colombo E, Farina C. Lessons from S1P receptor targeting in multiple sclerosis. Pharmacol Ther. 2022;230:107971. https://doi.org/10.1016/j.pharmthera.2021.107971 Epub 2021 Aug 25. PMID: 34450231. Connor JR, Menzies SL, St. Martin SM, Mufson EJ. A histochemical study of iron, transferrin, and ferritin in Alzheimer’s diseased brains. J Neurosci Res. 1992;31:75–83. https://doi.org/10.1002/jnr.490310111 PMID: 1613823. Dal-Bianco A, Grabner G, Kronnerwetter C, Weber M, Höftberger R, Berger T, Auff E, Leutmezer F, Trattnig S, Lassmann H, Bagnato F, Hametner S. Slow expansion of multiple sclerosis iron rim lesions: Pathology and 7 T magnetic resonance imaging. Acta Neuropathol. 2017;133:25-42. https://doi.org/10.1007/s00401-016-1636-z Epub 2016 Oct 27. PMID: 27796537; PMCID: PMC5209400. Dal-Bianco A, Grabner G, Kronnerwetter C, Weber M, Kornek B, Kasprian G, Berger T, Leutmezer F, Rommer PS, Trattnig S, Lassmann H, Hametner S. Long-term evolution of multiple sclerosis iron rim lesions in 7 T MRI. Brain. 2021;144:833-847. https://doi.org/10.1093/brain/awaa436 PMID: 33484118. Delizannis AT, Nonneman A, Tsering W, De Bondt A, Van den Wyngaert I, Zhang B, Meymand E, Olufemi MF, Koivula P, Maimaiti S, Trojanowski JQ, Lee VM, Brunden KR. Effects of microglial depletion and TREM2 deficiency on Aβ plaque burden and neuritic plaque tau pathology in 5XFAD mice. Acta Neuropathol Commun. 2021;9:150. https://doi.org/10.1186/s40478-021-01251-1 PMID: 34503586; PMCID: PMC8428059. Dickson DW, Rogers J. Neuroimmunology of Alzheimer's disease: A conference report. Neurobiol Aging. 1992;13:793-798. https://doi.org/10.1016/0197-4580(92)90104-6 PMID: 1491745. Dutta R, Chomyk AM, Chang A, Ribaudo MV, Deckard SA, Doud MK, Edberg DD, Bai B, Li M, Baranzini SE, Fox RJ, Staugaitis SM, Macklin WB, Trapp BD. Hippocampal demyelination and memory dysfunction are associated with increased levels of the neuronal microRNA miR-124 and reduced AMPA receptors. Ann Neurol. 2013;73:637-645. https://doi.org/10.1002/ana.23860 Epub 2013 Apr 17. PMID: 23595422; PMCID: PMC3679350. Dutta R, McDonough J, Yin X, Peterson J, Chang A, Torres T, Gudz T, Macklin WB, Lewis DA, Fox RJ, Rudick R, Mirnics K, Trapp BD. Mitochondrial dysfunction as a cause of axonal degeneration in multiple sclerosis patients. Ann Neurol. 2006;59:478-489. https://doi.org/10.1002/ana.20736 PMID: 16392116. Eikelenboom P, Stam FC. Immunoglobulins and complement factors in senile plaques. An immunoperoxidase study. Acta Neuropathol. 1982;57:239-242. https://doi.org/10.1007/BF00685397 PMID: 6812382. Espiritu AI, Sy MCC, Anlacan VMM, Jamora RDG; Philippine CORONA Study Group Investigators. COVID-19 outcomes of 10,881 patients: Retrospective study of neurological symptoms and associated manifestations (Philippine CORONA Study). J Neural Transm (Vienna). 2021;128:1687-1703. https://doi.org/10.1007/s00702-021-02400-5 Epub 2021 Aug 27. PMID: 34448930; PMCID: PMC8391861. Evans FL, Dittmer M, de la Fuente AG, Fitzgerald DC. Protective and regenerative roles of T cells in central nervous system disorders. Front Immunol. 2019;10:2171. https://doi.org/10.3389/fimmu.2019.02171 PMID: 31572381; PMCID: PMC6751344. Fabbri VP, Foschini MP, Lazzarotto T, Gabrielli L, Cenacchi G, Gallo C, Aspide R, Frascaroli G, Cortelli P, Riefolo M, Giannini C, D'Errico A. Brain ischemic injury in COVID-19-infected patients: A series of 10 post-mortem cases. Brain Pathol. 2021;31:205-210. https://doi.org/10.1111/bpa.12901 Epub 2020 Nov 2. PMID: 33002281; PMCID: PMC7536900. Falco A, Pennucci R, Brambilla E, de Curtis I. Reduction in parvalbumin-positive interneurons and inhibitory input in the cortex of mice with experimental autoimmune encephalomyelitis. Exp Brain Res. 2014;232:2439-2449. https://doi.org/10.1007/s00221-014-3944-7 Epub 2014 Apr 26. PMID: 24770856; PMCID: PMC4055863. Fischer MT, Sharma R, Lim JL, Haider L, Frischer JM, Drexhage J, Mahad D, Bradl M, van Horssen J, Lassmann H. NADPH oxidase expression in active multiple sclerosis lesions in relation to oxidative tissue damage and mitochondrial injury. Brain. 2012;135:886-899. https://doi.org/10.1093/brain/aws012 PMID: 22366799; PMCID: PMC3286337. Fowke TM, Galinsky R, Davidson JO, Wassink G, Karunasinghe RN, Prasad JD, Bennet L, Gunn AJ, Dean JM. Loss of interneurons and disruption of perineuronal nets in the cerebral cortex following hypoxia-ischaemia in near-term fetal sheep. Sci Rep. 2018;8:17686. https://doi.org/10.1038/s41598-018-36083-y PMID: 30523273; PMCID: PMC6283845. Gabriely G, da Cunha AP, Rezende RM, Kenyon B, Madi A, Vandeventer T, Skillin N, Rubino S, Garo L, Mazzola MA, Kolypetri P, Lanser AJ, Moreira T, Faria AMC, Lassmann H, Kuchroo V, Murugaiyan G, Weiner HL. Targeting latency-associated peptide promotes antitumor immunity. Sci Immunol. 2017;2:eaaj1738. https://doi.org/10.1126/sciimmunol.aaj1738 PMID: 28763794; PMCID: PMC5657397. Gerrits E, Brouwer N, Kooistra SM, Woodbury ME, Vermeiren Y, Lambourne M, Mulder J, Kummer M, Möller T, Biber K, Dunnen WFAD, De Deyn PP, Eggen BJL, Boddeke EWGM. Distinct amyloid-β and tau-associated microglia profiles in Alzheimer's disease. Acta Neuropathol. 2021;141:681-696. https://doi.org/10.1007/s00401-021-02263-w Epub 2021 Feb 20. PMID: 33609158; PMCID: PMC8043951. González-Tablas Pimenta M, Otero Á, Arandia Guzman DA, Pascual-Argente D, Ruíz Martín L, Sousa-Casasnovas P, García-Martin A, Roa Montes de Oca JC, Villaseñor-Ledezma J, Torres Carretero L, Almeida M, Ortiz J, Nieto A, Orfao A, Tabernero MD. Tumor cell and immune cell profiles in primary human glioblastoma: Impact on patient outcome. Brain Pathol. 2021;31:365-380. https://doi.org/10.1111/bpa.12927 Epub 2021 Feb 13. PMID: 33314398; PMCID: PMC8018082. Hametner S, Wimmer I, Haider L, Pfeifenbring S, Brück W, Lassmann H. Iron and neurodegeneration in the multiple sclerosis brain. Ann Neurol. 2013;74:848-861. https://doi.org/10.1002/ana.23974 Epub 2013 Oct 7. PMID: 23868451; PMCID: PMC4223935. Jack AS, Lu J-Q. Immune cell infiltrates in the central nervous system tumors. Austin Neurosurg Open Access. 2015;2:1024. Kenkhuis B, Somarakis A, de Haan L, Dzyubachyk O, IJsselsteijn ME, de Miranda NFCC, Lelieveldt BPF, Dijkstra J, van Roon-Mom WMC, Höllt T, van der Weerd L. Iron loading is a prominent feature of activated microglia in Alzheimer's disease patients. Acta Neuropathol Commun. 2021;9:27. https://doi.org/10.1186/s40478-021-01126-5 PMID: 33597025; PMCID: PMC7887813. Keren-Shaul H, Spinrad A, Weiner A, Matcovitch-Natan O, Dvir-Szternfeld R, Ulland TK, David E, Baruch K, Lara-Astaiso D, Toth B, Itzkovitz S, Colonna M, Schwartz M, Amit I. A unique microglia type associated with restricting development of Alzheimer's disease. Cell. 2017;169:1276-1290.e17. https://doi.org/10.1016/j.cell.2017.05.018 Epub 2017 Jun 8. PMID: 28602351. Kiljan S, Prins M, Baselmans BM, Bol JGJM, Schenk GJ, van Dam AM. Enhanced GABAergic immunoreactivity in hippocampal neurons and astroglia of multiple sclerosis patients. J Neuropathol Exp Neurol. 2019;78:480-491. https://doi.org/10.1093/jnen/nlz028 PMID: 31100147; PMCID: PMC6524632. Kirschenbaum D, Imbach LL, Rushing EJ, Frauenknecht KBM, Gascho D, Ineichen BV, Keller E, Kohler S, Lichtblau M, Reimann RR, Schreib K, Ulrich S, Steiger P, Aguzzi A, Frontzek K. Intracerebral endotheliitis and microbleeds are neuropathological features of COVID-19. Neuropathol Appl Neurobiol. 2021;47:454-459. https://doi.org/10.1111/nan.12677 Epub 2020 Dec 14. PMID: 33249605; PMCID: PMC7753688. Kmiecik J, Poli A, Brons NHC, Waha A, Eide GE, Enger PØ, Zimmer J, Chekenya M. Elevated CD3+ and CD8+ tumor-infiltrating immune cells correlate with prolonged survival in glioblastoma patients despite integrated immunosuppressive mechanisms in the tumor microenvironment and at the systemic level. J Neuroimmunol. 2013;264:71–83. https://doi.org/10.1016/j.jneuroim.2013.08.013 Epub 2013 Aug 31. PMID: 24045166. Kmiecik J, Zimmer J, Chekenya M. Natural killer cells in intracranial neoplasms: Presence and therapeutic efficacy against brain tumours. J Neurooncol. 2014;116:1–9. https://doi.org/10.1007/s11060-013-1265-5 Epub 2013 Oct 2. PMID: 24085644; PMCID: PMC3889498. Koch M, Uyttenboogaart M, Polman S, De Keyser J. Seizures in multiple sclerosis. Epilepsia. 2008;49:948-953. https://doi.org/10.1111/j.1528-1167.2008.01565.x Epub 2008 Mar 11. PMID: 18336559. Krasemann S, Madore C, Cialic R, Baufeld C, Calcagno N, El Fatimy R, Beckers L, O'Loughlin E, Xu Y, Fanek Z, Greco DJ, Smith ST, Tweet G, Humulock Z, Zrzavy T, Conde-Sanroman P, Gacias M, Weng Z, Chen H, Tjon E, Mazaheri F, Hartmann K, Madi A, Ulrich JD, Glatzel M, Worthmann A, Heeren J, Budnik B, Lemere C, Ikezu T, Heppner FL, Litvak V, Holtzman DM, Lassmann H, Weiner HL, Ochando J, Haass C, Butovsky O. The TREM2-APOE pathway drives the transcriptional phenotype of dysfunctional microglia in neurodegenerative diseases. Immunity. 2017;47:566-581.e9. https://doi.org/10.1016/j.immuni.2017.08.008 PMID: 28930663; PMCID: PMC5719893. Lambert JC, Ibrahim-Verbaas CA, Harold D, Naj AC, Sims R, Bellenguez C, DeStafano AL, Bis JC, Beecham GW, Grenier-Boley B, Russo G, Thorton-Wells TA, Jones N, Smith AV, Chouraki V, Thomas C, Ikram MA, Zelenika D, Vardarajan BN, Kamatani Y, Lin CF, Gerrish A, Schmidt H, Kunkle B, Dunstan ML, Ruiz A, Bihoreau MT, Choi SH, Reitz C, Pasquier F, Cruchaga C, Craig D, Amin N, Berr C, Lopez OL, De Jager PL, Deramecourt V, Johnston JA, Evans D, Lovestone S, Letenneur L, Morón FJ, Rubinsztein DC, Eiriksdottir G, Sleegers K, Goate AM, Fiévet N, Huentelman MW, Gill M, Brown K, Kamboh MI, Keller L, Barberger-Gateau P, McGuiness B, Larson EB, Green R, Myers AJ, Dufouil C, Todd S, Wallon D, Love S, Rogaeva E, Gallacher J, St George-Hyslop P, Clarimon J, Lleo A, Bayer A, Tsuang DW, Yu L, Tsolaki M, Bossù P, Spalletta G, Proitsi P, Collinge J, Sorbi S, Sanchez-Garcia F, Fox NC, Hardy J, Deniz Naranjo MC, Bosco P, Clarke R, Brayne C, Galimberti D, Mancuso M, Matthews F; European Alzheimer's Disease Initiative (EADI); Genetic and Environmental Risk in Alzheimer's Disease; Alzheimer's Disease Genetic Consortium; Cohorts for Heart and Aging Research in Genomic Epidemiology, Moebus S, Mecocci P, Del Zompo M, Maier W, Hampel H, Pilotto A, Bullido M, Panza F, Caffarra P, Nacmias B, Gilbert JR, Mayhaus M, Lannefelt L, Hakonarson H, Pichler S, Carrasquillo MM, Ingelsson M, Beekly D, Alvarez V, Zou F, Valladares O, Younkin SG, Coto E, Hamilton-Nelson KL, Gu W, Razquin C, Pastor P, Mateo I, Owen MJ, Faber KM, Jonsson PV, Combarros O, O'Donovan MC, Cantwell LB, Soininen H, Blacker D, Mead S, Mosley TH Jr, Bennett DA, Harris TB, Fratiglioni L, Holmes C, de Bruijn RF, Passmore P, Montine TJ, Bettens K, Rotter JI, Brice A, Morgan K, Foroud TM, Kukull WA, Hannequin D, Powell JF, Nalls MA, Ritchie K, Lunetta KL, Kauwe JS, Boerwinkle E, Riemenschneider M, Boada M, Hiltuenen M, Martin ER, Schmidt R, Rujescu D, Wang LS, Dartigues JF, Mayeux R, Tzourio C, Hofman A, Nöthen MM, Graff C, Psaty BM, Jones L, Haines JL, Holmans PA, Lathrop M, Pericak-Vance MA, Launer LJ, Farrer LA, van Duijn CM, Van Broeckhoven C, Moskvina V, Seshadri S, Williams J, Schellenberg GD, Amouyel P. Meta-analysis of 74,046 individuals identifies 11 new susceptibility loci for Alzheimer’s disease. Nat Genet. 2013;45:1452–1458. https://doi.org/10.1038/ng.2802 Epub 2013 Oct 27. PMID: 24162737; PMCID: PMC3896259. Langenbruch L, Krämer J, Güler S, Möddel G, Geβner S, Melzer N, Elger CE, Wiendl H, Budde T, Meuth SG, Kovac S. Seizures and epilepsy in multiple sclerosis: Epidemiology and prognosis in a large tertiary referral center. J Neurol. 2019;266:1789-1795. https://doi.org/10.1007/s00415-019-09332-x Epub 2019 May 8. PMID: 31069528. Lapato AS, Szu JI, Hasselmann JPC, Khalaj AJ, Binder DK, Tiwari-Woodruff SK. Chronic demyelination-induced seizures. Neuroscience. 2017;346:409-422. https://doi.org/10.1016/j.neuroscience.2017.01.035 Epub 2017 Jan 30. PMID: 28153692; PMCID: PMC5394933. Lassmann H, van Horssen J. The molecular basis of neurodegeneration in multiple sclerosis. FEBS Lett. 2011;585:3715-3723. https://doi.org/10.1016/j.febslet.2011.08.004 Epub 2011 Aug 16. PMID: 21854776. Lee MH, Perl DP, Nair G, Li W, Maric D, Murray H, Dodd SJ, Koretsky AP, Watts JA, Cheung V, Masliah E, Horkayne-Szakaly I, Jones R, Stram MN, Moncur J, Hefti M, Folkerth RD, Nath A. Microvascular injury in the brains of patients with Covid-19. N Engl J Med. 2021;384:481-483. https://doi.org/10.1056/NEJMc2033369 Epub 2020 Dec 30. PMID: 33378608; PMCID: PMC7787217. Lewcock JW, Schlepckow K, Di Paolo G, Tahirovic S, Monroe KM, Haass C. Emerging microglia biology defines novel therapeutic approaches for Alzheimer's disease. Neuron. 2020;108:801-821. https://doi.org/10.1016/j.neuron.2020.09.029 Epub 2020 Oct 22. PMID: 33096024. Lodder C, Scheyltjens I, Stancu IC, Botella Lucena P, Gutiérrez de Ravé M, Vanherle S, Vanmierlo T, Cremers N, Vanrusselt H, Brône B, Hanseeuw B, Octave JN, Bottelbergs A, Movahedi K, Dewachter I. CSF1R inhibition rescues tau pathology and neurodegeneration in an A/T/N model with combined AD pathologies, while preserving plaque associated microglia. Acta Neuropathol Commun. 2021;9:108. https://doi.org/10.1186/s40478-021-01204-8 PMID: 34103079; PMCID: PMC8188790. Lopes KO, Sparks DL, Streit WJ. Microglial dystrophy in the aged and Alzheimer’s disease brain is associated with ferritin immunoreactivity. Glia. 2008;56:1048–1060. https://doi.org/10.1002/glia.20678 PMID: 18442088. Magliozzi R, Pitteri M, Ziccardi S, Pisani AI, Montibeller L, Marastoni D, Rossi S, Mazziotti V, Guandalini M, Dapor C, Schiavi G, Tamanti A, Nicholas R, Reynolds R, Calabrese M. CSF parvalbumin levels reflect interneuron loss linked with cortical pathology in multiple sclerosis. Ann Clin Transl Neurol. 2021;8:534-547. https://doi.org/10.1002/acn3.51298 Epub 2021 Jan 23. PMID: 33484486; PMCID: PMC7951111. Mahad DH, Trapp BD, Lassmann H. Pathological mechanisms in progressive multiple sclerosis. Lancet Neurol. 2015;14:183-193. https://doi.org/10.1016/S1474-4422(14)70256-X PMID: 25772897. Maiese A, Manetti AC, Bosetti C, Del Duca F, La Russa R, Frati P, Di Paolo M, Turillazzi E, Fineschi V. SARS-CoV-2 and the brain: A review of the current knowledge on neuropathology in COVID-19. Brain Pathol. 2021;31:e13013. https://doi.org/10.1111/bpa.13013 Epub 2021 Aug 13. PMID: 34390282; PMCID: PMC8420197. Martinez FO, Helming L, Gordon S. Alternative activation of macrophages: An immunologic functional perspective. Annu Rev Immunol. 2009;27:451–483. https://doi.org/10.1146/annurev.immunol.021908.132532 PMID: 19105661. Mathys H, Davila-Velderrain J, Peng Z, Gao F, Mohammadi S, Young JZ, Menon M, He L, Abdurrob F, Jiang X, Martorell AJ, Ransohoff RM, Hafler BP, Bennett DA, Kellis M, Tsai LH. Single-cell transcriptomic analysis of Alzheimer's disease. Nature. 2019;570:332-337. https://doi.org/10.1038/s41586-019-1195-2 Epub 2019 May 1. Erratum in: Nature. 2019;571:E1. PMID: 31042697; PMCID: PMC6865822. Matschke J, Lütgehetmann M, Hagel C, Sperhake JP, Schröder AS, Edler C, Mushumba H, Fitzek A, Allweiss L, Dandri M, Dottermusch M, Heinemann A, Pfefferle S, Schwabenland M, Sumner Magruder D, Bonn S, Prinz M, Gerloff C, Püschel K, Krasemann S, Aepfelbacher M, Glatzel M. Neuropathology of patients with COVID-19 in Germany: A post-mortem case series. Lancet Neurol. 2020;19:919-929. https://doi.org/10.1016/S1474-4422(20)30308-2 Epub 2020 Oct 5. PMID: 33031735; PMCID: PMC7535629. Mayo L, Cunha AP, Madi A, Beynon V, Yang Z, Alvarez JI, Prat A, Sobel RA, Kobzik L, Lassmann H, Quintana FJ, Weiner HL. IL-10-dependent Tr1 cells attenuate astrocyte activation and ameliorate chronic central nervous system inflammation. Brain. 2016;139:1939-1957. https://doi.org/10.1093/brain/aww113 Epub 2016 May 31. PMID: 27246324; PMCID: PMC4939696. McGeer PL, Itagaki S, McGeer EG. Expression of the histocompatibility glycoprotein HLA-DR in neurological disease. Acta Neuropathol. 1988;76:550-557. https://doi.org/10.1007/BF00689592 PMID: 2974227. Mehta V, Pei W, Yang G, Li S, Swamy E, Boster A, Schmalbrock P, Pitt D. Iron is a sensitive biomarker for inflammation in multiple sclerosis lesions. PLoS One. 2013;8:e57573. https://doi.org/10.1371/journal.pone.0057573 Epub 2013 Mar 14. PMID: 23516409; PMCID: PMC3597727. Michailidou I, Naessens DM, Hametner S, Guldenaar W, Kooi EJ, Geurts JJ, Baas F, Lassmann H, Ramaglia V. Complement C3 on microglial clusters in multiple sclerosis occur in chronic but not acute disease: Implication for disease pathogenesis. Glia. 2017;65:264-277. https://doi.org/10.1002/glia.23090 Epub 2016 Oct 25. PMID: 27778395; PMCID: PMC5215693. Nalugo M, Schulte LJ, Masood MF, Zayed MA. Microvascular angiopathic consequences of COVID-19. Front Cardiovasc Med. 2021;8:636843. https://doi.org/10.3389/fcvm.2021.636843 PMID: 33604359; PMCID: PMC7884319. Nicholas R, Magliozzi R, Campbell G, Mahad D, Reynolds R. Temporal lobe cortical pathology and inhibitory GABA interneuron cell loss are associated with seizures in multiple sclerosis. Mult Scler. 2016;22:25-35. https://doi.org/10.1177/1352458515579445 Epub 2015 Apr 28. PMID: 25921040; PMCID: PMC4702245. Orrego E, Castaneda CA, Castillo M, Bernabe LA, Casavilca S, Chakravarti A, Meng W, Garcia-Corrochano P, Villa-Robles MR, Zevallos R, Mejia O, Deza P, Belmar-Lopez C, Ojeda L. Distribution of tumor-infiltrating immune cells in glioblastoma. CNS Oncol. 2018;7:CNS21. https://doi.org/10.2217/cns-2017-0037 Epub 2018 Oct 9. PMID: 30299157; PMCID: PMC6331699. Pajo AT, Espiritu AI, Apor ADAO, Jamora RDG. Neuropathologic findings of patients with COVID-19: A systematic review. Neurol Sci. 2021;42:1255-1266. https://doi.org/10.1007/s10072-021-05068-7 Epub 2021 Jan 22. PMID: 33483885; PMCID: PMC7822400. Petrache AL, Rajulawalla A, Shi A, Wetzel A, Saito T, Saido TC, Harvey K, Ali AB. Aberrant excitatory-inhibitory synaptic mechanisms in entorhinal cortex microcircuits during the pathogenesis of Alzheimer's disease. Cereb Cortex. 2019;29:1834-1850. https://doi.org/10.1093/cercor/bhz016 PMID: 30766992; PMCID: PMC6418384. Potter LE, Paylor JW, Suh JS, Tenorio G, Caliaperumal J, Colbourne F, Baker G, Winship I, Kerr BJ. Altered excitatory-inhibitory balance within somatosensory cortex is associated with enhanced plasticity and pain sensitivity in a mouse model of multiple sclerosis. J Neuroinflammation. 2016;13:142. https://doi.org/10.1186/s12974-016-0609-4 PMID: 27282914; PMCID: PMC4901403. Povysheva N, Nigam A, Brisbin AK, Johnson JW, Barrionuevo G. Oxygen-glucose deprivation differentially affects neocortical pyramidal neurons and parvalbumin-positive interneurons. Neuroscience. 2019;412:72-82. https://doi.org/10.1016/j.neuroscience.2019.05.042 Epub 2019 May 30. PMID: 31152933; PMCID: PMC6818263. Ramaglia V, Dubey M, Malpede MA, Petersen N, de Vries SI, Ahmed SM, Lee DSW, Schenk GJ, Gold SM, Huitinga I, Gommerman JL, Geurts JJG, Kole MHP. Complement-associated loss of CA2 inhibitory synapses in the demyelinated hippocampus impairs memory. Acta Neuropathol. 2021;142:643-667. https://doi.org/10.1007/s00401-021-02338-8 Epub 2021 Jun 25. PMID: 34170374; PMCID: PMC8423657. Schartz ND, Tenner AJ. The good, the bad, and the opportunities of the complement system in neurodegenerative disease. J Neuroinflammation. 2020;17:354. https://doi.org/10.1186/s12974-020-02024-8 PMID: 33239010; PMCID: PMC7690210. Schirmer L, Velmeshev D, Holmqvist S, Kaufmann M, Werneburg S, Jung D, Vistnes S, Stockley JH, Young A, Steindel M, Tung B, Goyal N, Bhaduri A, Mayer S, Engler JB, Bayraktar OA, Franklin RJM, Haeussler M, Reynolds R, Schafer DP, Friese MA, Shiow LR, Kriegstein AR, Rowitch DH. Neuronal vulnerability and multilineage diversity in multiple sclerosis. Nature. 2019;573:75-82. https://doi.org/10.1038/s41586-019-1404-z Epub 2019 Jul 17. PMID: 31316211; PMCID: PMC6731122. Schwabenland M, Salié H, Tanevski J, Killmer S, Lago MS, Schlaak AE, Mayer L, Matschke J, Püschel K, Fitzek A, Ondruschka B, Mei HE, Boettler T, Neumann-Haefelin C, Hofmann M, Breithaupt A, Genc N, Stadelmann C, Saez-Rodriguez J, Bronsert P, Knobeloch KP, Blank T, Thimme R, Glatzel M, Prinz M, Bengsch B. Deep spatial profiling of human COVID-19 brains reveals neuroinflammation with distinct microanatomical microglia-T-cell interactions. Immunity. 2021;54:1594-1610.e11. https://doi.org/10.1016/j.immuni.2021.06.002 Epub 2021 Jun 9. PMID: 34174183; PMCID: PMC8188302. Sobue A, Komine O, Hara Y, Endo F, Mizoguchi H, Watanabe S, Murayama S, Saito T, Saido TC, Sahara N, Higuchi M, Ogi T, Yamanaka K. Microglial gene signature reveals loss of homeostatic microglia associated with neurodegeneration of Alzheimer's disease. Acta Neuropathol Commun. 2021;9:1. https://doi.org/10.1186/s40478-020-01099-x PMID: 33402227; PMCID: PMC7786928. Stolp HB, Fleiss B, Arai Y, Supramaniam V, Vontell R, Birtles S, Yates AG, Baburamani AA, Thornton C, Rutherford M, Edwards AD, Gressens P. Interneuron development is disrupted in preterm brains with diffuse white matter injury: Observations in mouse and human. Front Physiol. 2019;10:955. https://doi.org/10.3389/fphys.2019.00955 PMID: 31417418; PMCID: PMC6683859. Szulzewsky F, Pelz A, Feng X, Synowitz M, Markovic D, Langmann T, Holtman IR, Wang X, Eggen BJ, Boddeke HW, Hambardzumyan D, Wolf SA, Kettenmann H.. Glioma-associated microglia/macrophages display an expression profile different from M1 and M2 polarization and highly express Gpnmb and Spp1. PLoS One. 2015;10:e0116644. https://doi.org/10.1371/journal.pone.0116644 PMID: 25658639; PMCID: PMC4320099. Thakur KT, Miller EH, Glendinning MD, Al-Dalahmah O, Banu MA, Boehme AK, Boubour AL, Bruce SS, Chong AM, Claassen J, Faust PL, Hargus G, Hickman RA, Jambawalikar S, Khandji AG, Kim CY, Klein RS, Lignelli-Dipple A, Lin CC, Liu Y, Miller ML, Moonis G, Nordvig AS, Overdevest JB, Prust ML, Przedborski S, Roth WH, Soung A, Tanji K, Teich AF, Agalliu D, Uhlemann AC, Goldman JE, Canoll P. COVID-19 neuropathology at Columbia University Irving Medical Center/New York Presbyterian Hospital. Brain. 2021;144:2696-2708. https://doi.org/10.1093/brain/awab148 PMID: 33856027; PMCID: PMC8083258. Togo T, Akiyama H, Iseki E, Kondo H, Ikeda K, Kato M, Oda T, Tsuchiya K, Kosaka K. Occurrence of T cells in the brain of Alzheimer's disease and other neurological diseases. J Neuroimmunol. 2002;124:83-92. https://doi.org/10.1016/s0165-5728(01)00496-9 PMID: 11958825. Vaes JEG, Kosmeijer CM, Kaal M, van Vliet R, Brandt MJV, Benders MJNL, Nijboer CH. Regenerative therapies to restore interneuron disturbances in experimental models of encephalopathy of prematurity. Int J Mol Sci. 2020;22:211. https://doi.org/10.3390/ijms22010211 PMID: 33379239; PMCID: PMC7795049. van Duijn S, Bulk M, van Duinen SG, Nabuurs RJA, van Buchem MA, van der Weerd L, Natté R. Cortical iron reflects severity of Alzheimer’s disease. J Alzheimers Dis. 2017;60:1533–1545. https://doi.org/10.3233/JAD-161143 PMID: 29081415; PMCID: PMC5676973. Weber CE, Krämer J, Wittayer M, Gregori J, Randoll S, Weiler F, Heldmann S, Roβmanith C, Platten M, Gass A, Eisele P. Association of iron rim lesions with brain and cervical cord volume in relapsing multiple sclerosis. Eur Radiol. 2021 Sep 22. https://doi.org/10.1007/s00330-021-08233-w Epub ahead of print. PMID: 34549326. Weiner HL, da Cunha AP, Quintana F, Wu H. Oral tolerance. Immunol Rev. 2011;241:241-259. https://doi.org/10.1111/j.1600-065X.2011.01017.x PMID: 21488901; PMCID: PMC3296283. Wekerle H, Bradl M, Linington C, Kääb G, Kojima K. The shaping of the brain-specific T lymphocyte repertoire in the thymus. Immunol Rev. 1996;149:231-243. https://doi.org/10.1111/j.1600-065x.1996.tb00907.x PMID: 9005217. Williams GP, Schonhoff AM, Jurkuvenaite A, Gallups NJ, Standaert DG, Harms AS. CD4 T cells mediate brain inflammation and neurodegeneration in a mouse model of Parkinson's disease. Brain. 2021;144:2047-2059. https://doi.org/10.1093/brain/awab103 PMID: 33704423; PMCID: PMC8370411. Wimmer I, Zrzavy T, Lassmann H. Neuroinflammatory responses in experimental and human stroke lesions. J Neuroimmunol. 2018;323:10-18. https://doi.org/10.1016/j.jneuroim.2018.07.003 Epub 2018 Jul 6. PMID: 30196821. Yuan L, Wu J, Liu J, Li G, Liang D. Intermittent hypoxia-induced parvalbumin-immunoreactive interneurons loss and neurobehavioral impairment is mediated by NADPH-Oxidase-2. Neurochem Res. 2015;40:1232-1242. https://doi.org/10.1007/s11064-015-1586-1 Epub 2015 Apr 25. PMID: 25911467. Zhang B, Shen R, Cheng S, Feng L. Immune microenvironments differ in immune characteristics and outcome of glioblastoma multiforme. Cancer Med. 2019;8:2897–2907. https://doi.org/10.1002/cam4.2192 Epub 2019 Apr 30. PMID: 31038851; PMCID: PMC6558448. Zoupi L, Booker SA, Eigel D, Werner C, Kind PC, Spires-Jones TL, Newland B, Williams AC. Selective vulnerability of inhibitory networks in multiple sclerosis. Acta Neuropathol. 2021;141:415-429. https://doi.org/10.1007/s00401-020-02258-z Epub 2021 Jan 15. PMID: 33449171; PMCID: PMC7882577. Zrzavy T, Hametner S, Wimmer I, Butovsky O, Weiner HL, Lassmann H. Loss of 'homeostatic' microglia and patterns of their activation in active multiple sclerosis. Brain. 2017;140:1900-1913. https://doi.org/10.1093/brain/awx113 PMID: 28541408; PMCID: PMC6057548. Zrzavy T, Machado-Santos J, Christine S, Baumgartner C, Weiner HL, Butovsky O, Lassmann H. Dominant role of microglial and macrophage innate immune responses in human ischemic infarcts. Brain Pathol. 2018;28:791-805. https://doi.org/10.1111/bpa.12583 Epub 2017 Dec 28. PMID: 29222823; PMCID: PMC6334527.
Copyright: © 2022 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |