|
|
|
Free Neuropathology 2:28 (2021) |
|
Reflections |
|
50 years of surgical pathology / 36 years of neuropathology |
|
My way / A personal journey |
|
Sverre J. Mørk |
|
University of Bergen, Clinical Institute 1, Jonas Lies vei 91B, 5021 Bergen, Norway |
|
Corresponding author: |
|
Submitted: 13 October 2021 Accepted: 19 October 2021 Copyedited by: Henry Robbert Published: 08 November 2021 |
|
Keywords: Neuropathology, Reflections, Autobiography |
|
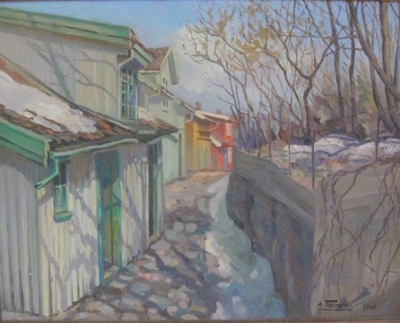
I: The start 1 Drøbak I was born in Drøbak (Norway) in 1942. Drøbak is a village-like small town at the eastern shoreline of the Oslofjord (the photo at the top, from the 1960s, shows our dark house dead centre). I grew up here, where everyone ‘knew’ each other. My neighbourhood is depicted in the oil painting from the spring of 1945 (the artist, Anton Thoresen, lived in the red house). In these safe surroundings, we played cowboys and Indians and hide and seek.
1 Drøbak I always wanted to be a physician. After 12 years of effortless schooling, my final grades lacked a few points for studying medicine in Oslo or Bergen, the only two medical faculties in Norway at that time. In the 1960s and 70s, 50% of Norwegian physicians studied medicine abroad. Germany, Austria, Switzerland, Great Britain, and Ireland were among the most popular countries. I applied to and was accepted by universities in Scotland, Austria, and Germany. I did not fancy studying in big cities like Berlin, Hamburg, Munich, or Vienna, with all their social diversions (or ‘opportunities’). So, among the actual medical faculties, I chose the one that looked ‘safest’ to me.
2 Giessen The Medical School of the Justus Liebig University in (Hessen, Deutschland) presented a bed-side-teaching concept where the 11 half-year semesters were organised in a school-like schedule (i.e., less freedom of choice for composing your curriculum). The fact that only a few students were accepted every year (‘…kleine Zahl seiner Medizinstudenten…’) was a perfect fit for me. Low numbers of consemesters and transparency (‘who is missing today? almost all on board!’) are two ways to harness young and drifting spirits. Steady surveillance by my peers turned out to be a helpful remedy. So, on October 30th 1961, I listened to the first lecture in German. After 3 weeks, I lowered the language barrier enough to understand most of what I heard. Although generally restless, I stayed at the Justus Liebig University from October 1961 until August 1967.
I kept the same room (#19) in the new dormitory ‘Landgraf Ludwig Haus’ from autumn 1961 until I left for Norway in August 1967. The drawing (45x15cm) by my little brother Erling hung above my bed; it has been with me ever since. It depicts the cycle of life and I have been through six of the depicted stages. The right figure fits me best now.
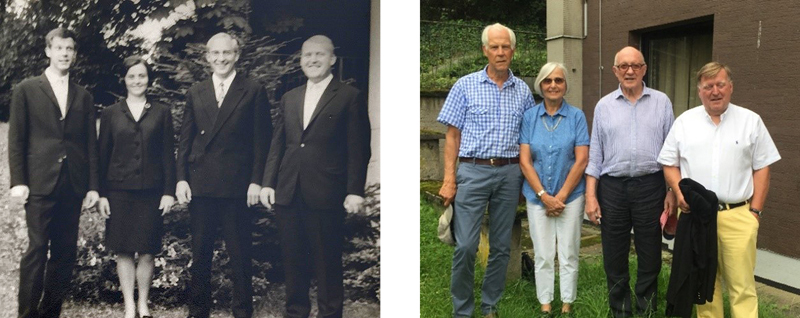
Sverre, Sabine, Hans, and Peter minutes after the last examination, 1967, and 50 years later (2017). The 12th semester was a tough stretch of examinations, all oral, 19 in all. We were examined in groups of four (the same four students during the whole ‘Staatsexamen’). We all did well. Here, in the summer of 1967, we were a relieved and happy quartet standing in front of my 11m2 studio after the very last examination.
3 Oslo Back in Oslo, half a year of additional studies (‘Tilleggskurs’) were required to pass the last hurdle to be an authorised physician. I was granted preliminary permission to practice medicine for the duration of this course. For the rest of 1967, I worked at the acute psychiatric ward for men of the Oslo City Hospital, which added to my mental health. I successfully completed ‘national examinations’ in Forensic Psychiatry, Forensic Medicine, Hygiene, Social Medicine, and Prescription Theory, and was awarded my diploma on December 12th 1967. It states that with my Staatsexamen from Giessen, with the Additional Course included, I was granted the Norsk Medisinsk Embedseksamen. No crystal ball could tell that four years later I would face many examinations every day executing diagnostic anatomical pathology (histopathology). I learned to see and register what the microscope shows you, internalizing what you see, processing these images into a conclusion, and revealing a correct and crisp diagnosis. 4 Kongsberg On January 1st 1968, I started 1.5 years of internship (six months of surgery, six months of internal medicine, lastly half a year of general practice). There was an official raffle for a number that would give you your place in the queue for choosing ‘your’ hospital as well as the country district where you’d spend the last stretch before being certified to practice medicine. I drew a low number, and decided to stay in the south of Norway, where I picked the community hospital in Kongsberg. There I met and worked together with another intern, Tore Böhmer Halvorsen, who three years later was to be decisive in My Way into pathology. I had family and friends in and around Drøbak on the east shore of the Oslofjord. Kongsberg was located inland on the west side of the fjord. During 1968, I’d travel those one-hundred-and-twenty kilometres countless times, through nights and early mornings, probably driving too fast. The interns and other young doctors lived in small townhouses close to the clinic. I had memorable times as a bachelor: socialising, playing bridge, driving on ice-covered lakes, skiing, dancing, sailing, and soccer. 5 Larsnes
The final six months of my internship took place within the boundaries of the district Sande, north of Stad, the roughest coastal stretch of Norway. My assignment was to assist the county doctor’s general practice. From Monday to Friday, the local bus unloaded patients at 8:30 in front of the district doctor’s office in Larsnes. At the very start most ‘customers’ wanted the attention of the ‘old’ doctor. With some luck in handling, I was quickly accepted by the inhabitants, giving the older doctor and me equal workload. In this large district with several islands and no bridges I had many demanding visits during the winter and spring, going out to islands in bad weather. But in June of 1969, military service in the Norwegian Airforce called.
6 Ørland Air Base Students of medicine, theology, and dentistry could absolve part of the 15 months of mandatory military service during their studies. I finished my recruit training (‘Boot Camp’) in between semesters. In the summer of 1969, I did a six-week Officers Course followed by one year as a flight surgeon in a care-of-the-flyer program at Ørland Air Base west of Trondheim. To fill this assignment, it was important to get an impression, a real feeling, of how it is to be a fighter pilot. Some of the enlisted doctors in the air force did get one single flight with a fighter jet. Airtime for the Northrop F-5 Freedom Fighter was precious. All non-fighter pilots within the air base would give ‘anything’ to be taking off in a fighter jet. I was lucky to be granted this experience five times for a total of 6 hours and 25 minutes. I flew tactical missions, night flight, interceptions, and granted control of the jet for some minutes, pretending that the top of the clouds was solid ground! Exciting and unforgettable! I met my wife Kari during this period and made many life-long friendships. 7 Meråker After I completed my obligatory military service, I had not yet decided what kind of a physician I wanted to be. A friend in the military persuaded me to spend the next year in rural Meråker (approx. 3,000 inhabitants). The single country doctor was leaving to specialise in psychiatry and had no successor. Following my friend’s call, I filled the vacancy for 12 months (1970-1971). It was quite a challenge for a green and inexperienced 28-year-old physician. I still remember my existential thoughts passing the local church that had a huge and grassy graveyard with only a few stones in a corner… Now (photo as of July 2021) the trees have multiplied and grown; still there is abundant free space.
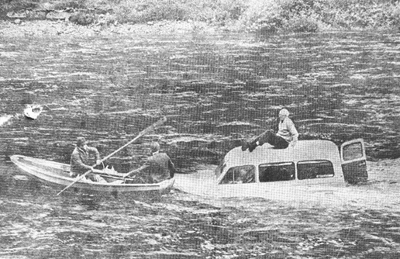
Decades ago, the people in rural areas of Norway were not accustomed to unnecessarily bothering the doctor. Calls during late evenings and nights occurred, on average, once a month. It was like a fairy-tale for rural doctors today. My medical practice went rather smoothly. When more complicated situations occurred (e.g., marriage counselling), I referred my patients to other competent persons or institutions. Generally, childbirths are among the most exciting things in life but I was terrified to being called to a difficult one. Thankfully, for me and the Meråker community, we were lucky enough to have a brilliant country nurse who acted as a midwife when necessary. Her soothing expertise was not called for during my tenure but nurse (söster) Inger’s familiarity with generations of inhabitants was indispensable for my practice of medicine there. One story has stayed with me to this day: An old man was found in a river on top of his Volvo van. He had fallen asleep on his way to his Swedish home, and then the local river flooded after heavy rainfall. The roaring river swept his van away and took it 100 meters downstream, where it snagged on large rocks. A farmer saw the incident and fetched me and other neighbours. We dropped a small boat in the river and secured it with an exceptionally long rope and then made our way to the driver. I was in the back of the boat to catch him. A journalist happened to pass by and shot the telling photo (from the newspaper Adresseavisen):
My colleague and friend Tore B. Halvorsen (from internship in Kongsberg) had started pathology training in Trondheim, the third largest Norwegian city. Trondheim was located 1.5 hours from Meråker. He tried to convince me to start working in the Pathology Department with him. We had many arguments back and forth, but he won the day he said, ‘The workforce is young, enthusiastic, and easy-going’. I realised that whatever I ended up doing, basic knowledge in general and special pathology would be a benefit. After one year of being the only MD for 3,500 persons, it was tempting to enter the safe harbour of a hospital. During my last months in Meråker, I had already sent two work applications to hospitals in Hamar (internal medicine) and Arendal (general surgery). These were specialties miles apart thematically and geographically. The idea was to have some time before choosing the eventual ‘right' specialty. None of my applications were even confirmed received. As the saying goes, ‘one bird in the hand is better than ten on the roof’. I accepted the ‘offer’ from the Pathology Department in Trondheim. Late letters of acceptance from both clinics arrived, but too late. I had already promised to join my friend in Trondheim. We (Kari, baby Pia and I) left Meråker without having contributed to an increase in the number of tombstones. Luckily. II: The start of my surgical pathology Trondheim 1971-1974
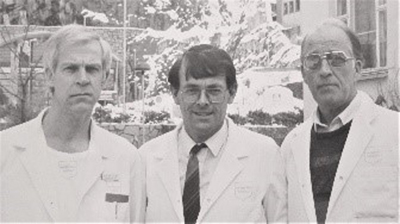
Sentralsykehuset i Sør-Trøndela My backbone in anatomical/surgical pathology was formed in the practice of a rather large community hospital. During the years in Trondheim, I was influenced by two colleagues, who had entered the pathology field some 8 to 12 months earlier than me. They were experienced fellows compared to the ‘rookie’. My colleagues (Tore B. Halvorsen and Arne Ødegaard) managed to keep me ‘downstairs’ doing autopsies for half-a-year. I was told that was the customary entrance to anatomical pathology. Starting out with post-mortem examinations should give you ample time (no hurry) to get a grip on the microscopy of tissues and changes therein.
Thus, my friends (Tore and Arne, see the next photo) had it easy, cuddled with biopsies, while I, lifting the burdens of autopsies off their shoulders, strived to ‘see’ and to ‘read’ what microscopy offered me. I longed for the real thing - to experience the task of being the doctor’s doctor in real time. That is what surgical pathology is about. In Goethe’s words: ‘Vor die Therapie haben die Götter die Diagnose gestellt’. But I was doing the essential work of diagnostic pathology: Establishing borders between normal appearances, physiological changes within the boundaries of normality, and initial changes signalling disease within tissues.
After only autopsies for month after month, I longed to address pathology in real time – biopsies. The Chief Physician of the pathology lab in Trondheim was painstakingly meticulous. His goal was not to miss anything in an autopsy or biopsy. He wanted minimal aberrations from the ‘normal’ to be written down on the final ‘List of Diagnosis’ on the front page of the autopsy report. I recall 20 or more items on the final list. We’d discuss the individual order of findings with minor, or even no clinical significance to give it its proper position on the list. I still use some of his elegant, descriptive phrases which characterise the microscopic picture in a few, well-chosen words. An awkward situation in the autopsy room: The ‘whole’ lung department came for a demonstration. We had interesting findings and good discussions. In the end, there was something in the air… They complained about the long time it took to get autopsy reports. I protested, knowing that we were pretty prompt. Later the same day, a doctor from the lung department informed me that one of the secretaries had a drawer where she puts reports related to ‘dead patients’ without telling anyone. My second ‘boss’ had been on a leave-of-absence as a surgical pathologist in Uganda. He was quick to recognise the important players in a tissue section and was effective in his diagnostic service. Nor did he dwell on details of no or minimal clinical significance. He was an efficient surgical pathologist. I learned from both, as I did from all the continued education courses in the following years. In 1973 I attended a tumour biology course in Uppsala, Sweden. The main lecturer was Professor Jan Pontén who headed the Institute of Pathology at Uppsala University. This course became a key experience for me. Pontén had a unique presence; he was part of what he presented - be it cells, tissues, neoplasia (‘tumours’, new growths, cancers). His research led to insights into growth capacities and proliferation dynamics in normal and neoplastic cells in cultures (in vitro) and in tissues (in vivo). The course involved exciting presentations on glioma tissue culture, multicellular spheroids, contact inhibition, growth capacity and proliferation dynamics. Bengt Westermark’s lectures also left a lasting impact. He presented many things that were new to me in my second year of diagnosing common surgical biopsies. For me, he added a third and a fourth dimension – he revealed the sheer complexity of the still-life lying in front of your eyes on the glass slide. You would have to imagine what is just a few microns below and above the actual tissue level. You have to think of the 4th dimension: The time aspect, how the present lesion could have evolved and what lies ahead (prognostication). The equation of ‘positive’ (proliferation/cell divisions/mitoses/mitotic figures) and ‘negative’ elements (cell death/apoptosis/apoptotic figures/necroses) defines the biological aggressiveness of a neoplastic tumour. Location and eventual spread add to the equation. The tumour biology course contributed to my interpretation ability but it also instilled in me the importance of trying to understand the biology and natural history of human cancers. Since there were no neurosurgeons north of Oslo, the ‘University Hospital’ Trondheim planned to start a neurosurgery unit at the hospital where I worked. The plan materialised in the mid-1970s with the appointment as Rolf Ringkjöb as the first neurosurgeon in Trondheim. To be prepared for the challenges this would bring, I applied for a junior position in the Neuropathology Section, Department of Pathology, Rikshospitalet (The National Hospital of Norway) in Oslo. The main task was to get accustomed to biopsy material from the peripheral, and central nervous system, the eye and orbit, as well as from skeletal muscle. The plan was to return to Trondheim to serve the Neurosurgery Department there.
III: The start of my neuropathology Rikshospitalet (The National Hospital of Norway) 1974-1976 Rikshospitalet (RH) was a hospital where special, rare, and difficult cases found their way. The Neurosurgical Department in Oslo served the whole country (about 3.500.000 individuals in the 1970s). The need for a set of criteria for histopathological diagnoses grew in the 1960s. We needed a necessary foundation for relevance of international cooperation in epidemiology and clinicopathological studies on cancer incidence and survival. The first ‘Blue Book’ was: Kreyberg L: Histological Typing of Lung Tumors. Geneva, World Health Organization, 1967. The Pathology Department at the National Hospital (RH) was influenced by the prominent pathologist Leiv Kreyberg (1896-1984). He headed the Institute of General and Experimental Pathology from 1938-1964. Professor Kreyberg’s scientific contributions were many. He left permanent footprints on carcinogenesis research, in typing and classification of lung cancer as well as diagnostic histopathology with emphasis on tumour biology. Olav Hilmar Iversen (1922-1997) headed the merged Pathology Department from 1964 to 1990. He recruited ‘aspiring scientists’ to focus on skin cancer (chalones), cell proliferation and growth control. One of them, Ole Didrik Laerum was to become a major influencer in my personal and scientific journey. My mentor to be, Ole Didrik Laerum, had done his PhD thesis on metabolic events related to cell population kinetics during early stages of mouse skin carcinogenesis. Laerum was inspired to follow a scientific career, and joined Manfred Rajewsky’s group at the Max Planck Institute of Virus Research in Tübingen, Germany, in 1971 as a postdoc. Around that time N-nitroso compounds were known to induce brain tumours in many different animal species. The rat turned out to be the animal of choice for experimental tumour production. Laerum and Rajewsky focused on the induction of brain tumours in the offspring of BDIX-rats after administration of ethyl-nitrosourea (ENU) at the 18th day of gestation, a standardised system developed by Ivancovic, Druckrey and others. Carcinogenesis was simultaneously followed in cell culture (in vitro) as well as in ENU-treated rats (in vivo).
Aagot Christie Löken (1911-2007), led the Neuropathology Section from 1952 until 1978. The official painting of her indicates the gentle intelligent person she was. To get into this new (for me) exciting field, works by Percival Bailey & Harvey Cushing, Hans Joachim Scherer, Klaus Joachim Zülch, Lucien J Rubinstein, for example, were mandatory reading. Not least, the works of the neuropathologist Scherer deserve a note. He published in German during the late 1930s and 1940s (also in English). Scherer performed enlightening histological studies on the development of malignant brain tumours in humans. He described how tumour cells invade the adjacent brain tissue by following existing anatomical structures and taking shape after them (secondary structures of Scherer). This was in distinction to the primary arrangement of the cells in the tumour itself. And this was just one of his many pioneering assessments. My neuro-oncological literature studies were educational and helpful, and I’ve returned to these books throughout my career. From the fall of 1974, the section of neuropathology was to be my workplace for the next two years. Here I was to meet the spectrum of primary brain tumours, the challenge of cell culture, and the excitement of experimental brain tumour research.
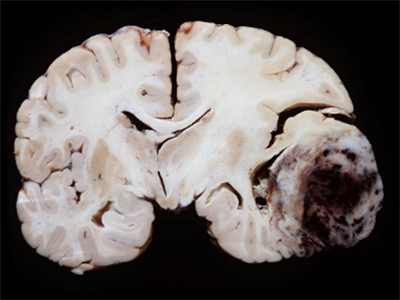
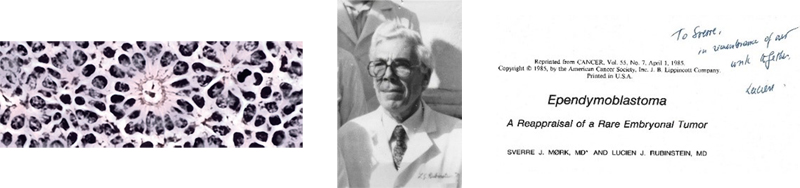
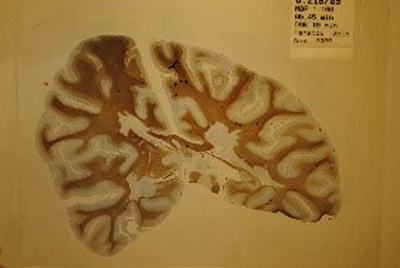
This photo of a brain section with grey and white matter and a brain tumour with a bleed (hemorrhage) was taken by Norbert Wey from a case I examined with a young colleague, Jens Pahnke, in 2002. (Department of Pathology, University Hospital Zurich, Switzerland) Early on, Dr. Löken asked me if I would be interested in working up some special brain tumour cases for eventual publication. Of course, I said ‘yes’. She suggested to focus on a group of neoplastic brain lesions with a varied connective tissue-like arrangement mixed with a common primary pattern of a malignant brain tumour. This new growth (tumour) is called gliosarcoma, a tumour pattern that needed clarification. As a newcomer to this intricate field (neuropathology/neuro-oncology), the first thing I had to do was to find out what kind of pattern warranted the use of this wording/diagnosis. Microscopically, I saw biphasic growth with one clear cut, intrinsic, malignant brain tumour, and another component with aggressive mesenchymal features. Evidently, this last tissue component could present in many forms. Long story short, my brain and I needed to start out with a tumour that had a more delineated histology. New to brain tumours, ependymoma seemed to be a relatively clearer defined entity. Therefore, I proposed to go through the National Hospital’s files to collect all tumours with this diagnosis. It turned out to be 148 cases of ependymomas of the brain and spinal cord in the archives from 1953 to 1974.This number reflects occurrence in the whole population of Norway during that period. After revisions and exclusion of plexus papillomas and subependymomas, we started a follow-up study of 101 cases. More on this project later (vide infra, part 2). The MDs of the Pathology Department met every morning at 8:00. I was early for my first morning meeting. I placed myself at the long table. Rather quickly I realised that my table position was wrong and unwanted. I repositioned, back to the wall (‘junge Burschen, zweite Reihe’) and fell in line. Time and again visiting pathologists and scientists ‘misplaced’ themselves, finding a professor standing tall alongside his/her assigned chair. Writing this, I recall another feeling: The anxiety fuming around the more scientifically oriented leading pathologists when, on rare occasions, a frozen section from a tumour-suspect breast lesion arrived under the microscope. My backbone (I felt like having one at the time!) in anatomical/surgical pathology was formed in the practice of a rather large community hospital. Thus, I felt confident evaluating the more common surgical biopsies. My self-centered ‘expertise’ was not often called for. Our section was run by two technicians and two MDs. I was in the starting block and enjoyed the challenges. We had a small frozen section area in front of the operating theatre on the 7th floor of the old block. When we were called upon, we had to leave our new high-rise and go into the main building which had a pater noster (see illustration) for staff only. A fun ride, especially when daring to go over the top.
Photo credit: L. Weber, 2014 My first frozen section: I have a habit of examining the slide before reading clinical info. I thought (and still think) that swiftness is a way of signalling proficiency. I quickly gave my interpretation over the intercom: ‘Meningioma’. My name said nothing to the neurosurgeon, nor did my diagnosis impress the operator, who called out that he was in the middle of the pituitary gland. He said that there was no way the lesion was a meningioma. Probably followed by a few more words not fit to print. The next few days, I checked through all files and found close to ten cases where ‘meningioma’ was called on frozen and changed to adenoma after viewing the permanent sections. A comfort of sorts. The work with the special brain tumour, ependymoma, stayed with me for a couple of years. At that time, the Norwegian population was ethnically consistent. We had one of the oldest cancer registers in the world, Kreftregisteret (est. 1951), with complete, mandatory reports of cancer cases from all pathology departments in Norway. This registry could be linked up to the mortality register of the ‘Statistics Norway’ (Statistisk Sentralbyrå, est. 1876). Thus, we could obtain a follow-up rate of 100%. Having such a setting, we wanted to establish the frequency of ependymomas in a well-defined, homogeneous population, and determine survival times after brain surgery. The final stages of the manuscript had a special and fortunate course. Karin (Blikstad) Miller, a colleague of mine, knew that I worked on a brain tumour project, and also that I had little experience in such an undertaking. She ‘offered me’ her husband saying that he loved to help aspiring authors with all sides of a manuscript. After retirement in 1968, Ashton Miller (1908-1992) moved to Oslo with his wife, Karin. He had been President of the Section of Urology of the Royal Society of Medicine in England. The result of his help with language, disposition, and corrections led to our shot at a high-ranking journal for eventual publication. I chose Cancer, a top cancer journal (of the American Cancer Society) at that time. Miller’s ingenious help with corrections and suggestions proved invaluable. It turned out to be a bull’s-eye (see below). Juan Rosai asked for and got permission to use one figure (a Kaplan-Meyer plot showing survival related to location of the tumour) in Ackerman’s Surgical Pathology (Juan Rosai / Sixth Edition, 1981). Six years later Lucien J Rubinstein ‘confessed’ to me that he was one of the reviewers. He had advised the editor to ‘accept it as is’.
Ependymoma paper: Ole Didrik Laerum returned to Oslo in 1972, where he continued in vitro and in vitro research on human and experimental brain tumours. He had brought with him a breeding pair of BDIX-rats, a gift from Druckrey personally. In the summer of 1973, he got a call for an academic position at the Gade Institute, Haukeland University Hospital, in Bergen. The call was furnished with means to continue and expand his research facilities. He accepted the call and moved to Bergen with his family and a pair of rats! From the summer of 1974, he embarked on a unique academic and scientific career in Bergen. In 1976, a flow cytometer (an advanced cell sorter based on Laser measurements) enforced the research landscape at Gade’s. He successfully guided 44 candidates to PhDs since then. In addition, Laerum served as rector of the University of Bergen, 1990-1995. I took over parts of Laerum’s cell culture duties in Oslo. From 1975 on, I was repeatedly asked to join Laerum in Bergen. Going there would probably secure an academic career for me. So… IV: The Gade Institute, Department of Pathology, Haukeland University Hospital, Bergen, Norway Gade’s institute was originally named ‘Dr. med. F.G. Gades pathological anatomical laboratory’. Fredrik Georg Gade (1855-1933) was the son of a wealthy merchant in Bergen. He was a pathologist who defended his thesis ‘About pathological anatomical changes in the tissues of neurotrophic origin’ in 1900. Gade donated NOK 150.000 (inherited from his father) to build a house exclusively for pathology (which included bacteriology at that time). The Gade Institute was inaugurated on March 15th 1912. On Friday October 1st 1976, I started on another stretch of My Way as a Consultant in Surgical Pathology and Neuropathology at the Gade Institute in Bergen. That same autumn, I was board certified in the specialty of pathology. Going to Bergen, I brought three years of anatomical/surgical pathology with two years of neuropathology, added as a subspecialty to complete the five- year minimum of specialty training for being a certified pathologist in Norway. This duality, surgical and neuropathology, stayed with me from then on. The beginning was demanding, with lots to learn, in many ways and in many fields. Ernest Glück was the oldest and the most experienced surgical pathologist in Bergen at that time. He took me under his wing and enabled me to become a doctor’s doctor at the Haukeland University Hospital. He had an open door, always willing to help when I felt insecure diagnostically. On a double-headed microscope with him, my suggestions were corrected or affirmed. It took almost half a year before I was joined by my family, and we could start settling in. However, in my scientific life, I settled in immediately with the group Laerum had started to build at the Gade Institute. The long presence of the Hanseatic League merchants in the city of Bergen (1350-1750) has contributed to the unique Bergen dialect. Bergeners have a saying: ‘I’m not from Norway, I’m from Bergen’. The wet climate is another well-known fact. Many jokes about the climate in Bergen are ‘floating’ around - you probably have heard at least one? Neurosurgeons, neurologists, ophthalmologists, and ear-nose-throat doctors in Bergen were pleased to have a ‘fresh neuropathologist’ aboard. Recent biopsies and brain autopsies were presented in the presence of neuroradiologists, neurologists, neurosurgeons, and others, with interest in the actual case. My colleagues interacted for the best of the person in focus (also called patient). In other words, these were clinicopathological conferences in the same form as at the RH in Oslo (all over, for that matter). Except that I always used gloves. I recall that Dr. Löken sometimes demonstrated bare-handed. A young and enthusiastic neurologist, Harald Nyland, contacted me early on. He tried to persuade me to take specimens from fresh autopsy brains. ☹ That was against my neuropathological workbook. To find and eventually confirm a suspected pathology in the central nervous system, you should first secure the brain, eventually with the spinal cord, trough fixation in 10% formalin (4% formaldehyde solution) for at least 2 weeks. Harald insisted upon the necessity of using unfixed brain tissue in the search for immune-active cells in the plaques, typically seen by the naked eye (grossly/macroscopically) in this brain disorder. This research resulted in significant findings (to be presented further down the road). However, since immunohistochemistry emerged to be effective on formalin-fixed tissue, the standard fixation method was used on most post-mortem brain examinations. A thorough study of post-mortem brains is still fundamental to understand neurological diseases.
Gade’s Staff around 1980, ‘none mentioned, none forgotten’. Exception: Professor emeritus Erik Waaler, in front, who discovered the Rheumatoid Factor in 1939. He went to Bergen and opened the Medical Faculty here in 1947. An open mind A touch of subjectivity is inherent in histopathological diagnoses. A reality is evidenced through inter-observer as well as intra-observer variance in histopathological assessments. Since I am easily influenced, I long ago settled into a routine of ignoring the specimen’s clinical, anamnestic data. My policy is to grab the object glass, glance at the slide on its way to the position between light source and objectives. To look through the microscope before reading at the clinical data (age, gender, actual problem et cetera) is My Way to lower bias in reading the histology. That is, before I acknowledge the clinical problem, and the eventually suggested, tentative diagnosis (TX). Starting every biopsy assessment with an open mind, trying to decide the source of the material (organ?), then a quick glance for changes, has worked well for me. It is not a time-consuming ordeal, one second, sometimes a few, does it. The trick is to convert the evaluation (reading) of every biopsy specimen into an internal competition. This habit makes the daily workload fascinating to handle. I’ve not had a single day of boredom in the company of my microscope and a carefully produced tissue section. I’d say that this habit (modus operandi) has fed alertness and positivity. In my office I had two computer screens in front of me. One hooked up to the Pathology Department and the other connected to the servers of the University for surfing the web to keep updated. In this way I could confer with the newest data without having to shut down the one with sensitive patient information. As mentioned before, the BDIX rat was an asset that Laerum used to the fullest extent for the years to come. The breeding of the BDIX rats was in the hand of animal technician Tore-Jacob Raa. He kept breeding 35 generations! The +40-year-old photo shows us injecting tumour cells intraperitoneally:
During the 1970s, Marc Mareel and Leo de Ridder at the University of Ghent, Belgium, developed organotypic methods for the study of invasiveness by malignant tumour cells in vitro. Chick heart tissue was found to be well suited for invasion studies. In Bergen, Laerum cooperated with the group in Ghent, and I was naturally involved in these activities. This cooperation led to my thesis: ‘Characterization of premalignant and malignant cells from the nervous system’, which I defended publicly at the University in Bergen, May 1983.
V: International activities The idea to start a society of neuropathology in the Nordic countries originated chiefly from Erna Christensen and Edith Reske-Nielsen in Denmark, Aagot Christie Löken in Norway, and Patrick Sourander in Sweden. Ansgar Torvik, Oslo and Yngve Olsson, Uppsala were involved as well. The Scandinavian Society of Neuropathology was to be a forum for persons interested in clinical and experimental neuropathology. The founding meeting was held at Rigshospitalet, Copenhagen, Denmark on January 23rd 1965. Erna Christensen and Patrick Sourander were among those few who re-formed the International Committee of Neuropathology into The International Society of Neuropathology in Copenhagen in 1967. Sourander was the grandfather of modern neuropathology in Scandinavia. The Scandinavian Society had joint meetings with British, German, Italian and other nation’s neuropathological societies. These were friendly and inspiring conferences with social events. Several Nordic neuropathologists were members of other nations’ neuropathological societies. The winter and summer meetings of the British Neuropathological Society (BNS) were especially popular among Scandinavians, I would say. In the BNS Summer Meeting 1979 in Oxford I presented ‘Ploidy of human intracranial neoplasms studied by flow cytometry’. I did not follow up ploidy and brain tumours, since I did not feel that this would have an impact on prognostication of an individual person’s brain tumour. (Two Roads) The first large and overwhelmingly impressive meeting on My Way was that of The VIIITH INTERNATIONAL CONGRESS OF NEUROPATHOLOGY, Washington, D.C., USA, September 24-29th 1978. I still have the program and the list of participants, as well as the abstracts of that meeting. This event was special for Americans too, since it represented the first International Congress of Neuropathology to be held in the United States. The earlier Congresses are listed here:
I 1952 Rome Kenneth M Earle was the President and Henry de Forest Webster the Secretary General of that congress. I have good memories of both these gentlemen. The same applies to Officers of the AANP from that meeting: Asao Hirano, John J Kepes, Richard L Davies, and Michael N Hart. From the congress, one memorable recollection: a big audience in a dark, huge room with a large picture projected onto the wall. There was a tiny, fuzzy structure barely visible, in the middle. This was Stanley Prusiner’s first image of a scrapie associated particle. If body language and unclear murmurs were any indication, the audience was not convinced that there was a specific structure to be seen in the image. In the program leaflet, I ticked off a platform presentation: ‘GFA AND INTERMEDIATE FILAMENT PROTEIN IN GLIOMA CELLS’, given by Anders Paetau of Helsinki University, Helsinki, Finland. It must have been my first acquaintance with this household molecule to be. The 1980s In 1980, I returned to Washington, D.C., to spend three weeks at the Armed Forces Institute of Pathology (AFIP) in Bethesda, Maryland, just outside the city limits. The AFIP had made life easier for the world’s surgical pathologist through their soft-covered fascicles (‘a set of books being published in instalments as separate pamphlets’), which presented the tissue patterns of tumours. These inexpensive Atlases of Tumor Pathology standardised nomenclature, classification, and diagnostic, histological criteria of human tumours of all primary sites.
I got permission to visit the Departments of Neuropathology and Ophthalmic pathology. After a quick photo session I had an ID card, and then the huge concrete building (‘atom bomb secure’, they said) was free to me. My plan for the first week was to see as much eye tumours as possible in the unit of ophthalmic pathology, headed by Lorenz E Zimmerman. On Monday morning, ‘Second in Command’, Ramon L Font welcomed us (around 10 US and international eye aficionados) with actual, current cases of diseases of the eye and orbit. He really grilled us for diagnostic suggestions. Originally from Cuba, he spoke with an accent. I recall him correcting the eye doctor (from Mexico) in front of me, who had answered ‘leukeMIA’; Ramon Font with a prompt correction: ‘leuKEmia, leuKEmia’. The doctor in front of me uttered in his cupped hand, ‘At least I speak two languages’. Zimmerman had finished editing the Blue Book on Eye and Orbital Tumors. The manuscript was being printed. He was so kind to give me access to the background material, most importantly, a box with glass slides. The content was identical to the material sent to leading ophthalmic pathologists worldwide. The rest of the week I was completely occupied by ‘reading’ the different lesions through the microscope. With the box came the diagnoses offered by every one of the cooperating international ophthalmic pathologists (more than 10 of them). I kept my eyes (see ‘An open mind’ above) away from the judgment of the international expertise. I worked the microscope in a relaxed mood (‘no rush’) and wrote down my assessment of every case. Only then would I check the diagnoses of the specialists from the international editorial board. The head of Department of Ophthalmology in Bergen, Professor Torstein Berthelsen (1923-2008) did contribute financially to my study tour to the AFIP. The week ended with a feeling of having the stamina to adequately serve the eye doctors of Western Norway. The last two weeks of My Way of the AFIP experience turned out to be great as well. I was the only ‘free player’ there. I was fortunate to have the personal attention of the neuropathology staff, especially Gary Clark and James Henry, who helped in picking interesting cases to study during my stay. Vernon Armbrustmacher supplied me with muscle biopsies. I recall memorable lunches with Kenneth Earle (Chief of Neuropathology) and Leslie H Sobin (editor of innumerable books on histological classification of tumours, and poetry (see example in box)).
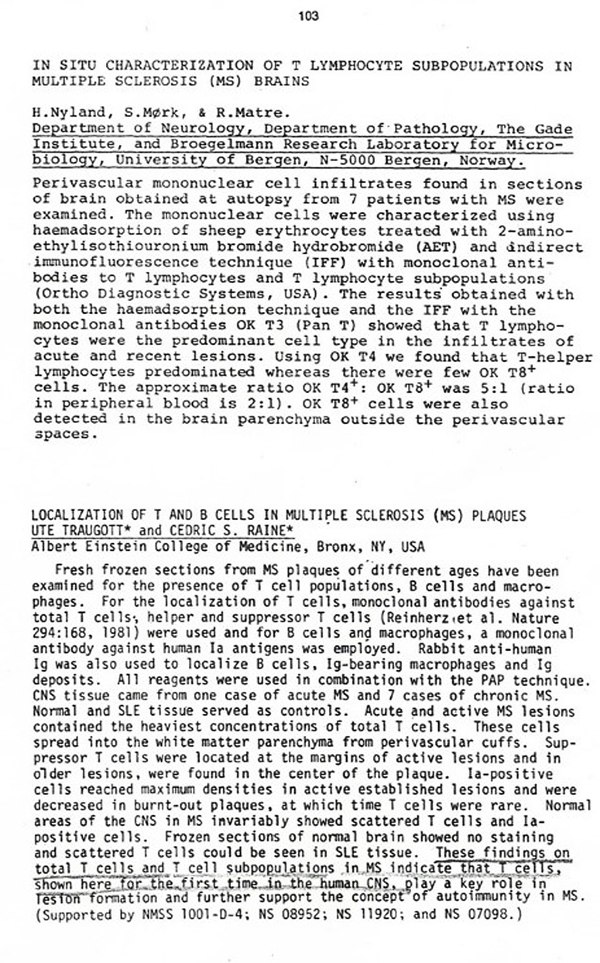
Despite all the studies we try L H Sobin I made life-long friends at the AFIP. The AFIP experience added substantially to my brain’s library of diseases. AFIP is history now. Wikipedia: In a blow to the US’s pathology community, the Armed Forces Institute of Pathology will close its doors Sept. 15 (2011), the victim of government cost-cutting initiatives. The Washington, D.C.-based facility, which holds around 95 million tissue samples in its repository and employs platoons of ‘renowned scientific consultants’, has been a ‘global resource for disease diagnosis and analysis’ for nearly 150 years. Returning to Scandinavia in 1980 On the flight back to Scandinavia, I was seated next to a young Japanese who told me of his years in Palo Alto at Stanford University which was the highlight of his time in the US. His positive tale about Palo Alto/Stanford planted a seed in me. Wasn’t the eminent diagnostician and renowned author of the brain tumour ‘bible’ situated in Stanford? He was. The unrivalled textbook on brain tumour pathology used since the 1960s was Pathology of Tumours of the Nervous System (published by Edward Arnold). This book was co-authored by Dorothy S Russel and Lucien J Rubinstein. It was first published in 1959. In total, five editions of this critically acclaimed, highly appraised book have been published. After defending my thesis in May 1983 I felt ready for a change. I planned to join Lucien J Rubinstein for a one-year sabbatical. I wrote a letter (September 20th 1980) introducing myself, asking for a possible stay under his guidance. Professor Rubinstein’s response came some weeks thereafter. He was pleased with my ‘interest in coming to work with us’ and he detailed interesting projects they were pursuing. He asked for three letters of reference, ‘possibly one from Dr. Löken, whom I know of course quite well’. The letter also stated: ‘we are planning to move our neuropathological operation from Stanford University to the University of Virginia in Charlottesville’. This was a surprising statement; I had planned for both: Stanford and Rubinstein. The latter had to be the preference, of course. So, instead of sunny California, Virginia would be my state of residence, if I got the opportunity to team up with LJR. Opportunity knocked, and a few years later, I went through the door. (See VIII) IX International Congress of Neuropathology, Vienna, Austria September 5-10th 1982 Wednesday, September 8th: At 16:30 I presented ‘IN SITU CHARACTERIZATION OF T LYMPHOCYTE SUBPOPULATIONS IN MULTIPLE SCLEROSIS (MS) BRAINS’. At 16:45 Ute Traugott presented ‘LOCALIZATION OF T AND B CELLS IN MULTIPLE SCLEROSIS (MS) PLAQUES’. These presentations were awaited with interest, not least due to the take-home message of Traugott and Raine’s abstract: ‘shown here for the first time in the human brain’. The Chairpersons (Ingrid Allen and Ellsworth C Alvord) decided that the two last oral presentations of the afternoon were to be discussed together at the end. The discussion I was nervous and cannot recollect much about the discussion. I recall that the meeting room was half dark, with thick curtains hiding the sun outside. One person stood up, asking me if I ‘believed’ those cells I presented really were lymphocytes. I ended up saying, in the affirmative, that ‘I believe they are’. Then he pointed at me, looked around in the audience and called out (screamed, in my ears/brain): ‘He’s a believer…, he’s a believer!’. This aggressive comment hit me in the chest, like a heart attack.
After the session closed, I was told that this person was known to act rudely/impolitely in discussions. He, a virologist, from the US West Coast, was Mikkel Gammelsten (name changed to Old Norse by me). I still remember the few neuropathologists who patted my back afterwards. But this unpleasant occurrence is still with me. To cure ‘it’, I reset my focus to the message we presented in 1982. The Cedric Raine group penned it for us: ‘T cells, shown here for the first time in the human CNS’. We could not have written it better ourselves.
Now it pleases me to look back on that afternoon session in Vienna 40 years ago and re-establish the fact that our group from Haukeland University Hospital (Harald Nyland, Department of Neurology), Roald Matre (Immunologist, Broegelmann Research Laboratory, and I) were the ‘first’ to show evidence that T-cells were at the site of MS lesions. We even gave an estimate of the ratio (5:1) between helper and suppressor lymphocytes, as well as presenting CD8 positive cytotoxic T-cells in the parenchyma. Our findings were published in a letter to the editor under the heading ‘T lymphocyte subpopulations in multiple sclerosis lesions’ in December 1982 (New England Journal of Medicine 307:1643-1644, 1982) and those of Traugott and Raine in January 1983. This fact seems forgotten in most references to this topic. The results presented in Vienna 1982 have been repeatedly confirmed during later years. In 1986 the Scandinavian Neuropathological Society hosted the Xth International Congress of Neuropathology. This meeting took place in Stockholm, Sweden with Patrick Sourander as President of the congress. It was a huge success, scientifically as well as financially, not least through the economic efficacy of Yngve Olsson. To my knowledge, the number of participants (1,300) have never been surpassed by later International and European Neuropathology congresses. In 2002 our Society hosted the Euro-CNS meeting in Helsinki, Finland, with Matti Haltia and Hannu Kalimo as chief organisers. The 12th European Congress of Neuropathology was organised by Bjarne Winther Kristensen, Denmark from May 31st – June 3rd 2021. Our Society also organises the Northern Lights Neuroscience Symposia. VI: Northern Lights Neuroscience Symposia During the preparation for the 1986 event in Stockholm, the idea came up to start a high-quality series of Neuroscience Symposia. I took the challenge of organizing the first such meeting. My cooperation with neurologist Harald Nyland had focused on Multiple Sclerosis for some years, and it was convenient to select themes related to this disease. The leader Gerd Hagen of the Norwegian MS Society provided financial support so we could invite active researchers from any country to give the newest research in their field of expertise. All the 17 internationally acknowledged scientists complied with our invitation to contribute to the First Northern Lights Neuroscience Symposium. The scientific focus was ‘Myelin and Demyelination’. One of the invited, Bruce D Trapp, would turn out to be a valuable research partner for the next 30 years!
Bergen is the hometown of the composer Edvard Grieg. No rain and extraordinary nice weather, cloudless blue skies, and up to 25oC daily for the meeting (May 20-23rd 1987), which coincided with the opening of the Bergen International Music Festival. This is a yearly main Norwegian cultural event existing since 1953. A fine combination of science and culture.
Kuo-Chun Ma (Shanghai) with Yngve Olsson (Uppsala). Most participants came from Europe, many from North America and a few from Asia and Africa. Some of us still remember Dr. Kuo-Chun Ma from Shanghai. He had been taken from the dinner table and imprisoned for eight years by the Gang of Four. He had learned English well enough that he could serve as an interpreter. That was reason enough for imprisonment. He was one of the first MDs allowed to travel out of China. Kari Skullerud and Yngve Olsson could tell you more about the astonishing Dr. Ma, a highly intelligent and flexible personality. Probably they will do so here in Free Neuropathology.
Sam Ludwin (Kingston) and Hans Lassmann (Vienna) enjoy luncheon at Hotel Norge, Bergen (First NLNS, May 1987). There have been numerous NLNS since then. To mention a few: The one in 1995 (the VIth NLNS on Inflammatory Muscle Disorders) was an adventurous and highly praised event. The location was Svalbard/Spitsbergen and Kari Skullerud (neuropathologist, Oslo) had the idea and organised the symposium.
Ellsworth C ‘Buster’ Alvord (1923-2010) and wife Nancy (left) took part in our first NLNS. He was an outstanding neuropathologist and scientist from Seattle (University of Washington).
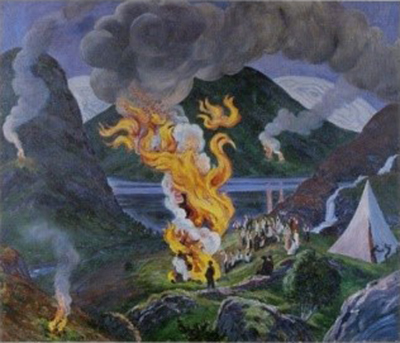
Numerous attendants attested to the quality of all aspects of this very first NLNS gathering with a focus on Myelin and Demyelination. See reactions tagged for the facsimile. Harald Nyland and I organised another symposium on Multiple Sclerosis in 1996. We used a painting by the artist Nicolai Astrup (1880-1928) as an eye catcher. In English the title of the oil painting is ‘Midsummer Eve Bonfire’. For us it symbolises the various aspects of demyelinating lesions. Multifocal fires of different age and intensity, some burned out, others with flames high! By the way, Nicolai Astrup was introduced for the first time in the USA just this August 2021. The venue: The Clark Art Institute, Williamstown, MA. The Boston Globe writes: ‘the best artist you’ve never heard of’ and adds: ‘The Wall Street Journal and the New Yorker, no less, are cheerleaders’.
VII: International activities continue
The IXth NLNS in Reykjavik, 1998, was organised by my good friend Gudmundur Georgsson. He is standing on the left. In front Peter Stubbe-Teglbjerg (Aalborg) with wife, center Mara Popovic (Ljubljana) and Marie Bojsen-Möller (Aarhus), then Henning Laursen (Copenhagen), Inger Mazanti (Southampton), and Henrik Schröder (Odense). American Association of Neuropathologists Inc. and other activities I have attended many annual meetings of this society, and met so many people who left an impression on me. The list of all those whom I feel a special bond with would be too long. But I must mention here two persons: one a neuropathologist and the second the spouse of a neuropathologist. I met Bernd Walter Scheithauer in June 1984 at my first annual meeting of the American Association of Neuropathologists. During a lunchbreak I saw him having a beer at the pool bar in the Holiday Inn at the Embarcadero, San Diego, CA. When I think of him, I recall a quote from the TV show Mad Men: ‘When a man goes into a room, he brings his whole life with him’. I joined him and swapped stories interchanged with information about our similar ‘upbringing’ in Europe. In later meetings, I noticed that Bernd was augmenting newcomers, disregarded their origin. He trained in the Department of Pathology at Stanford University School of Medicine during the last half of the 1970s. There he was influenced by Rubinstein who was the Director of Neuropathology at Stanford at that time. From 1979 Bernd worked in the Department of Laboratory Medicine and Pathology at the Mayo Clinic in Rochester, Minnesota. His neuro-oncological expertise was undisputed, and he enjoyed displaying it.
He welcomed many Norwegian pathologists to stay with him at the Mayo Clinic in Rochester, Minnesota. We met many times on both sides of the Atlantic, presenting cases at workshops etc. in Prague, Toronto, Zurich, and at other venues. Both of us, among others, were searching for histological features that could predict survival of persons with oligodendrogliomas. At the 1984 meeting I presented preliminary data on oligodendroglioma. The full work ‘Oligodendroglioma. Histologic Evaluation and Prognosis’ was published in 1986. In a review titled ‘Oligodendroglioma: Diagnosis and Prognosis’ (Seminars in Diagnostic Pathology 4:352-261, 1987) Janet M Bruner (Chief Neuropathologist, M. D. Anderson Hospital and Tumor Institute, Houston, Texas) notes: ‘Detailed clinical analysis in two large series of cases,2,3 with similar attention to the relation of prognosis and histologic features in two companion studies4,5 have provided concrete and apparently valid criteria for grading’.
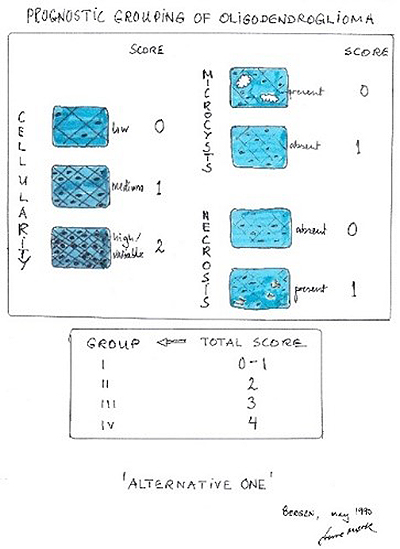
Grading of oligodendrogliomas was an issue of interest not only for neuropathologists. Bernd was used to the so-called St. Anne-Mayo grading system, which was primarily for astrocytomas. Nuclear atypia, mitosis, endothelial proliferation, and necrosis as the morphologic criteria to assign a grade, 1-4, according to presence of cero to all four criteria. The Norwegian experience was that microcystic change, necrosis, and cell density were the only histologic features of prognostic significance. It was surprising that nuclear atypia, mitosis, and endothelial proliferation did not display effect on survival. It was a fertile soil for discussions and further studies (more on this topic under ‘1990’ later). He opened his home to me, and I am happy to say that he also stayed in our home in Norway a couple of times. Bernd died in 2011. He is very much missed. Since San Diego (1984), I have visited Arlington, Atlanta, Boston, Cleveland, Denver, Minneapolis, New Orleans, Orlando, Pittsburgh, Portland, St. Louis, Salt Lake City, San Francisco, Seattle, and Washington, D.C., but have not done much tourism, unfortunately. Usually, it is airport - hotel - airport - like for most readers of Free Neuropathology, I’m sure. Annual meetings usually occurred in the first half of June, starting on Thursday, and ending early afternoon on Saturday. When your home base reimburses attendance fees, with paid leave of absence included, you are reluctant to leave a meeting. But I could get in some exploring by having a stayover to Sunday (ostensibly to save on airfare). I will never forget one such Sunday: June 11th 2000, in Atlanta. It was the Day of Pentecost. I went for a walk around noon. A woman in a glorious white dress, came towards me down the sidewalk. To my surprise, I recognised a lady I had met once or twice in Charlottesville 12 years before. She beamed, telling me about her experience in an Episcopal Church just minutes ago. After entering the packed church, she stood out. She was called by the chaplain to present herself, and then experienced open arms. She ended up singing and swaying with the whole vibrant parish. She had planned this months ago when she realised that the meeting her husband was going to also coincided with the celebration of Pentecost in the Deep South. Later we got acquainted with each other well. Working in Zurich, I spent many a weekend enjoying the hospitality of Elisabeth and Elias Perentes who both worked at Novartis in Basel and lived just over the border to France. In 2003, a lorry ran a red traffic light, crashed into two cars, and killed both drivers, one of whom was Elisabeth driving home after work. I will never forget the flamboyant Elisabeth Perentes on that hot Sunday in Atlanta. VIII: Lucien Julien Rubinstein, UVA, Charlottesville
University of Virginia, Charlottesville After defending my thesis in May 1983, I was ready to join Lucien J Rubinstein for a one-year sabbatical leave of absence from Haukeland University Hospital in Bergen. Late June 1983 Lucien met me at the little Charlottesville-Albemarle Airport outside of Charlottesville, Virginia. Leaving the airplane, I was struck by the burning sun and the warm, moist air (40oC). In other words, my first experience with steaming hot Virginian weather. The air was ‘dead’, not even a little breeze gave relief. After a few welcoming words, he told me that when you live in America, the first thing you should do is to buy a car. Mobility is a must here, he stressed. In the parking lot, Lucien’s open Mustang was a pleasant surprise. I recall his gray hair in the wind speeding down Route 29 South to the small town (approx. 25,000 inhabitants). He took me to my temporary quarters. I was to live in a huge white barn, from another century with barren rooms, high ceilings and worn-out furniture. In most rooms, there were slowly rotating ceiling fans. I did not notice any students. It was hotter inside than out, and ‘summer empty’. As we looked around, I think my facial expression and body movements signalled reluctance to be ‘dumped’ there. After some minutes of silent disbelief, it must have dawned upon Lucien that this residence was not appropriate for a 41-year-old cold-blooded Norwegian Visiting Associate Professor of the honourable UVA. From Norway, I had tried to find a flat or townhouse in Charlottesville or outskirts (Albemarle County) without success. It would be easier when being there in person, I thought. It took some weeks before I found a fitting place for my family (wife Kari and our children, Pia, 12, Ine, 11, and Erik, 2 years). In the intervening time, I was offered lodging in LJR’s home, a one-stock redbrick house on the hillside close to the famous resort Boar’s Head Inn. The adjacent, even posher, Farmington Country Club had been their first choice, but LJR’s application for membership was declined for unknown reasons. The interior of Lucien’s and wife Mary M Herman’s home was elegant and even cosy. I was offered a nice bedroom with a queen-size bed, soft and comfortable. The room had a feminine flavour. It took a while before I realised that I occupied Mary’s bedroom… I felt welcome and even comfortable in Mary and Lucien’s house the two weeks of my stay in Ednam Drive. Mostly I was offered a quick breakfast with Lucien. He worked on a new edition of Pathology of the Nervous System, usually from early morning, not seldom in his morning-robe. Therefore, he often came in late. Taking Lucien’s advice, I took my first test drive, which proved to be an unpleasant encounter. Raised on cars with manual gearshift, my initial attempt to shift led to an immediate clash with the windshield. Without prolonging my essay, I will skip all the details about problems with old and big American cars, only to say that I needed assistance to find where to fill the gas tank.
One of my first days in Charlottesville, I was introduced to Lennart Heimer, a neuroanatomist/physiologist, originally from Gothenburg. UVA was evidently proud to have him in their midst. Heimer spoke English with a heavy Swedish accent, which didn’t seem to hurt him in academia. I felt relieved to continue with my own Scandinavian drawl.
Neuropathology had offices, labs and special rooms for cell/tissue culture, electron microscopy (ultrastructure), and biochemistry as a special section of the Department of Pathology. It was situated within the old colonial redbrick building with ‘MEDICAL SCHOOL’ above the entrance. An antique, thin, squeaky, and almost worn-out door can be seen above. Exiting it, you entered a small lawn close to a cosy, little street, called an avenue (University Avenue). Although not broad, wide, or lined by trees, ‘avenue’ makes sense (avenir – access to) since it leads to the original UVA campus. University Avenue had some nice small restaurants, coffee shops, fast-food spots, and bookstores. I remembered the site of the very first lunch break Lucien invited me to. This picture, taken through the front screen of my rental car, shows the red front of the smallest joint in the avenue. We had sloppy joes (without the bun).
My assigned office space was shared with two neuropathology fellows, Estelle T May and José M Bonnin. We had weekly lab meetings, were we talked projects, progress, assigned workplaces and equipment. My first lab meeting was rather special. A disagreement about glass pipettes used by Sozos was awkward to listen to. They were taken from Mary’s side of the lab bench! I uttered something about spoiling time in discussing pettiness. My voicing did not fall in good soil, as the saying goes in Norwegian. I was registered as a difficult new boy on the block, a notion further enabled a few weeks later.
The summer of 1983 was very warm with record highs. On my lunch break each day, it was a shock to leave the cool air-conditioned interior entering a sauna with clothes on (never did that, by the way). Now and then we (Estelle, José and I) had our Burger King Whopper on the grass close to the serpentine wall surrounding the original Thomas Jefferson’s UVA.
Our office door had a little window, on the inside of which I put a little black and white version of Edvard Munch’s ‘The Scream’. It was facing the hallway and hung there long enough to annoy passers-by. Someone tacked up a message telling me to remove the image. It was an intuitive or subconscious cry from me that I see clearly now. Amazing grace comes to my mind: ‘was blind, but now I see’. I recently wondered if my fellow Fellows felt the same unease at the time. They most probably did.
As the time went by, I felt more relaxed, especially during the weekends. This ‘saturday in the office’ posture was more casual than necessary. Note the small microscope compared to the ‘monsters’ of today. Family life in Charlottesville expanded just a few days after Kari, Pia, Ine and Erik’s arrival in the US on August 11th 1983. We rented a townhouse in ‘Four Seasons’ just outside the Charlottesville city limits. After a few days, we found out about a lake not too far away. At Chris Green Lake we enjoyed cooling off in the hot and humid August with swimming and making ‘bombs’ (pictured here). On the first day in the water, a passing young swimmer asked our girls if they were from Norway. Her mother was. The young girl came up to us on the beach with the telephone number to her home. One phone call and we quickly got anchored to people that we still have as friends, close to 40 years later.
Other social activities: the head of Neurological Surgery (John A Jane) was exceptionally gracious. I was able to attend two of his garden parties. ‘Christmas in June’ was a yearly event hosted by ‘DR. AND MRS. JOHN A. JANE’. It was a fantastic party, which people looked forward to for weeks. In a corner of their huge lawn, a Dixieland Band entertained with feel-good vibrations. There was plenty of food and beverages. Some persons even followed the suggested theme of the party for ‘OPTIONAL MASQUERADE AND/OR MASKS.’ The Christmas Party in June was an extraordinary successful socialising event. I was introduced to many interesting people. I recall: ‘You have to meet Lennart Heimer, he is from Sweden, and has recently published a Neuroanatomy textbook.’ I had not heard Heimer’s name before. His ‘The Human Brain and Spinal Cord: Functional Neuroanatomy and Dissection Guide’ had just been published in 1983. The reviews were excellent and so was the book, which I promptly acquired. Lennart’s wife was Norwegian, and there were further Scandinavian ladies married to American scientist and businessmen. They met once a month, and Kari was wholeheartedly taken in. In our Four Seasons neighbourhood we connected to neighbours with children from abroad, like Peru, Israel, Finland, and Canada. After a harsh start, our two girls thrived in the public Jack Jouett Middle School. They were considered just very shy Americans. After those first awkward weeks, things turned around. Neuropathology continued Lucien’s office was relatively modest in size, soft-coloured interior, decorated in beige and brown. A two-headed microscope was the first thing you saw when entering this sacred place. You did not want rush in there. I felt tension in the air from the start. (Was it only me?) However, I found the weekly review of the recently arrived consultation cases (‘CCs’) most educational. Brain tumour cases came from all over the world. The fellows and I were assigned cases for presentation at the review meeting, and I greatly valued the scholarly discussions related to these rare and mostly difficult cases. The significance of patterns and elements of the microscopic changes were deliberated in extenso. Back at our desks, we dictated microscopic descriptions and diagnoses. The front page, for the ease of the submitter to see, gave a clear conclusion/diagnosis. This was followed by a very wordy description to ensure that every possibility was taken into consideration. Rubinstein’s wordings in letters to editors (and others) were polite, starting and ending with ‘Thank you for’ with interspersed ‘...would you be so kind as to…’, and ‘…please find...’, a custom I have adopted which has suited me well. Another matter was his quest for excellence in microphotography with many retakes and increases of magnification (‘go to a higher mag!’). He typically stressed the fact that you are writing for educated and interested readers, so you do not have to explain everything. Trust that your audience is ‘level’. I recall a special incidence: At the double microscope, he rubbed his face and moaned over the quality of the tissue section we were looking at. A long silence, and then ‘Who ordered the lab to do this (immunostaining, my comment) GFAP?’ I did. More moaning, then: ‘Technicians must respect the persons who give them orders’, meaning that he himself had to order immunohistochemistry if he wanted the result to be ‘perfect’. In other words, I was not respected. A deep sadness hit me, I felt both bad and sad. ‘They’re like animals’ he said. I thought I didn’t hear right! Lucien was unique in his position as a world authority on brain tumours with a more than complex personality, not without ‘musicality’ and a sort of sweetness and vulnerability. In January of 1990, Lucien J Rubinstein died at 65. The eulogy, written by Scott R Vandenberg, Bernd W Scheithauer, and Darrell D Bigner, has a passage that I would like to share with you. ‘Lucien Rubinstein had a remarkable dramatic presence. Not many people could fail to remember the first encounter with him. All were affected by his charming manner, subtle and, at times mischievous wit, or lancinating wrath’. My wife would easily have stayed in Charlottesville for another year or two. I, however, longed for doing neuropathology and diagnostic surgical pathology back home. (Two Roads) Lucien had a special liking for embryonal tumours, so I’ll close the UVA experience with three images.
IX: The 1980s continued During the year as a Visiting Associate Professor at UVA, I continued work on my oligodendroglioma project, which I had started years earlier. Through recommendation by Kari Skullerud (neuropathologist, The National Hospital of Norway, Oslo), we (The Norwegian Cancer Society) hired a young, inexperienced person, Arnhild Tollefsrud. Her intelligent suggestions and hard work included correct registration of hundreds of data points from 208 persons with a oligodendroglioma diagnosis. Her insightful work provided sound foundation for three manuscripts. The first, ‘Oligodendroglioma. Histologic Evaluation and Prognosis’, was sent to the Journal of Neuropathology and Experimental Neurology (JNEN). It turned out to be quite an ordeal to get through the review process of the JNEN, with many back-and-forth letters between me and the powerful Editor-in-Chief, John Mossy. Some sentences from our correspondence might be of interest. I wrote: ‘Our contribution is one for (and by) neuropathologists and surgical pathologists, and not for experimental neurologists. We feel that our manuscript reveals the materials, methods, and results in a way that compares favourably with other contributions in this field. We therefore hope you will accept it in its present form. For example, to give a more ‘precise definition’ of oligodendroglioma than used in authoritative textbooks and in the WHO Classification seems beyond our competence and scope’. I asked Mossy to return the manuscript to us, and politely added: ‘I do not regret sending it to you, as your comments and criticism have improved the article’. But then it was accepted for publication. Janet M Bruner (Houston) found an error in Figure 7 of our JNEN oligo-article. We were impressed by her ingenuity and gave a reply in a letter to the editor (Journal of Neuropathology and Experimental Neurology 45, 1986). Ellsworth C Alvord suggested further avenues of studying histological correlation of oligodendroglioma with prediction of survival. (Two Roads) The two other ‘oligo-manuscripts’ were accepted and published by the Journal of Neurosurgery after a thorough review. High on life, after getting an extremely nice comment from the Editor-in-Chief, William F Collins, I sent in a suggestion for the cover page of the issue in which our article would appear. I got no feedback. Oh well…
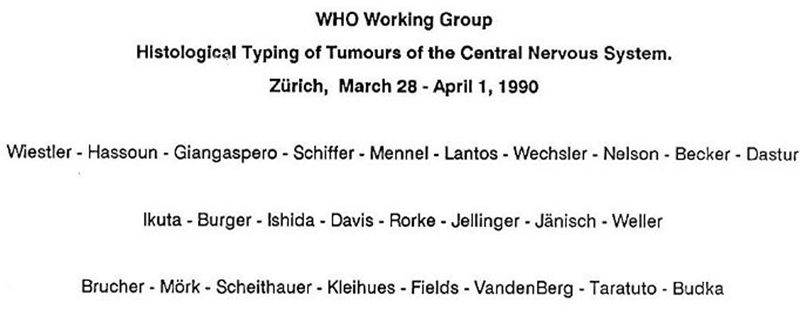
After publication of the oligodendroglioma papers in JN and JNEN, many neuropathologists and neurosurgeons reacted in a positive manner. I gave ‘oligo-talks’ in Europe and in the States. Following one in in Memphis, Tennessee, the neuropathologist, F Curtis Dohan Jr, wanted to discuss some interesting cases with me. Entering the microscopy room, I was met by a 12-headed microscope loaded with 10 residents. Ten (!)and all were residents of the largest neurosurgical department in the Southern US. The cases ‘Curt’ had sought out for discussion were certainly not straightforward. I remember that we had lengthy discussions before concluding. Thinking back, I must say that the quality of questions and comments from those mainly neurosurgical residents surpassed anything I had experienced before. The 1990s Two key events in My Way occurred in 1990. In January I received an invitation from Paul Kleihues (Zurich/Lyon) to participate in a brain tumour meeting in Zurich. The invitation had a questionnaire attached, where you answered, ‘by circling the answers which correspond best to your current opinion on classification and grading’. At the end of March 1990 Paul called together a WHO Working Group to discuss Histological Typing of Tumours of the Central Nervous System. The main purpose was to get consensus on the nomenclature to be used in the next version of the IACC brain tumour classification. Although the meeting took place more than 30 years ago, you can recognise the expertise of the participants by reading some of the last names in the official photo. Scott Vandenberg sat in for Lucien Rubinstein who died in January 1990. There were slide-viewing sessions, short presentations on specific problems followed by panel discussions, and occasional decisions by voting. For me, a highly educational and excellent experience.
One evening, Peter Burger, Bernd Scheithauer, Roy Weller and I discussed criteria for grading oligodendroglioma among other things. Bernd and I agreed to take this further. We wanted to do an ‘Oligo Study’ (Heading of a letter from Bernd to me, July 9th, 1990) comparing different grading systems. I had the impression that ‘my’ system would be part of the study, but something went wrong. I am not sure what it was. The study was now ‘Oligodendroglioma Grading Project’. In the summer of 1993 I had fulfilled my contribution to the somewhat changed study/project. Caterina Gianinni compiled the input from six neuropathologists and six surgical pathologists and was the first author of ‘Oligodendrogliomas: Reproducibility and Prognostic Value of Histologic Diagnosis and Grading’ (Journal of Neuropathology and Experimental Neurology 60(3):248-62, 2001).
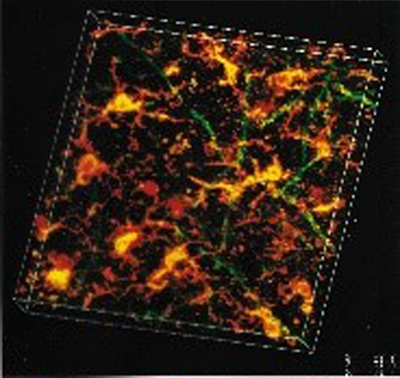
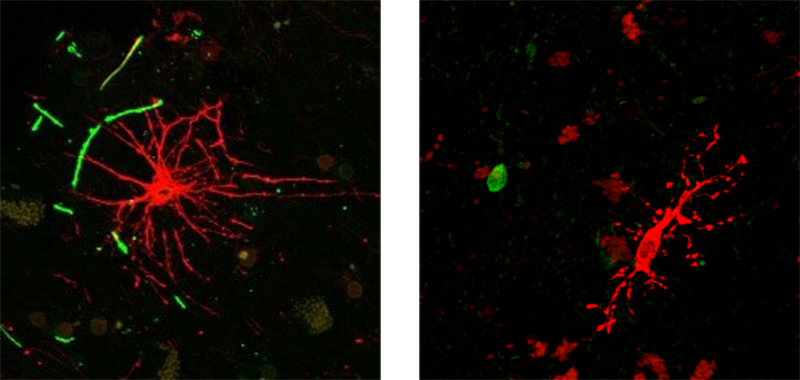
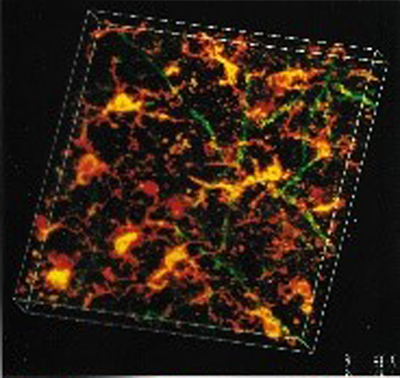
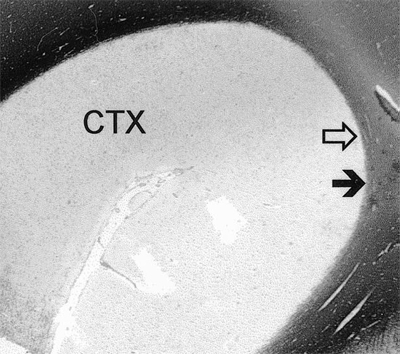
The second event came after the XIth International Congress of Neuropathology, Kyoto, Japan 1990, which was my first and only visit to Asia. I had a gap of two or three days between the end of the Congress and an MS meeting in the same city. I was completely on my own; no one understood what I said. I did not interact with anyone for days. At least it felt so. (Writing this, I reflect that feeling down and being depressed is not the same.) That aside, for the second time in life, I felt so down that I considered it depression. I avoided entering the balcony of my hotel room… On the way back home, I bought a CD at the airport in Singapore. It was the misspelling on the cover that hit me: Beethoven’s Third Symphony (‘Erotica’)! Back in Norway, Beethoven helped me over my down period/depression. From the first day, I played his ‘Eroica’ very loudly (very, very) driving to and from work. It helped very much. I did not miss a day’s work. The ‘Third’ is a dynamic source of mental energy. X: Department of Neurosciences, Lerner Research Institute, Cleveland Clinic, Cleveland, Ohio The first time I met Bruce Trapp was in Vienna, 1982. He was in company with my friend Henning Laursen (neuropathologist at Rigshospitalet, Copenhagen). They knew each other from the time they spent as postdocs at the National Institutes of Health, Bethesda, Maryland (Laboratory of Neuropathology and Neuroanatomical Sciences, National Institute of Neurological and Communicative Disorders and Stroke). After short introductory remarks, Henning suggested that we come together in a ‘Heuriger’ the same evening. ‘Heuriger’ is a word for Austrian wine taverns serving this year’s wine (heuer: this year) that they produce themselves. They serve their wines in gardens, and welcome everyone warmly; just what I needed following the infamous afternoon session. Outside on bleachers, a couple of Americans and Scandinavians had a jovial and laid-back time in a pleasant atmosphere. Since then, Bruce Trapp and My Way have crossed many times. In one AANP Annual Meeting, Bruce asked me if I knew any ‘bright Norwegians’ (!) who could be recruited to join him at the Department of Neurology, Johns Hopkins School of Medicine, Baltimore, Maryland. I said yes. Back in Bergen, a young MD, Lars Bö, took the challenge and met with Bruce Trapp and the Chairman of the Neurology Department, John ‘Jack’ Griffin, to check out the ‘premises’ in 1990. Lars and his wife, Elisabeth, went to Baltimore in 1991, supported by the Norwegian Research Council. He developed into an open-minded, innovative, and rational researcher. Bruce Trapp was, and still is, a well-known myelin researcher. His ultrastructural studies on myelin are of exceptional quality and won him the ‘Weil Award for Best Paper on Experimental Neuropathology’ presented at the AANP Annual Meeting 1986. So, when Harald Nyland and I prepared for a meeting on myelin and demyelination, Bruce Trapp was one of the 17 international experts we invited to Bergen. In the 1990s the Lerner Research Institute at the Cleveland Clinic Inc. (Cleveland, OH) wanted to add a Department of Neuroscience to its stock of nine research departments. Bruce Trapp applied and was offered the position of Director of the newly established unit. He started developing neuroscience at CCF in 1994, and Lars fit well into the structure that Bruce had in mind. We, wife Kari and son Erik (born 1980) moved to join the ‘Trapp Lab’ for a one-year-sabbatical in 1997/98. Meeting the Trapp family was an enjoyable event. After a short while we were treated and felt like family. Our families are closely connected still. I could write pages about Caring Carol, the twins Brian & Dan the Man, Sara, David, and Bruce. I hope it will be done by others. The collaboration of neuroscience in Cleveland and neuropathology in Bergen developed in a persistently friendly and inspiring atmosphere. I learned the basics of preparing and immunostaining free-floating 30μm thick sections for confocal microscopy by Ansi Chang. She was, and still is, an extremely skilled and intelligent person who I am glad I met and with whom I still keep in touch. She instructed me to be an approved user of the Leica Aristoplan laser scanning microscope. Through confocal microscopy and computer-based, three-dimensional reconstructions, we studied pathological changes in multiple sclerosis brains.
Many hours were spent on the confocal microscope looking for clues. The attraction of the ‘collapsed’ stacks of the laser-scanned immune-stained 30μm thick sections from the frozen specimen of brain tissue was evident in images. The image is stained for myelin and microglia. It was a good feeling to know that you had removed the CNS at post-mortem, fixated, selected areas to study, cut, and stored tissue wet or in paraffin blocks. I brought some of the tissue to the US in my hand luggage. The co-operation between Cleveland and Bergen resulted in many publications (the first results were published in 1994, and the last paper last year in 2020. One, in the New England Journal of Medicine had a special impact since our findings initiated an Editorial (‘Demyelinating Diseases ― New Pathological Insights, New Therapeutic Targets’) in the same journal. Our results were presented on national TV and, in February of 1998, reached the front page of the New York Times. In other words, the old knowledge that MS lesions affect grey matter of the brain as well as white matter came in ‘new wrappings’ and got some great attention. I had long since noticed that the characteristic lesions in MS brains did not spare the grey matter. So I got the idea to sample grey and white matter from preselected areas disregarding macroscopic changes/lesions. We wanted to see what the eyes did not see; therefore, we searched for a new way to examine MS brains. We did not sample macroscopic lesion. Rather we stuck to sampling brain material strictly from preselected areas. We weren’t looking for macroscopically evident MS lesion; instead, we took tissue probes from predetermined areas. (I was experienced in cutting formalin fixed brain in the frontal plane coronal sectioning). A section through the anterior commissure turned out to be a fine landmark for getting similar brain areas from different individuals with MS. From this section we sampled the superior temporal, the cingular gyrus, and parietal tissue. We revealed the extent and pattern of demyelination in the cerebral cortices and underlying white matter of 20 MS brains. Tissue from the same preselected brain areas from people without neurological disease served as controls. Our findings were published in the JNEN in 2003 and undermined the amount and importance of grey matter (cortical) changes in the brains of MS patients. Lars Bö defended his PhD dissertation ‘Multiple sclerosis: Immunopathological studies of inflammatory central nervous system demyelination’ at the University of Bergen, in 1998. The five peer-reviewed articles of his dissertation have, as of May 2021, been cited 5,639 times. Space was precious in the energetic and crowded neuroscience floor. So, when the newly ‘added’ neuropathologist/researcher Susan Staugaitis arrived in Cleveland, I had to ‘give up’ my office to her. She was split between diagnostic service for pathology and research in neuroscience. Susan was intelligent, sharp, and well informed. She was an outspoken and confident contributor in many AANP and other scientific meetings. We had lot of engaging discussions. Susan sadly had a glioblastoma diagnosed in 2014, a fact that she was extraordinarily open about. In 2017, I sent her a Christmas greeting with this photo from the library room.
Drs Susan Staugaitis (✝) and Ansi Chang were treasured colleagues of mine in the Trapp lab. Susan: ‘It goes without saying that I am still alive. I never believed I would be around this long. I am doing my best to stay as strong and safe as possible as I continue to live alone in my home. It helps when we can look at things from multiple perspectives and find the part of the glass that is half full’. She died in August 2018. XI: Other activities Medical University of Lübeck In the year 1360 the Hanseatic League (the German Guild of Merchants) created an overseas office in Bergen. For almost 400 years, they dominated commerce and social life here. Hanseatic influence is still very much evident in surnames, buildings, and the wharf (‘German wharf’ or ‘Tyskebryggen’, after WWII best just called ‘Bryggen’) in the centre part of the city. In the 1970s, a ‘Hansa-related’ idea was born at an international forensic science meeting where Professors Otto Pribilla from Lübeck and Johan Chr. Giertsen from Bergen happened to meet. They found it timely to try to establish an official contact between the two Hanseatic cities through their respective universities. A general agreement of cooperation was officially acknowledged by both parties in 1976. The aim was and is to foster better contact through student exchange, postgraduate education, and research within the fields of medicine and natural sciences. I had the honour of taking Giertsen’s place as coordinator of this cooperation from 1993 to 2011; most of the time together with the surgeon Professor Jan Fredrik Halvorsen. We enjoyed interactions with many team players in Lübeck. Manfred Oehmichen, Eberhard Schwinger, and Michael Seyfahrt were among the proactive professors, to name a few. The main burden of this successful treaty was carried by the administrators Peter Mühlhausen (Oberamtsrat) in Lübeck and Johannes (Johs) Teigland (Faculty Director), as well as Torill Knag in Bergen. In 1995 the General Agreement of Cooperation between the Universities was extended without limitation. Universitäts Spital Zürich 2002 In 2002, I spent an interesting year at the Universitäts Spital Zürich. I was asked to take care of the diagnostic neuropathology for a year or so. Phillip U Heitz was the director of The Institute of Pathology and Molecular Pathology, with its highly qualified medical and technical staff. I especially remember the productive, pleasant, and friendly atmosphere within the department. Social skills were ‘comme il faut’, highlighted by free ski weekends in Davos. Lifts, lodging, and food were paid for by the department! The Institute of Neuropathology was completely focused on prion research, enigmatically led by Adriano Aguzzi. This meant they were continually searching for a clinically oriented neuropathologist to take care of the diagnostic routine for a longer or shorter period. I went for one year (December 2001- March 2003). I intended to combine diagnostic ‘neurosurgical’ work with microglia research but that did not materialise. I did, however, learn a lot about prions and psychology, and witnessed the immense effort of postdocs to satisfy their manager during the weekly progress report (and in-between). I connected with many of the optimistic, eager, dedicated, young scientist during my period there. 12 years later, one of them, Jens Pahnke, became professor of neuropathology at the Oslo University Hospital. His track record has been and is superb. I appreciated working with the fine technical staff of the Institute of Neuropathology.
This photo shows that we had a good time in between skiing, needless to mention afterwards! Miscellaneous Major changes have increased the effectivity of doing diagnostic pathology and research over the years. I’ll just mention a few elements that made My Way easier. One general problem that gummed up the works all over was the backlog created by secretaries typewriting manuscripts. If you had a few minor changes, pages or the whole report had to be typed anew. From 1973 the IBM ‘golf ball’ typewriter with an internal correction feature reduced the backlog for typing and retyping manuscripts. Another problem was that all manuscripts had to be submitted with original photos to be accepted for review. There were strict instructions for authors, especially regarding illustrations, and you had to pay for coloured illustrations. It seemed that every journal had different rules. The invention of the Letraset’s dry rub-down instant lettering made it easier to put arrows on figures. They were large, half transparent sheets with letters, stars, arrows and more. Letraset was ‘expensive’ and popular; you had to ask around to find the right sheet. It was not uncommon to find the tokens you needed for your illustration ‘scratched out’. It took time to order new sheets. Letraset was very popular for years before desktop publishing took over. To find and check out correct references, libraries had meter after meter with Index Medicus occupying their shelfs. They received new, heavy books annually. You had to carry one to your desk, turn the pages, carry it back to the shelf, get the next one, and so on. During the 1990s, the introduction of the internet and world-wide-web (www) accelerated the shift from printed to online information, especially with the start of PubMed. Also in the 1990s, PowerPoint transformed the process of preparing and giving presentations. The development of immunohistochemistry (IHC) opened possibilities in characterizing tissue, cells, and cell products. At first, you were lucky if you knew someone who had produced an antibody and was willing to share it. Now the production of antibodies is a huge industry providing opportunities for research and industrial applications. (Order online and receive your antibody in a couple of weeks!) For me, it was great experience to effectively pinpoint the inborn superintendent of the microenvironment of the normal brain, the microglia (MG)! They are almost invisible in conventional staining (HE). The importance of MGs cannot be overrated. They are everywhere in the CNS, acting as sensors (housekeepers) of the local milieu. They are constantly working, switching between quiet monitoring physiologic activity and active efforts to keep changes from doing harm. Tissue Micro Arrays (TMAs) became popular in the 2000s. Small cores of tissue (for example tumour material) could be cut from a ‘donor’ paraffin block and, one by one, placed in an ordered way in columns and rows to the recipient block. As large number of samples could be examined in a single cut from one recipient paraffin block, thus creating an exceptionally cost-effective and timesaving research tool. The digitizing of specimen slides with computer-assisted technology has led to Digital Pathology as a powerful and expanding line of work for easing many aspects of diagnostic pathology. Special scanning machines convert the tissue specimen on the glass slides to a seamless image on your computer screen. This allows for a wealth of possibilities related to histological assessment (diagnosis), research and teaching. I have worked as a Digital Pathologist for many years now. My first experience was in Costa del Sol (Spain) in 2015. There I performed microscopic evaluation and diagnoses on surgical biopsies in between rounds of golf and trips to the beach. Digital Pathology allows for quicker measurements, easier comparisons, straightforward sharing of information, and effortless transfer of digitised images for consultation and second opinions. This home-office type of diagnostic, digital pathology is perfect in this SARS-CoV-2/COVID-19 pandemic. Polymerase chain reaction (PCR) needs no introduction, but I will tell the following historical anecdote: As a postdoc at the Institute for Enzyme Research, University of Wisconsin 1968-1970, the Norwegian Kjell Kleppe (Bergen based) found ways to copy larger amounts of DNA from a limited quantity (Studies on polynucleotides. XCVI. Repair replications of short synthetic DNA’s as catalyzed by DNA polymerases. Journal of Molecular Biology 56(2):341-361, 1971). Kary B. Mullis used more heat resistant enzymes in the reactions and was given the Nobel Prize in Chemistry for 1993 ‘for his invention of the polymerase chain reaction’. Neither the Nobel Committee nor the Laureate mentioned the pioneering work of Kjell Kleppe. The importance of Kleppe’s work has been emphasised recently (see Jonathan D Kaunitz in Digestive Diseases and Sciences 60(8):2230-2231, 2015; https://en.wikipedia.org/wiki/PCR). Haukeland University Hospital, Bergen, Norway The Norwegian Cancer Registry contains complete, mandatory reports of all cancer cases in the country. Since the registry can be linked to the Mortality Register of ‘Statistics Norway’, a follow-up rate of 100% is obtainable. In cooperation with Fröydis Langmark (Director of the Norwegian Cancer registry) and Arild Helseth, we performed population-based epidemiological studies on intracranial gliomas, primary intraspinal neoplasms, and meningioma. We also analysed the occurrence of multiple primary neoplasms in people with meningioma. Results were published in 1988 and 1989. In 1989, Are Helseth defended his thesis ‘A Population-Based Survey of Neoplasms of the Central Nervous System in Norway’ in Bergen, for the PhD degree. Another fruitful collaboration was that with Christos D Katsetos, the neuropathologist of the Departments of Pathology and Laboratory Medicine at Hahneman University and St. Christopher’s Hospital for Children Hospital, Philadelphia. We knew each other from mutual UVA experience (both, at different times, disciples of Lucien J Rubinstein). This cooperation led to his successful public defence of ‘Neurobiology of Class IIIb-Tubulin Isotype: Differential Cellular Expression in Human Development and Neoplasia’ for the PhD degree at the University of Bergen in 2002. Paul Kleihues (Zurich/Lyon/Zurich) and Roy Weller (Southampton) were the evaluators of and opponents in the public discussion of the dissertation at the Haukeland University Hospital, Bergen. (Sadly, Christos passed away in 2017.) In the central block of Haukeland University Hospital, forensic pathology is located next to labs and offices of neuropathology. We have had much to do with each other. Years of oil-related professional diving in the North Sea has claimed many lives. Likewise, amateur diving is another diving activity that sometimes can be fatal. Forensic post-mortem examinations of such cases always gave rise to examinations of brains and often the spinal cord too. Surprisingly, there is very little damage to be found even in long-time professional saturation divers. One should think that the pressure and the stress of such activity takes its toll. We were surprised, after examining 8 to 64 (!) tissue blocks from the spinal cord of twenty divers with immunohistochemistry, to conclude that the cords did not reveal tissue changes. While I am happy that the study was published in the journal Undersea & Hyperbaric Medicine, I now think that I perhaps should have published this thorough report somewhere else with wider reach. Norwegian MS Registry & Biobank
Research related to brain tumours, and MS have been closest to my heart. In cooperation between the Norwegian Multiple Sclerosis Competence Centre and the Norwegian MS Registry & Biobank, we have organised CNS material for research purposes. We have stored clinical data, paraffin blocks, stained, and unstained slides from more than 40 persons with MS. In many cases bioengineers Brynhild Haugen and Laila Vårdal embedded whole coronal sections from MS brains into paraffin. They are cut by a large sliding microtome (not many of them around) into 20μ sections, mounted on glass slides in glycerol, and cover slipped for microscopic analysis. The manoeuvring via water bath to glass is technically challenging, as is the staining process. The images (above and below) show how it can be done!
Regarding MS, there is so much to wonder about. Looking through the microscope on IHC stained lesions, I still haven’t been able to grasp who or what is the wrongdoer? Angiocentricity of lesions is for me not a general feature. Staring at different highlighted antigens from the same lesion gives me an uneasy feeling that the key is there, you just cannot add up the clues to unlock the enigma. I think of the philosopher Henri Bergson: ‘The eyes only see what the mind is prepared to comprehend’.
Above, a thin (20μ) coronal brain sections immunostained for myelin (dark brown). It shows bilaterally irregular, and sharply bordered, large, demyelinated areas adjacent to lateral ventricles. Look closely and you will notice the amount and variation of the widespread myelin deficits in the cortex.
To me it looks as if the players in demyelinated foci have their own agenda! To the left, a single reactive astrocyte dominates the field with scattered myelin rests. (Two intact internodes?). To the right you see a tiny myelin debris in a cortical (autofluorescence) field with total loss of myelin and a solitary microglia cell (watch dog) with multiple tiny cell processes, which do not signal activation. What happened to the myelin? One can wonder… then I consider: what about the bioactive substances that are present in the same spot, untagged?
This slightly tilted 3D presentation shows a very active cortical MS lesion; the most active picture I have seen. Microglia is in red, and myelin is in green. The yellow colour signals co-localisation. The morphology is clearly that of acutely activated microglia engulfing myelin. Think about this image as a point in time in a video, with a dynamic remodelling of the cytoplasm, with extensions and retractions in an undulating mode. It goes from slim microglia via this morphology to full-blown macrophages. Hopefully methods of the future will start to bring us nearer to the ultimate goal: To unravel the mystery of Multiple Sclerosis.
Above a conventionally cut section where demyelination (black=myelin in subcortical white matter) affects the full thickness of the cortex can be seen. The extremely sharp border between affected and normal brain should say something about how the wrongdoer moves in the microenvironment. It is a well-known fact that the movement of cerebrospinal fluid (CSF, oedema) differs greatly within the CNS. The restriction of fluid movement is much higher in grey matter than in white matter. The complexities of the multi-layered and compact grey matter lead to slower drive of substances here. Our (Bö et al.) findings presented in JNEN in 2003, showed purely cortical subpial demyelination in an extent not demonstrated earlier. This indicates that the CSF transports myelin-harming substances which lead to demise of myelin in MS. (Fluid transport through the ependyma of the ventricular walls is unrestricted; this being so, white matter oedema drains directly into the CSF.) I have a gut feeling considering initial events in MS. Recent studies have revealed prominent clonal expansion of CD8 positive T-cells within the CNS during MS (Journal of Immunology 206(1), 2021). This is just one example that has confirmed our findings, first reported in Vienna in 1982.
The photograph shows my closest co-workers and friends from before 2000 to 2012 and beyond: the bioengineers Edith Fick, Laila Vårdal, and Brynhild Haugen. Many are those who have helped me along My Way. In Bergen, I have had expert assistance on different occasions by Anne Marie Austerheim, Karin Eliassen, Gerd Lillian Halseth, Nina Holmelid, Randi Lavik, Karen Böhm Nilssen, Bendik Nordanger, Tore-Jacob Raa, Laila Vårdal, and Grethe Waaler. I left diagnostic neuropathology after turning 70 in 2012. I felt like I was one of the last surviving members of the HE only (+ some IHCs) era of neuropathologists - squeezing the most out of basic, classic, cost-efficient, affordable, and fast histopathology. After April 2012, I continued as a consultant in general surgical pathology (at 30% of full time) through 2019. That was the end of my affiliation to the Haukeland University Hospital. However, I am still engaged in digital diagnostics. I have spent my pathology career believing in short, relevant descriptions, quick responses, and up-to-date diagnoses. I am content as an emeritus professor sharing a 15 m2 office with two other emeriti. One of them is Ole Didrik Laerum, the one who got me to Bergen in the first place. Each of us have a desk, one microscope, and one computer. Rarely are all three of us present at the same time, so the space is adequate. I hope to accomplish a few more things yet. The last years have come and gone like snow in April. In the last decade, my beloved wife, Kari, who has been a source of love and order for our close family, started to lose us and herself. She was diagnosed with dementia. She was so full of life, a loving mother, and a talented artist. Her care enabled my career and family life, so it was difficult when the tables were turned, and I found myself caregiving for her. My close-knit family has helped me greatly in coping with this challenging time, for which I am endlessly thankful. She has transitioned to a care home, but I visit her frequently, and she frequently comes back to herself. Her face often lights up when she sees a frequent visitor, whom she sometimes recognises as ‘Sverre’. I have told myself, ‘De-mentia is not A-mentia’, and for Kari, that is true. She has retained her use of language. On one recent visit, she exclaimed, ‘There are more people here!’ ‘Just me’, I said. ‘Well’, Kari said. ‘I am here too!’ For the last 50 years, she has been a wonderful companion and remains one now, even as we come to the end. The challenge I was given by the Free Neuropathology has helped me to concentrate on times past. The time spent has been valuable. I have by now wound up most items that I had put aside. Private letters, reports, material related to international co-operation, journals, books, folders with obituaries, reprints, and photographs. I thank Werner Paulus and Tibor Hortobágyi for this opportunity to illuminate my existence. Brian Trapp helped me with language corrections and inputs. A mild acceptance of how things have turned out, the ‘you could have done better’ have been overtaken by the perception of the facts of My Way. All the way, Robert Frost’s poem (The Atlantic Monthly, 1915) has been with me.
THE ROAD NOT TAKEN
With my friend, Tore,
Copyright: © 2021 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |