|
|
|
Free Neuropathology 2:27 (2021) |
|
Reflections |
|
Lessons learned from a career in neuropathology |
|
Roy O. Weller |
|
Faculty of Medicine, Southampton University, United Kingdom |
|
Address for correspondence: |
|
Submitted: 09 October 2021 Accepted: Accepted: 12 October 2021 Published: 25 October 2021 |
|
Additional resources and electronic supplementary material: supplementary material |
|
Keywords: Clinical neuropathology, Research, Students, Lymphatic drainage of the brain, Alzheimer’s disease, Cerebral amyloid angiopathy, Personal reflections, Family |
|
Introduction Writing an Autobiography was probably the last thing on my mind when I was asked to add mine to a growing list of personal accounts published in Free Neuropathology. It was no easy task to summarise my life in what I hope will be an interesting account for my readers. But, in the end, it has been rewarding for me at least to state what I think have been the important events, ideas and attitudes that have shaped my life and career in Neuropathology and to recognise some of the many people who have taught, influenced, helped me and offered their friendship over many years. As for the lessons learned, I hope they will become apparent as the account proceeds. Early years I was born in a South-Eastern suburb of London a year before the outbreak of the Second World War. Our house was two miles from the River Thames and Woolwich Arsenal but, despite this vulnerable position, our home suffered no damage from bombing. It did mean, however, that there were many periods when we spent nights in an air-raid shelter in the garden. I was too young to appreciate the deprivations of wartime England and the terrible time that my parents endured. The first school that I attended was partially destroyed by a V2 rocket and my classmates and I transferred to another school that had already been half destroyed by incendiary bombs. Despite this, all I can remember is a very happy childhood and education. At the age of 11 years, I transferred to a Grammar School in the centre of London, close to Tower Bridge. Founded in 1588, St Olave’s and St Saviour’s School that I attended had moved to a beautiful Early Victorian building in 1840 to make room for the construction of London Bridge station. The school is now in Kent and the original 1840 building is a 5-star hotel. I received a classical education with some concentration on languages; English, Latin, French, Greek and German have all been of great value to me, not only in medicine but also when I travelled widely in Europe as an undergraduate and during my postgraduate career. Science was also strong in my school and this enabled me to enter Guy’s Hospital Medical School in London as a medical student in 1956. My motivation for studying medicine was mainly the attraction of the basic sciences, particularly biochemistry, but I soon became enthralled with patient contact and clinical medicine. During my undergraduate studies I spent a year, gaining a Bachelor of Science degree in Anatomy under excellent tuition from Roger Warwick and Peter Williams who were both Editors of Gray’s Anatomy. I visited many of the Medical Schools in London for lectures and demonstrations during this year which gave me a clear insight into academic medicine and was probably a major factor in determining my postgraduate career in Neuropathology. Early postgraduate career Having completed my medical education, I took a teaching post in Anatomy at Guy’s and a research post with Professor John Cavanagh (Figure 1) to work on peripheral neuropathies, most especially experimental diphtheritic neuropathy in chickens (much to the amusement of my friends). My objective was to determine the ultrastructural sequences involved in the initial stages of segmental demyelination. John was an ideal supervisor at the beginning of my research career as he would present me with a problem and leave me to solve it, only giving advice when asked; John also taught me the basis of the scientific method and how to view earlier findings in my field with scepticism. I was introduced to the technical aspects and analysis of transmission electron microscopy (TEM) that was still a relatively new technique. The skills I learnt at that time have served me throughout my career. In my first paper in 1965 1, I showed that, prior to breakdown of the myelin sheath in segmental demyelination, acid phosphatase-containing lysosomes gathered in cytoplasmic pockets on the inner aspect of the myelin sheath. This gave some indication of how the myelin was removed without damaging the axon that it encompassed.
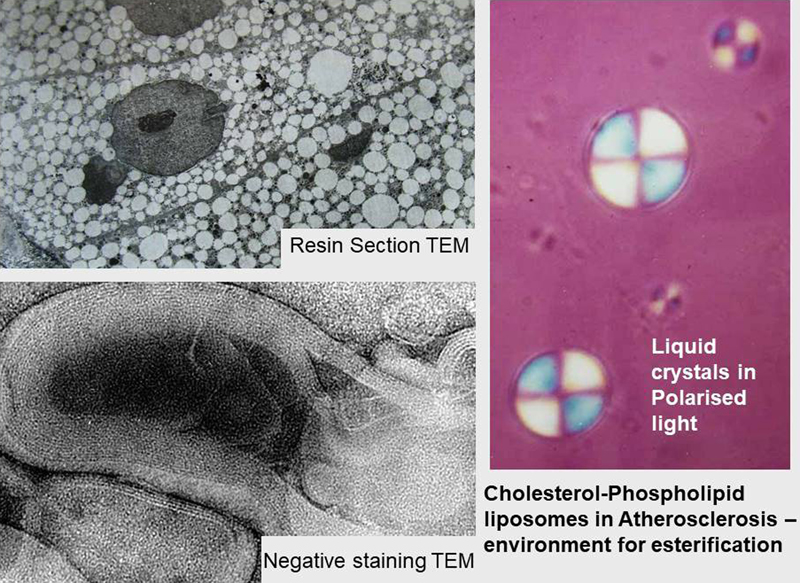
Figure 1. John B Cavanagh 1997. My second post at Guy’s was with Professor Colin Adams, who was a lipid histochemist of world renown. He had a gift for adapting techniques to identify individual lipids, particularly in atherosclerosis and in multiple sclerosis. The major task for my PhD was to define the ultrastructure of intracellular lipid accumulations in atherosclerosis. This was no easy matter as the lipids are soluble in the organic solvents used in preparation for TEM. By a combination of polarised light microscopy, negative staining and routine TEM (Figure 2), I identified the multi-lamellated structure of the liquid crystalline lipid droplets that appeared to be the template for esterification of the cholesterol that they contain 2,3. It was during this period, that I started my education in Clinical Neuropathology with Henry Urich at the London Hospital. Henry’s teaching was direct and very suitable for me in the early stages of my career.
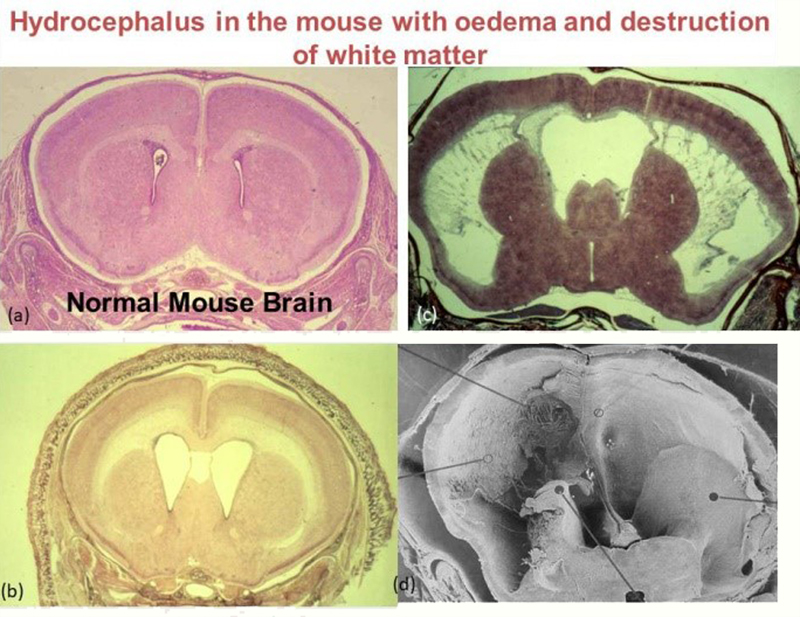
Figure 2. Intracellular lipid droplets in atherosclerosis. Top left and then clockwise: TEM showing removal of lipid from cells during preparation. Birefringent liquid crystalline droplets of cholesterol and phospholipids isolated from an atherosclerotic lesion. Similar droplets examined as negative stained TEM showing lamellated structure 2,3. US-NIH-Fellowship at the Albert Einstein College of Medicine in New York Having gained my Ph.D. in 1967, it was time for a change, so my wife, Francine, and our two children, Adrienne, aged three and Timothy aged two years embarked on a boat for the USA. I had gained an US-National Institutes of Health (US-NIH) Postdoctoral Fellowship in Neuropathology with Dr Robert Terry at the Albert Einstein College of Medicine in New York. It was a very different but highly stimulating environment. Bob Terry was very generous with his time and ideas and this led to numerous interesting discussions about pathology of the nervous system. I learned much about clinical neuropathology from Bob and his colleagues, especially Kinuko Suzuki. For my research, I investigated the effects of acute hydrocephalus upon the brains of adult rabbits, infant dogs and in biopsies from very young children. My main teacher and collaborator in this project was Henryk Wisniewski who was an excellent animal surgeon and experimenter. Henryk devised a technique for producing hydrocephalus by injecting highly viscous, but non-inflammatory, silicon oil through a lumbar intrathecal catheter into the posterior fossa of adult rabbits and young dogs to compress the fourth ventricle and impede the drainage of CSF. I examined the brains in large-area 1 μm resin sections and by TEM. By sequential examination of the olfactory bulbs in adult rabbits and the walls of the lateral ventricles in infant dogs, we showed that as the ventricles dilate in the early stages of hydrocephalus, the ependyma ruptures and the flow of CSF into the periventricular white matter results in extensive CSF oedema with a mild degree of axonal degeneration. As hydrocephalus progresses, the CSF oedema subsides and the periventricular white matter displays extensive reactive astrocytosis, and axonal degeneration 4,5. A similar sequence of changes was revealed in biopsies from very young children with acute hydrocephalus 6. These observations suggested that treating children with shunts in the early stages of hydrocephalus would preserve axons and improve prognoses. Our findings were confirmed several years later when CT scans clearly revealed the presence of periventricular oedema in the acute stages of hydrocephalus. The sequence of changes of ependymal rupture, increasing CSF oedema and destruction of periventricular white matter is well demonstrated in a congenital model of hydrocephalus in mice that I bred later when I returned to Guy’s (Figure 3).
Figure 3. Progressive Hydrocephalus in the mouse showing (a) Normal mouse brain. (b) Early stages of hydrocephalus with CSF oedema of the white matter. (c) Severe oedema with destruction of the white matter and preservation of grey matter. (d) SEM showing almost total destruction of the cerebral white matter and rupture of the ependyma 7. My family and I spent a most rewarding year in New York. We lived in an apartment block in the Bronx very near the Einstein. As the months progressed we adapted to the very low temperatures in the winter in New York and the high temperatures and humidity in the summer. Our children became bilingual through contact with their friends at nursery school; they would speak with a New York accent and vocabulary between themselves and their friends but spoke English when communicating with Francine and me. We explored Manhattan widely and travelled to a variety of cities in the US to appreciate the diversity of the country. As we finally left New York in September 1968, we travelled by Greyhound bus to a conference in New Orleans before flying home – quite an adventure! I have very pleasant memories of the team of people with whom I worked at the Einstein (Figure 4). Through meetings of the American Association Neuropathologists (AANP), I remained in contact with Bob Terry for many years. Similarly, I retained contacts with Henryk Wisniewski, who had a very successful research career in demyelinating diseases and in Alzheimer’s disease.
Figure 4. Neuropathology group at the Albert Einstein College of Medicine 1968. First row, left to right: Drs Kinuko Suzuki, Mariene Lenger, Krystyna Wisniewska, Kytja Voeller and Anne Johnson. Second row, left to right: Drs Roy Weller, Henryk Wisniewski, Robert D. Terry, John Andrews, Jan Leestma and Ivan Herzog. Third row, left to right: Drs Steven Shayvitz, Michael Shelanski, Richard Snyder, John Prineas and Carlos Araoz. I have Kinuko-Suzuki to thank for my much of my training in diagnostic neuropathology and for her friendship that lasts to the present day. Of the younger members of the team, Michael Shelanski became Professor of Pathology at Columbia University in New York, John Prineas returned to Australia as a Neurologist in Sydney to continue his research on multiple sclerosis. Jan Leestma developed a very successful career in Forensic Neuropathology in Chicago; we are still in contact. After the photograph in Figure 4 was taken, Cedric Raine and Peter Spencer joined Bob Terry’s Department. Cedric developed a very successful career in multiple sclerosis research. Peter Spencer moved into Toxicology and together with Herb Shaumburg published a large multi-author book on Clinical and Experimental Neurotoxicology to which my colleague in Southampton, John Mitchell, and I contributed a chapter on a fascinating Mexican segmental demyelinating neuropathy due to ingestion of fruit and seeds of the Buckthorn plant (Karwinskia humboltiana) 8. It was rumoured that Mexican women would administer small amounts of the fruit or seeds to their husbands so that that they would feel weak and stay at home rather than spending the evenings drinking with their friends. Return to England In the fall of 1968, my family and I returned to England and I was appointed Lecturer in Pathology at Guy’s Hospital Medical School. I continued my close connections with Neuropathology by working in Peter Daniel’s Department at the Institute of Psychiatry in London. My joint appointment allowed me to learn much from Peter and from his colleagues. I also broadened my knowledge of clinical diagnostic pathology in general by engaging in the analysis of renal biopsies in collaboration with David Turner, a fellow Pathologist, and Renal Physicians, Stewart Cameron and Chisholm Ogg. This was a very fruitful time as correlation of the ultrastructural changes in renal biopsies with clinical syndromes was still in its early stages. Together with Barry Nester, I published mid-20th-century diagnoses for three post-mortem kidneys that had been preserved by Richard Bright in the 1820-30s 9. For me, this was a valuable time for establishing contacts in London and elsewhere in the UK and for considering my ultimate career. During the 1970s I started to regularly attend conferences abroad, mainly in Europe. This was essential for my continuing education and for maintaining contact with colleagues. I also benefitted by visiting many interesting countries and cities and meeting a great variety of different people. In 1971, I was fortunate to spend a short period in Berlin with Jorge Cervós Navarro that not only greatly increased my experience in neuropathology, but also allowed me to appreciate life in East Berlin, then in the Soviet bloc, and to visit the famous Pergamon Museum and its marvellous exhibits from Ancient Greece. It was through Jorge that I was introduced to the German Neuropathology Society. At this time, trips to interesting nearby attractions were a feature of the German conferences. Following a meeting in Heidelberg, for example, we visited Bad Dürkheim and the Dürkheimer Wurstmarkt (sausage market but in reality the world’s largest wine festival) (Figure 5). I retained contact with Jorge for many years and together we wrote a book on the “Pathology of Peripheral Nerves” that was published in 1978.
Figure 5. Bad Dürkheim (Germany), 1971, Fotoschiessen. As our colleague in the centre hit the target, the photo was taken with Jorge Cervós Navarro (left) and Roy Weller (right). The text book – “Pathology of Peripheral Nerves” (lower right) – was one product of my collaboration with Jorge. University of Southampton School of Medicine In early 1972, the opportunity arose to join the new Medical School that had been established in 1971 in the University of Southampton on the southern coast of the UK. It was a combined National Health Service (NHS) and University post for which the job description was brief and to the point: “Provide a diagnostic service for Neuropathology for the Wessex Regional Neurological Centre, teach Neuropathology and perform Research”. Following a thorough assessment of the post and the environment in Southampton, I applied and was appointed to start in January 1973. I have never regretted the move to Southampton. My family and I moved to live in Winchester, just north of Southampton; an ancient Roman city and mediaeval capital of England, one hour by train from London and 40 min by car from Heathrow. Clinical Neuropathology Service The 30 years that I worked in Southampton were delightful and I greatly appreciated the friendship of my colleagues. My relationships with Clinical and University colleagues worked through collaboration and mutual respect for each others’ areas of expertise. The two Neurosurgeons, Jason Brice and John Garfield, who were working in the Wessex Neurological Centre (there are now 14 Neurosurgeons) when I arrived and the three Neurologists, Stanley Graveson, Peter Robinson and Lee Illis (now 21 Neurologists) had very professional attitudes. Their aim was clearly to provide an excellent clinical service that required a high quality and rapid diagnostic Neuropathology service from me, together with weekly Multidisciplinary Team Meetings to discuss individual patients. I had soon realised that my clinical colleagues had many challenges and that my role was to provide them with all the assistance that I could. As we built up an atmosphere of mutual collaboration my life in Southampton remained stable and pleasurable. Neuropathology in Southampton had a defined laboratory with its own staff but it was part of a larger Department of Histopathology/Cell Pathology with Prof Dennis Wright at its head. This arrangement had many advantages, not least the wide range of expertise and facilities. Regular clinical pathology and research meetings allowed the sharing of ideas and information about new developments. Social activities were enthusiastically pursued which helped with cohesion of the Department; there was also a constant circulation of Pathology trainees from the UK and other countries through Neuropathology providing a very interesting international environment. There were some disadvantages, such as competition for space and staff but the advantages heavily outweighed the disadvantages. From the time that I arrived in Southampton, I was responsible for Neuropathological Services for the Wessex Region of some 3 million people. Richard Goodbody, who had long been involved in brain tumour diagnoses and in analysing post-mortem brains, very helpfully continued as part-time in this field. I covered brain, nerve and muscle biopsies, ophthalmic biopsies together with post-mortem brains and teaching sessions for trainee pathology staff, clinicians, medical students and nurses. My workload was very high and I was careful to prioritise so that I could cover all fields for which I was employed. I soon acquired a very extensive experience of diagnostic neuropathology and felt able to compile textbooks on Neuropathological subjects (see later section) During the 1970s, there were rapid advances in clinical neurology, neurosurgery and neuroradiology with the introduction of CT scanning and MRI that had a huge influence on diagnostic neuropathology. Tumours and other lesions in the brain and spinal cord were well visualised, but instead of reducing the workload in Neuropathology, the number of biopsies steadily increased. There were significant advances in the technical aspects of Neuropathology. Immunocytochemistry, for both frozen and paraffin sections, and later genetic techniques were incorporated into the diagnostic Pathology and Neuropathology services. Ray Hunt and Barbara Davis led the technical team for Neuropathology and together with Phillip Steart, Jean Buontempo and Judy Mepham were always very anxious and able to advance the scope and quality of the service. Trainees, fellows and staffing in clinical neuropathology In addition to trainee Pathologists and Neurosurgeons from Southampton rotating through Neuropathology, a number of Fellows from other Institutions joined me over the years. Ricardo Campora came in the 1970s from Seville and worked with me for a year before returning to Spain to practice Neuropathology. Ricardo is extremely able and became Professor of Pathology and head of Department in Seville. I am still frequently in touch with Ricardo and his wife Conchita. For a few years I taught a Neuropathology course in Seville and received tremendous hospitality there; we also meet on occasion in London. Laura Chavez from Mexico City worked with me as did Markus Tolnay from Basel and Jim Lowe from Nottingham; all have had successful careers in Neuropathology and we remain in contact. In the 1980s John Grant came to work with me as a trainee in Neuropathology. This changed my life as it gave me much more flexibility in how I spent my time. John was always very reliable and a great inspiration; when he left Southampton John gained experience in Zürich before embarking on a very successful career as a Consultant Pathologist in Cambridge, where he has been Head of Department for a number of years. Patrick Gallagher was a Consultant Cardiac Pathologist who also joined the Neuropathology diagnostic team which again was of great benefit to the Service. David Ellison arrived as a trainee in Neuropathology in the early 1990s and soon made significant progress in research into the genetics of brain tumours. David became a Consultant Neuropathologist in Southampton before gaining a Professorship in Newcastle and then moving to Memphis, Tennessee, to pursue his world-renowned career in the pathology and genetics of childhood brain tumours. Soon after David Ellison left Southampton, James Nicoll came from Glasgow; he brought tremendous expertise in dementia research, particularly in the roles of microglia. James has made a considerable contribution to the study of post-mortem brains in patients following immunotherapy for Alzheimer’s disease. I retired in 2003 and left Clinical Neuropathology in Southampton in the extremely capable hands of James Nicoll. After my retirement the Clinical Neuropathology Service was augmented by two very competent Consultants, Mark Walker and Mark Fabian. Research In this account, I take a personal view of how my research progressed in Southampton and I include the names of some, but by no means all, of the many people involved. Serendipity and the views of my colleagues worldwide played a major role in how my research progressed. I am indebted to the students and postdocs who contributed so much to our research programme and stimulated its progress. A number of themes initially emerged from my research including structural changes in Peripheral Neuropathies and Myopathies, regeneration in nerves and muscle and detailed analyses of brains with Growth Hormone-related Creutzfeldt-Jakob disease. Postdoctoral fellows, Lawrie Haynes and Gary Caine used tumour biopsy material to investigate the effects of pharmacological agents on tissue culture preparations of gliomas. With the introduction of immunocytochemistry for paraffin sections developed by Dennis Wright and his colleagues in our department, we were able to investigate the uptake of proteins by normal and neoplastic astrocytes. Major research themes Four Major Interconnected Themes dominated most of my research in Southampton and led to advances and revision of Scientific Concepts. (i) The structure of the leptomeninges and their relationships to the brain. (ii) The detailed pathways for lymphatic drainage of the brain. (iii) The relationship between age-related failure of lymphatic drainage and the accumulation of amyloid-β (Aβ) in artery walls in Cerebral Amyloid Angiopathy (CAA) and in the brain in Alzheimer’s disease. The latter advances were mainly through the work of Roxana Carare, who following completion of her PhD formed her own research group that included Cheryl Hawkes and many others (Figure 6). Roxana’s work progressed to identify potential therapies for Alzheimer’s disease and CAA and to early Clinical Trials. Roxana is now Professor of Clinical Anatomy in Southampton. (iv) Through a very fruitful and lasting collaboration with Britta Engelhardt in Bern, Switzerland, we also investigated the relationship between lymphatic drainage of the brain and neuroimmunological diseases with relevance to disorders such as Multiple Sclerosis. A list of over 200 peer-reviewed papers that my colleagues and I published can be obtained from PubMed. I will only cite a few of those papers in the following text.
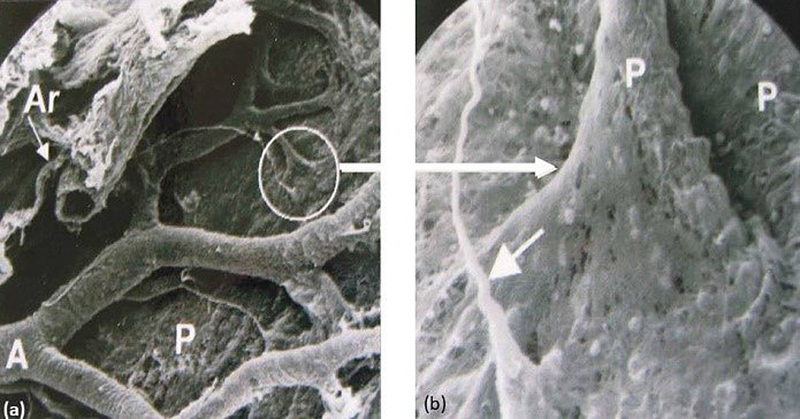
Figure 6. Roxana Carare and her group. Students and technical staff with Cheryl Hawkes (right front) next to Roy Weller and Roxana Carare. Why do research? For me, the main reasons for engaging in research are to satisfy my curiosity and to take the opportunity to present unique data to colleagues at Scientific Conferences and in Scientific Journals. I had been exposed to research during my BSc course at Medical School and in my early postgraduate years working with John Cavanagh and Colin Adams. Bob Terry encouraged research in all his fellows and led by example. By the time I arrived in Southampton, research was well ingrained within me. Southampton has been, for me, an ideal environment for research through excellent facilities and multiple disciplines within the University available for consultation and collaboration. With a heavy diagnostic workload in biopsies and post-mortem brains, I was exposed to many unsolved problems in Human Neurobiology and Neuropathology that provided a stimulus for hypothesis-driven experimental research. Another important stimulus for research was the requirement that each Medical Student in Southampton perform a research project from October to May in the fourth year of the course. This meant that a constant stream of two or three highly intelligent, hard-working enthusiastic 22 year old students worked in Neuropathology each year with their individual projects but collaborating closely with BSc and PhD students, Post-Docs and Research Fellows. My strategy was to begin a research theme with straight-forward observational projects for the Medical Students that generated hypotheses to drive experimental research for the PhD students and Postdoctoral Fellows. Many students presented papers at British Neuropathological Society (BNS) Meetings and published papers in peer-reviewed scientific journals. All groups benefitted their future careers by acquiring skills in spoken and written communication. How did I benefit from students and others involved in research projects? The students educated me by their observations, the papers that they read and from the knowledge that they had gained in their recent medical education. Retaining an open mind was very important: each student was given a problem to solve but advised not to read the previous literature until they had results and could form their own opinions. There were numerous occasions upon which students burst into my office crying “The literature is wrong!” In this way they built up a healthy scepticism for previous findings. I advised students not to believe anything they read and not to believe anything that I told them until they had verified it for themselves. Structure of the human leptomeninges and their relationship to the brain and blood vessels Although my interest in fluid balance in the brain started with my work on Hydrocephalus in New York, it was reawakened in Southampton by student projects using Scanning Electron Microscopy (SEM) to examine human leptomeninges. Margaret Upton 11 identified the intricate pattern of channels by which CSF passes through arachnoid granulations to the blood in venous sinuses. Margaret Hutchings made a startling discovery in 1986 using SEM on the surface of human brain by showing that the pia mater is reflected from the surface of the brain on to arteries and veins in the subarachnoid space thus separating CSF in the subarachnoid space from the brain 10 (Figure 7). This exploded the longstanding concept that there was a direct communication between CSF and brain. Margaret also showed that erythrocytes in Subarachnoid Haemorrhage do not penetrate the pia mater to enter the brain. We later confirmed that solutes and macrophages do pass through the pia mater that forms a continuous sheet on the surface of well-fixed normal brain as shown by Ruth Alcalado 12. No pores in the pia have been identified by TEM and the holes seen in SEM images are probably post mortem or fixation artefact.
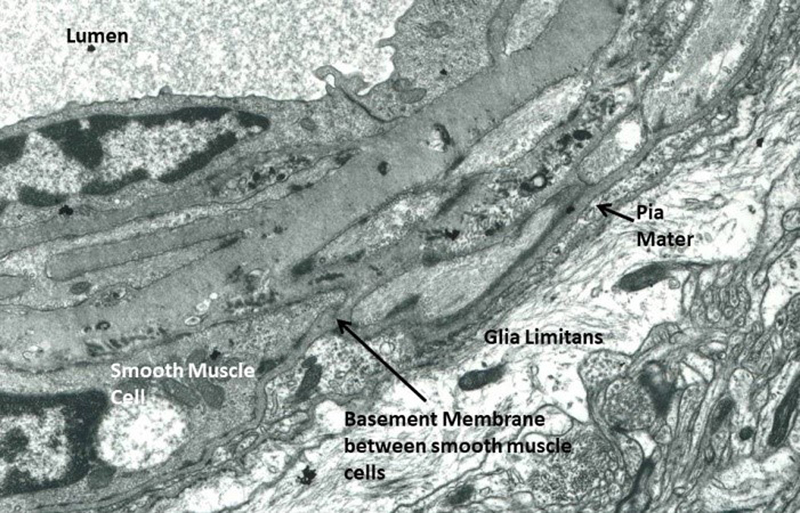
Figure 7. SEM of the meningeal surface of the human cerebral cortex showing the arachnoid mater (Ar) and branches of an artery (A) spreading over the surface of the pia mater (P). The circle depicts the point at which a branch of the artery enters the cortex and how the pia mater is reflected on to the artery thus separating the subarachnoid space from the brain. (b) is an enlarged view of the reflected pia mater (P). Artefactual holes are seen in the pia in this post-mortem specimen. Arrow (lower left) identifies a filiform trabecula crossing the subarachnoid space 10. In the 1980s, En-Tan Zhang came from Beijing to work with me in Southampton. En-Tan is a medically qualified Anatomist and he made a major contribution to establishing the relationships between the leptomeninges and arteries as they enter the brain. Using well fixed human biopsy brain material, En-Tan showed that a single layer of pia mater coats arteries as they enter the surface of the cerebral cortex and that there is no “periarterial space” between the glia limitans and the artery wall 13. Astrocytes in the glia limitans, pia mater, smooth muscle cells and endothelium together with the intervening layers of basement membrane form a compact structure, with no perivascular space (Figure 8). The long-described Virchow-Robin spaces do not exist in the cortex and if present they are mainly due to swelling of astrocyte processes from poor fixation as emphasised by Milton Brightman in the 1960s. En-Tan’s observations completely changed our perception of the relationship between CSF and the brain. Subsequently, Roxana Carare’s group showed that tracers from the CSF enter the brain, not along perivascular spaces (as there are none) but along basement membranes between the glia limitans and the single layer of pia mater that surrounds each artery as it enters the brain 14. Basement membranes between smooth muscle cells in the tunica media were later shown by Roxana Carare to be the pathways for flow of fluid and solutes out of the brain. Due to the absence of periarterial spaces, there are no periarterial pathways for the entry of inflammatory cells from the CSF into the brain. Periarterial spaces do form in other the parts of the brain, especially in the basal ganglia and around arteries in the white matter. At both of these sites, arteries are surrounded by two layers of pia mater and the periarterial space develops between them 15,16.
Figure 8. TEM of a well-fixed human cortical artery showing part of the wall and surrounding brain. The layers of glia limitans, pia mater, smooth muscle cells and endothelium adjacent to the lumen are all compacted with no preriaterial space (see also 13). Lymphatic drainage of the brain There are two extracellular fluids associated with the brain and spinal cord: (i) CSF in the ventricles and subarachnoid spaces and (ii) Interstitial Fluid (ISF) in the extracellular spaces of the brain and spinal cord. Pathways for lymphatic drainage of CSF are almost completely separate from lymphatic drainage of ISF from the brain. Lymphatic drainage of CSF Shinya Kida, a Neurosurgeon from Japan, joined us in Southampton in the early 1990s and embarked upon a search for the drainage pathways for CSF in the rat with a medical student Andreas Pantasis. Lymphatic drainage of CSF to cervical lymph nodes had been demonstrated by Schwalbe in 1869, and Bradbury and Cserr showed in the 1980s that lymphatic drainage of CSF occurred through the cribriform plate of the ethmoid bone but the details were unclear. Shinya and Andreas 17 demonstrated direct drainage of Indian ink tracer from the subarachnoid space along distinct vessels that pass through the cribriform plate alongside olfactory nerves into the nasal submucosa en route to cervical lymph nodes. Such channels were also shown to exist in post mortem humans brains by the injection of Myodil tracer into the CSF 18 and by reconstruction from serial sections of the human cribriform plate and nasal mucosa by Effie Djuanda in her fourth year medical student project 19. Other channels for drainage of CSF identified in these studies included dural lymphatics and the sheaths of cranial nerves 17,20. Drainage of CSF by the nasal route has been demonstrated in humans using PET scanning 20. The balance between lymphatic drainage of CSF to cervical or lumbar lymph nodes and drainage through arachnoid granulations has yet to be determined. The small size and paucity of arachnoid villi in the rat suggests that they are quantitatively less important for the drainage of CSF in rodents than lymphatic drainage. In humans, arachnoid granulations do not develop until the age of two years which suggests that lymphatic drainage may also be an important route for the drainage of CSF in Humans. Arachnoid granulations may compensate for variations in CSF pressure that occur with change of body position; this speculation still requires direct verification. Lymphatic drainage of Interstitial Fluid (ISF) and solutes from the brain There are no conventional lymphatic vessels in the brain or spinal cord. In the 1980s Helen Cserr and her colleagues 21 injected minute amounts of radioactive human serum albumin as a tracer into the basal ganglia of the rat brain, and showed that the tracer drained to cervical lymph nodes along the walls of cerebral arteries. Only 10-15% of tracer leaked into the CSF emphasising that the pathways for lymphatic drainage for CSF from the subarachnoid spaces are separate from drainage of ISF from the brain itself. En-Tan Zhang attempted to define the drainage pathways for ISF in more detail in the late 1980s by injecting Indian ink particles directly into the basal ganglia of the rat brain. The ink particles tracked along the outside of arteries, were taken up by perivascular macrophages and remained in situ 22. This technique did not identify the drainage pathways for ISF but did identify a pathway that was later used for Convection-Enhanced Delivery (CED) of drugs directly into the brain 23. The results from En-Tan’s work led to discussions with Alex Roher from Phoenix, Arizona, who suggested that cerebral amyloid angiopathy (CAA) may be related to periarterial lymphatic drainage of the brain. We subsequently published a joint paper in American Journal of Pathology in 1998 with the title “Cerebral Amyloid Angiopathy: Amyloid β Accumulates in Putative Interstitial Fluid Drainage Pathways in Alzheimer’s Disease“ 24. Breakthrough A major breakthrough in our research on lymphatic drainage of the brain came from the work of Roxana Carare in her PhD project that I supervised jointly with Hugh Perry. Roxana injected formalin-fixable fluorescent dextrans or soluble Amyloid-β (Aβ) into mouse brains and examined the drainage pathways by confocal microscopy. In her paper, “Solutes, but not cells, drain from the brain parenchyma along basement membranes of capillaries and arteries: significance for cerebral amyloid angiopathy and neuroimmunology” 25, Roxana defined the pathways for the lymphatic drainage of fluid and solutes from brain tissue that we later termed the “Intramural Peri-Arterial Drainage (IPAD) Pathways” 14. Following the injection of minute volumes (0.5 μL) of tracer into the caudate nucleus of the mouse brain, tracer spread through the extracellular spaces of the brain and within 5 mins had entered the lymphatic drainage pathway (IPAD) in the basement membranes of capillaries and basement membranes between smooth muscle cells in the tunica media of cerebral arteries. The drainage pathway (IPAD) extended into leptomeningeal arteries. No tracer was seen around veins in normal animals following intracerebral injections although animals with age-related impairment of IPAD did show some tracer around veins 26. Confusion Considerable confusion in the scientific literature has resulted from the injection of excessive volumes of tracer into the mouse brain that results in leakage of tracer into the CSF giving the false impression that lymphatic drainage of the brain occurs via the CSF. Furthermore, injecting excessive amounts of tracer into the brains of mice and not examining the animals until 1 hour later, after IPAD is complete, result in pooling of tracer around veins and has given the erroneous impression that lymphatic drainage of the brain is along the walls of veins. Supporting evidence for IPAD in the human brain CAA in mice and humans provides convincing supporting evidence that IPAD is the route for lymphatic drainage of fluid and solutes from the brain parenchyma. (i) The pattern of distribution of Aβ in capillary and artery basement membranes in CAA exactly mirrors the distribution of Aβ and other tracers in IPAD pathways in the animal experiments 27. (ii) CAA occurs in transgenic mice in which there is excessive production of Aβ in neurons; in these mice the origin of the Aβ is definitely from cells in the brain 28. Age-related failure of elimination of Aβ by IPAD is associated with CAA and Alzheimer’s disease By combining experimental studies in the mouse with observations of human CAA and Alzheimer’s disease, the following main conclusions have been reached as summarised in 29. IPAD is impaired by age-related changes in the walls of arteries and by CAA 26. Both theoretical models and experimental studies suggest that the motive force for IPAD is derived from waves of smooth muscle cell contraction (Vasomotion) that pass along the walls of cerebral arteries in the opposite direction to blood flow, but in the same direction as IPAD 29,30. Age and the presence of apolipoprotein E ε4 (APOE4) is associated with the impaired IPAD 31 and this correlates with age and APOE4 as major risk factors for Alzheimer’s disease and CAA in humans. CAA also affects capillaries; painstaking cutting of hundreds of serial transverse sections of arteries in regions of capillary CAA by Hong Yeen Yow (BSc student) suggest that capillary CAA is associated with thrombotic occlusion of penetrating cortical arteries 19. Age-related impairment of IPAD appears to be associated with loss of Homeostasis in the brain as reflected by accumulation of fluid in White Matter Hyperintensities on MRI and the failure of elimination of Aβ with age and in Alzheimer’s disease. Dilatation of periarterial spaces in the white matter is associated with CAA and probably reflects failure of IPAD. Translational neuroscience: Therapeutic strategies for CAA and Alzheimer’s disease: Facilitating IPAD For the past 20 years there have been many trials of Immunotherapy for Alzheimer’s disease but with little success in reducing cognitive decline in the treated patients. Studies of post mortem brains following Aβ immunotherapy have shown that although Aβ plaques are removed from the cerebral cortex both arterial and capillary CAA are increased in severity 32,33. It does appear that age-related failure of IPAD is a rate-limiting step in Aβ immunotherapy and this emphasises the importance of facilitating IPAD in the treatment of CAA and Alzheimer’s disease. Potential new therapeutic strategies could act via IPAD by modulating vasomotion as the postulated motive force for IPAD. This may be accomplished by stimulating contraction of vascular smooth muscle cells directly or through their nerve supplies. Another therapeutic possibility is the use of chaperone molecules to enhance the clearance of Aβ along the basement membranes that form the IPAD pathways 29. Lymphatic drainage of the brain and neuroimmunology The brain is an immunologically privileged site 34 as shown by experiments in which skin allografts implanted in the brain survive for longer periods than allografts in other organs. Rapid rejection of brain allographs does occur, however, when similar allografts are implanted into the animal’s skin. The leptomeninges and CSF spaces do not show the same immunological privilege as brain tissue 34. One of the major differences is that CSF drains directly into lymphatic vessels that allow fluid, antigens and antigen presenting cells to drain directly from the CSF to lymph nodes. IPAD pathways are too narrow to allow the traffic of APCs from the brain to lymph nodes 25. This may be a major factor in immunological privilege of the brain. Cervical lymph nodes have a major role in immunological reactions in the brain as shown by Marian Phillips, Dong Sun (Ph.D. students), Jonathan Lake and Michelle Needham (BSc medical students) and by Jon Laman and his group 35-37. Our first task was to enhance experimental autoimmune encephalomyelitis (EAE), in the cerebral hemispheres of rats so that accurate measurements of inflammation could be made. In most models of EAE following injection of antigen into the footpads, inflammation is concentrated in the spinal cord. However, Shinya Kida had previously shown that a wound to the surface of the rat cerebral cortex in the form of a cryolesion resulted in activation of perivascular macrophages throughout the cerebral hemispheres. Thus we showed that a cryolesion on the surface of the cortex in rats, 7 days post injection (dpi) of EAE antigens into the foot pad of the rat resulted in enhanced inflammation in the cerebral hemispheres at day 15 dpi. Removal of cervical lymph nodes on day 7 dpi resulted in a 50% reduction in EAE-related inflammation at day 15 dpi. These results suggest that cervical lymph nodes play a key role in cerebral EAE 35. Furthermore, adoptive transfer of lymphocytes from animals with cryolesion EAE resulted in a predominance of EAE lesions in the cerebral hemispheres in naive recipients rather than spinal cord EAE 36. Our involvement in neuroimmunology brought us into contact with Britta Engelhardt in Bern and her excellent studies on the receptor-mediated entry of lymphocytes into the brain through post-capillary venules. We are still in collaboration 34.
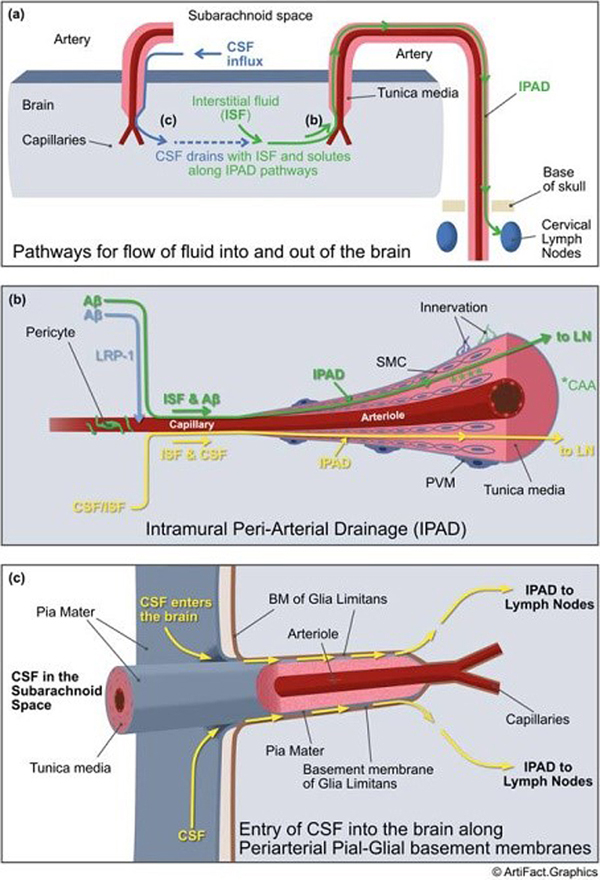
Figure 9. Summary of pathways for the flow of fluid and solutes into and out of the brain. (a) CSF flows into the brain along basement membranes shared by pia mater and glia limitans on outer surfaces of cortical arteries as they penetrate the brain. (b) Interstitial fluid (ISF) and solutes such as Aβ flow out of the brain to lymph nodes along IPAD pathways. (c) Details of the pathway by which CSF flows into the cerebral cortex along pial-glial basement membranes and then enters the brain to flow out along IPAD. Reproduced from 29. Original Design by Roy Weller and graphic by ArtFact Graphics. Award of the Gertrud-Reemtsma prize for International Translational Neuroscience 2020
Figure 10. The prize winners of the International Prize for Translational Neuroscience 2020: Left to right: Roy Weller, Maiken Nedergaard, and Mathias Jucker. I was greatly honoured by the award of the International Prize for Translational Neuroscience by the Council of the Gertrud Reemstma Foundation, administered by the Max Planck Society. The prize had been the K. J. Zülch-Prize until 2019 with many famous and worthy winners from 1990. I was awarded the prize together with Maiken Nedergaard and Mathias Jucker (Figure 10). My award was for the Southampton group’s “Ground-breaking scientific discoveries in the field of Lymphatic Drainage of the brain and its relationship to the aetiology of Alzheimer’s disease”. Of course the prize was awarded as much of the work performed by the many medical students, Ph.D. students and postdocs who worked with me in Southampton. Roxana Carare, Cheryl Hawkes, En-Tan Zhang, Shinya Kida and Dong Sun deserve special mention. Nevertheless, I felt it was a great honour for our group. Due to COVID-19 I could not attend the award ceremony on September 10th 2020 in Cologne, Germany, in person so I presented my lecture on Zoom. Management roles Throughout most of my career in Southampton I was involved in management in the NHS, Southampton University, and in Regional, National and International Organisations. It was part of my role to assist with the organisation of the Institutions to which I belonged. Furthermore I was rewarded by meeting many interesting people while performing management tasks. Within two years of my arrival in Southampton, I became Chairman of the whole of Pathology; this was in a very active period when all Pathology departments were moving into a newly-built Pathology block. At that time, in the mid-1970s, there were virtually no management courses and I learnt the necessary skills by observing others, how they chaired meetings, coordinated events and managed people so that the whole system ran smoothly and within budget. Soon after my promotion to Professor of Neuropathology in 1978, I became Deputy Dean of Medicine, which included, among other very interesting tasks, chairing the Committee for Selection of Medical Students; this gave me insight into the great variety of skills exhibited by the applicants to Medical School. Following my four-year term as Deputy Dean, I was appointed Chairman of the University Library Committee. Not only did this coincide with the delivery to the Library of the papers of the Duke of Wellington, but it was also the time that the Library acquired the papers of Lord Louis Mountbatten. The papers were markedly different in their condition. The Wellington papers were written with Indian ink on parchment such that they could be cleaned with large India rubber balls in sinks of cold water. The Mountbatten papers, on the other hand, were the fourth or fifth typed copy and required urgent transcription. For some 20 years I chaired various Regional and National Committees that ensured high quality training of Pathologists locally in Wessex and nationally through the Royal College of Pathologists. This was the time during which Neuropathology became an independent discipline within the Royal College of Pathologists and training and examinations were formalised. The establishment of the European Confederation of Neuropathological Society (EuroCNS) also allowed a European program of education and qualifications in neuropathology to be established. British Neuropathological Society The British Neuropathological Society (BNS) plays valuable roles in Neuropathology in the UK, both in monitoring the quality of clinical neuropathology and in encouraging research. The annual BNS scientific meeting is always very interesting and informative. In 2000, the BNS organised an International Neuropathology Society Congress in Birmingham, UK, with some 700 delegates. I chaired the committee that organised the scientific programme and David Graham was President. Due to the hard work and diligence of my many colleagues, the Congress was a great success. I was elected President of the BNS for 2001-2002. Major figures such as Hume Adams and David Graham in Glasgow, James Ironside and Jeanne Bell in Edinburg, Raj Kalaria in Newcastle, James Lowe in Nottingham, Seth Love in Bristol, Peter Lantos in London and many others played very significant roles in organising the BNS such that the BNS Conferences attracted significant numbers of Neuropathologist from Europe, USA and other countries. Editor of Neuropathology and Applied Neurobiology In 1975, John Cavanagh founded the Journal Neuropathology and Applied Neurobiology (NAN), that was adopted by the BNS as the Society Journal. I followed John as Editor in Chief of NAN between 1988 and 1998. This was a most rewarding time for me, organising the publication of research articles and review articles from an international body of authors. I learned much about the organisation of scientific journals and gradually NAN started to make a profit that has benefited the BNS financially. John had organised NAN with the original publishers, Blackwell, so that the profits were shared between the publisher and the BNS. Elizabeth Whelan was my main contact with the publisher and our relationship was excellent throughout my time as editor, largely due to Elizabeth’s skill and dedication. James Lowe followed me as editor in 1999 and there has been a succession of very successful Editors since. The Impact Factor of NAN has increased steadily from 3.9 in 2014 to 7.09 in 2019. Tom Jacques is the present Editor in Chief and NAN continues to play a significant role in international neuropathology. Editorial boards I have been a member of Editorial Boards of a number of Journals but the ones I remember in particular are the Boards of Brain Pathology, Acta Neuropatholgica and more recently, Free Neuropathology. Werner Paulus made a particular impression on me as editor of Acta Neuropatholgica; his very inspired decisions on which papers to accept for the Journal ensured that the Impact Factor for Acta Neuropatholgica rose to 18. Werner is the founding Editor in Chief of Free Neuropathology. Books published 1978-2013 I decided to harness the clinical material associated with the diagnostic service to publish a number of Text Books; this was partly as a self-education exercise. Some books I wrote alone or with another single author or I acted as Editor as well as a contributor. The rewards for my efforts were that writing and editing consolidated my knowledge of Neuropathology and built lasting friendships with multiple authors who showed great tolerance for my editorial changes. My first was “Pathology of Peripheral Nerves” by R O Weller and J Cervós-Navarro, published by Butterworths, London in 1978 and my second resulted from a course that we ran in Southampton: “Clinical Neuropathology.” A multi-author book edited by R O Weller, M Swash, DL McLellan and C L Scholtz, published by Springer Verlag, Berlin in 1983. The Japanese edition of “Clinical Neuropathology” was translated by T Mientani and published by Nishimura Co Ltd in 1983. “A Colour Atlas of Neuropathology” by R O Weller, published by Harvey Miller and Oxford University Press in 1984 and I contributed to “McAlpine’s Multiple Sclerosis”, by W B Matthews, E D Acheson, J R Bachelor and R O Weller. Edited by W. B. Matthews, published by Churchill Livingstone, Edinburgh in 1985. As part of “Systemic Pathology”, third edition: General Editor, W St C Symmers. I edited a multi-author “Volume 4: Nervous System, Muscle and Eyes”, published by Churchill Livingstone, Edinburgh in 1990. In 2002 I contributed to “Diagnostic Pathology of Nervous System Tumours”, by J W Ironside, T H Moss, D N Louis, J S Lowe and R O Weller, published by Churchill Livingstone, Edinburgh. I was appointed Director of the Book Series sponsored by the International Society of Neuropathology (ISN), publishing “Neurodegeneration. The molecular pathology of dementia and movement disorders”, second Edition. Edited by D W Dickson and R O Weller. Series director, R. O. Weller. Published by Wiley-Blackwell, Chichester, UK in 2011. As “Neurodegeneración”, the book was published in Spanish by Editorial Medica Panamericana, Madrid and Buenos Aires. The second book in the ISN series was “Muscle Disease: Pathology and Genetics”, second edition. Edited by H H Goebel, C A Sewry and R O Weller, Series director, R. O. Weller. Published by Wiley-Blackwell, Chichester, in 2013. I also contributed Chapters to a number of books including: Gray’s Anatomy, Greenfield’s Neuropathology, Clinical and Experimental Neurotoxicology and Histology for Pathologists. International Conferences and visits to other Neuropathology units Attending conferences was essential for my continuing education and for maintaining contact with colleagues. I also benefitted from visiting many interesting countries and cities throughout the world and meeting a great variety of different people. I regularly participated in the annual meetings of the British, French and German Neuropathology Societies and occasionally, the Scandinavian and Italian Neuropathology Society Meetings. I developed strong friendships with many members of those societies; Francoise Gray, Jacqeline Mikol and Homa Adle-Biassette to name but a few. A particular favourite conference of mine was the meeting of the Swiss Society of Neuropathology in St. Moritz every two years. Not only was the meeting held amidst beautiful scenery, the train journey was spectacular and there was ample opportunity for skiing and social interaction for discussing scientific data. I made many friends at these meetings. In addition to European meetings, I attended many conferences in the USA, including annual meetings of the American Association of Neuropathology. Other Conferences to which I contributed include those in India, Australia and Brazil. Photographs of many of the friends that I made at these international meetings appear in an excellent autobiography by Sam Ludwin 38. In 1988 Paul Kleihues kindly invited me to work for four months in Zürich. There was a most interesting group of young Neuropathologists working with Paul at the time, Otmar Wiestler, Andreas von Deimling and Adriano Aguzzi all of whom subsequently developed very successful careers and with whom I developed lasting friendships. While working for six weeks in Harare in Zimbabwe in 1991, I was involved mainly in teaching with occasional and most stimulating visits by car to other parts of the country. Martin Lewis was there at the time; he was an English pathologist working in Florida and we made a long tour around Zimbabwe in a 1968 Mercedes car that he had borrowed. Martin had extensive experience of Africa that is outlined in his book “The call of Africa”. Particularly rewarding were my visits to Beijing after my retirement at the invitation of Wei Wei Zhang. Quite apart from her tremendous hospitality, Wei Wei and her husband accompanied me on very interesting trips to other Chinese cities to meet many researchers and clinicians and to see the sights. I shall ever be indebted to Professor Zhang for introducing me to so much Chinese culture and cuisine. Post-retirement When I was about to retire, I realised that leaving what seemed like a lifetime in Neuropathology would be very difficult. Through the kindness of my colleagues, I took gradual retirement over 4-5 years moving to part-time involvement in clinical diagnostic neuropathology. I also remain involved on a consultancy basis with Professor Roxana Carare’s group who, following her Ph.D., developed a very successful research programme in Southampton with substantial grant income. I watched with great interest and some advice to the development of the IPAD work and I was involved in the discussion during the preparation of papers for publication. This was very helpful in my disengagement from neuropathology. In addition, I was asked to be chairman of the Biomedical Grants Advisory Board for the Alzheimer’s Society from 2013 to 2018 which kept me in touch with developments in research into Alzheimer’s disease. Living in Winchester gave me the opportunity to become a guide in the Cathedral. This 900-year-old building and its contents are a mine of information regarding British History in the last 2000 years. I edited the Winchester Cathedral Record that published research articles concerning the Cathedral for four years and I have been actively involved in researching the Cathedral for my own benefit and the benefits of my fellow guides and visitors. Family If it had not been for the support that I have received from my family, my career in Medicine and Neuropathology would not have been possible. My loving parents greatly encouraged me in my education and my wife, Francine, has offered her full support to me and to our moves around the UK and abroad. Throughout our 60 years of happy marriage, I have admired Francine’s independence and I am indebted to her for expanding my knowledge and involvement in the Arts, especially Music and Literature. We have both sung in choirs for almost the whole of our married life and continue to do so with great enjoyment. Our two children, Adrienne and Timothy have been a huge joy to us as have their spouses and our four grandchildren. Acknowledgments I would like to thank Professor Roxana Carare for all her help in the final editing and submission of the paper to Free Neuropathology. References
🎉 🎂 Celebrating Professor Roy Weller: 🎊 🥂 83 years old, over 5 decades of contributions to neuropathology Prof Johannes Attems Consultant Neuropathologist, Newcastle The first time I met Professor Roy Weller was at the British Neuropathological Society Winter meeting in 2001; in the break after the session where I had presented, he - the famous Professor - approached me - the unknown junior Doctor from Vienna - to discuss my talk! It was a nearly 20 minute discussion about the pathogenesis of cerebral amyloid angiopathy and Professor Weller listened to what I had to say and even produced some drawings illustrating the perivascular clearance. This first meeting with Professor Weller was hugely inspiring and motivating and certainly had a big impact on my decision to continue with research into neuropathology and I still think often back to this day in 2001! Naturally many more stimulating discussions between us followed (on all topics, professional and private) and I am looking forward to many more discussions in the future. Very many thanks for all your support Roy! Prof Roxana Carare Clinical Neurosciences, Roy Weller has catalyzed and energized the research into lymphatic drainage of the brain, inspiring and allowing us to pursue this with translational value for cerebral amyloid angiopathy and Alzheimer’s disease. He has taught me and many others the scientific method and testing hypotheses based on a solid overview of past and present observations on the human brain. The research group that I lead is a result of his continuous efforts to help with the direction of research, interpreting results, analytical, critical and forward-thinking discussions. We are grateful for his attention to detail and educating us to be researchers of high integrity and a deep quest for advancing science. Prof Mony de Leon Weill Cornell Medicine I am delighted to celebrate Professor Roy Weller’s 80th birthday by reflecting on his contributions to pathology and to radiology. However, using just a few words to do this, owing to his extensive and influential scholarly history, is a remarkably difficult but a highly refreshing task. Taking advantage of a personal and arbitrary starting point, my first encounter with Roy’s work was on his work in dementia and hydrocephalus. Weller, a longtime developer of animal models of hydrocephalus and an advocate for innovative dementia treatment options, would write in the J Neurol Neurosurg Psychiatry 1989, “When confronted with a patient with dementia, gait dyspraxia, and incontinence, we suggest that it is more realistic to look for a remediable hydrocephalic component to the illness than to consider that the patient must have either Alzheimer’s disease, multi-infarct dementia, or normal pressure hydrocephalus alone.” In the late 1970s I was a gerontology student studying Alzheimer disease (AD) and in 1980 I received an NYU-Brookhaven National Lab (BNL) neuroimaging post-doctoral fellowship. With the emergence of human imaging studies during the late 1970s, my mentor and colleague neuroradiologist Ajax George and I were awarded our first NIH-NIA funded studies of CT atrophy in dementia and in 1980, collaboration with Alfred Wolf and Joanna Fowler at BNL, NIH-NINDS funded FDG-PET studies of AD began. At the time, it was commonly believed that imaging had little to contribute to the AD diagnosis due to background aging effects. One real-world test of our AD diagnostic imaging work was to evaluate if our measurements differentiated between AD and hydrocephalus. We quantified CT scans for regional ventriculomegaly, evaluated compressed sulci and CSF pooling, we published and post mortem validated a CT scale for periventricular white matter pathology, and tested whether the hippocampus, a site of early AD pathology, was preserved in hydrocephalus. We ran FDG-PET scans before and after shunting looking for metabolic recovery, and collected biopsy samples during shunting for evidence for AD. This work led to another point of connection between my work and Roy Weller’s, interactions with two pathologists Henry Wisniewski and Robert Terry (both deceased) who both worked with Roy and who would become my valued friends and advisors. Today, the radiological diagnosis is an essential part of the differential dementia examination, and multiple avenues of imaging research, guided by Roy’s insights, continue. One such insight, and clearly for me, Roy’s most important contribution was for his anatomico-physiological studies examining the normal and pathological clearance of CSF and ISF from the brain. These studies, which continue today, are now led at the University of London in Southampton by Professor Roxana Carare, a former Weller mentee. Historically, these studies revealed the anatomical pathways for ISF drainage along basement membranes surrounding smooth muscle cells of cerebral arteries and along capillaries, and provided evidence that impaired interstitial flow contributed to parenchymal and vascular amyloid accumulations as well as being negatively impacted by amyloid accumulations. This mechanistic message was heard by many others, including the radiological community where currently PET and MRI imaging studies are underway today translating the Weller and Carare observations of a direct link between impaired vascular biology and AD and most recently other neurological diseases defined by misfolded proteinopathies. Thus, we wish Roy a happy birthday and applaud him and his colleagues for their continued efforts to treat dementia by providing pathology grounded data and testable hypotheses. Prof Margaret Esiri Consultant Neuropathologist, I first encountered Roy at my first BNS meeting in (probably) 1971 or 1972. He came over as a calm, confident deliverer of a presentation – I’ve forgotten what it was on. I think he may have been at Guy’s at the time. I was very impressed! I have gone on being impressed with Roy’s very significant contributions to neuropathology ever since. Long may they continue! Happy birthday, and many more to come, Roy! Prof Masafumi Ihara Head of the Cardiovascular Centre, It is my great pleasure to contribute to an article celebrating Prof. Weller's 80th birthday. Prof. Weller is an internationally recognized neuropathologist and well-known to have established the important concept of perivascular drainage pathway (now called IPAD) as an Abeta clearance system. I had been inspired by the concept and had a great opportunity to meet him in the XVIIth International Congress of Neuropathology in Salzburg (ICN 2010). I remember I had a good discussion with him in front of a poster of his team. I visited his and Prof. Carare’s laboratory in Southampton with three of my PhD students in 2012 and have been collaborating with the Southampton team. Our collaboration led to my investigator-led clinical trial of a vasoactive drug for MCI patients to determine whether IPAD can be facilitated clinically. Dr. Satoshi Saito, my former PhD student, joined the Southampton team in 2018, came back to Japan in 2020 after learning a lot not only from Prof. Carare but also from Prof. Weller, and is now working as a talented physician scientist in my department. Thus, Prof. Weller academically guided us as an established neuropathologist but not only that, he very kindly acted as a tour guide of Winchester for me a few years ago! Prof. Weller has continued impacting my research team for over 10 years with his plentiful neuropathological knowledge and we would like to send our heartfelt congratulations to Prof. Weller. Prof Raj Kalaria Neurovascular Pathologist, I had first heard about Roy from Helen Cserr, many moons ago! Besides the ‘art’ of neuropathology, Roy’s profound writings on drainage pathways of the brain intrigued me. In the late 1980s when I was still at Case Western Reserve University training in vascular neuropathology, I had communicated with Roy about a paper in Neuropathology and Applied Neurobiology. At the time, Roy was Editor-in-Chief of the journal. Few years later, I met Roy face-to-face when I was interviewed for a job in Southampton with the hope that the family and I could quickly return to England. I did not get the post but I thought it was such a privilege and an honour to meet the pleasant and humble Professor Weller! I had also thought somehow I should still keep in touch, especially that I developed a strong interest in cerebrovascular mechanisms and vascular pathology. I was absorbed in mechanisms of cerebral amyloid angiopathy (CAA) although at the time I searched for explanations on Cystatin C CAA, which causes profound intracerebral haemorrhages. Cystatin C is enriched in the brain and CSF but it was also found in the cervical lymph glands of Icelandic patients. Using the Cystatin C reasoning, I was determined to disprove the giants Selkoe and Wisniewski, who were both proposing at the time that cerebral Aβ amyloidosis was initiated by a protein(s) from the circulation (even papers in Nature) akin to the classical pathways discussed by Glenner and others how amyloidosis is caused in end organs. Large NIH funds were even spent on studies how Aβ could be transported from the blood-to-brain rather than searching for routes how it leaves the brain. All above was proven to be inaccurate and I was glad that Roy’s seminal work glued it altogether suggesting that Aβ is not only produced in the brain but ‘pouring’ out of it along perivascular pathways as one of the main routes. Roy and later Roxana beautifully demonstrated the mechanisms involved in CAA and how proteins including Aβ, prions, Cystatin C drain out formulating the IPAD hypothesis. This is also of importance because we have used the tonsils (lymphatic nodes) to test individuals who might have prions and infected with new variant CJD. To show, I understood the ‘drains’ of the brain, I was proud to give a talk on Weller’s Hypothesis of CAA at the ISN conference in Turin in 2004. Even though, I did not end up in Southampton, I am very fond of Roy and he has been an excellent mentor, advisor, collaborator and a good friend with whom one could relax, have a drink or two in the pub and discuss the ‘nuts and bolts’ of vascular neuropathology rather than daily mundane matters. Over the years, it has been one of the most exciting journeys with Roy. Our regular interactions at the BNS meetings, VasCog and ISN conferences including the one Roy organized in 2000 in Birmingham were refreshing, delightful and enjoyable. Having dinners at such gatherings and other times is something I always looked forward to and will cherish. Thank you Roy and congratulations on reaching 80, true to what the Scriptures say ‘The span of our life is 70 years or 80 if one is especially strong…’ (Psalms 90:10). Prof Dietmar Thal Consultant Neuropathologist, Roy Weller: A pioneering neuropathologist. The first time I heard a talk given by Roy Weller, he was explaining the contribution of perivascular clearance on several brain disorders. This was 1994. Perivascular clearance mechanisms became of clear importance for amyloid pathology in Alzheimer’s disease. Here, Prof. Weller had a strong impact on my thinking about how cerebral amyloid angiopathy develops in AD, namely as a result of perivascular clearance. For me, this could also explain interactions between cerebral small vessel disease and hypertension with AD by impairing the perivascular clearance. Prof. Weller’s concept of perivascular clearance is not only the basis of our understanding of cerebral amyloid angiopathy pathogenesis but had even a bigger impact on the understanding of fluid and protein drainage of the brain in general. Prof Hugh Perry Emeritus Professor, It was my pleasure to meet and get to know Roy Weller when I moved to Southampton in the late 1990s. Roy was a generous and welcoming colleague and as a basic scientist, mostly involved in pre-clinical models, he was there to remind us of the need to be aware of the human perspective. He had a great breadth of knowledge in neuropathology and also an understanding of the history behind many key observations in neuropathology. His research into how interstitial fluid carrying proteins from the brain drained from the brain was one of his passions. This is, of course, a very important component of understanding interactions between the immune system and the central nervous system. As the rapidly growing field of neuroimmunology advances so the research that Roy championed will remain relevant and new discoveries will amplify the importance of his favoured research topic. Prof Stephen Wharton Consultant Neuropathologist, I first came across Roy in the 1980s. I was presenting some (rather incomplete) results from my intercalated BSc project at a meeting of the Anatomical Society in Southampton. I received a kind and supportive question from an audience member and was told, “that’s Roy Weller”. Later, when I began training in neuropathology I used his textbook on Nervous System, Muscle and Eyes, part of the comprehensive Symmers series and enjoyed its clarity and approachability. Roy of course was editor of Neuropathology and Applied Neurobiology for ten years or so, and I had the opportunity to work with him more closely when I subsequently became Editor after Jim Lowe. Roy agreed to remain on the Editorial Board where he was always an enthusiastic contributor with good ideas to move the journal forward. He was also a great source of advice, both scientific and for those tricky situations that sometimes arise with papers. Since then I have continued to enjoy conversations about neuropathology at various meetings. I have always enjoyed these stimulating conversations and I, like many others, have appreciated his kindness and advice over many years.
Copyright: © 2021 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |