|
|
|
Free Neuropathology 2:19 (2021) |
|
Case Report |
|
Association of acute disseminated encephalomyelitis (ADem) and COVID-19 in a pediatric patient |
|
Liam Chen |
|
Department of Laboratory Medicine and Pathology, University of Minnesota Medical School, Minneapolis, MN, USA |
|
Corresponding author: |
|
Submitted: 8 June 2021 Accepted: 8 July 2021 Copyedited by: Deborah McIntyre Published: 12 July 2021 |
|
Keywords: SARS-CoV-2, COVID-19, Acute disseminated encephalomyelitis (ADem), Acute hemorrhagic leukoencephalitis (AHLE), Acute necrotizing encephalopathy of childhood (ANEC), Demyelinating |
|
Abstract Cases of acute disseminated encephalomyelitis (ADem) and its hyperacute form, acute hemorrhagic leukoencephalitis (AHLE), have been reported in coronavirus disease 2019 (COVID-19) patients as rare, but most severe neurological complications. However, histopathologic evaluations of ADem/AHLE pathology in COVID patients are extremely limited, so far having only been reported in a few adult autopsy cases. Here we compare the findings with an ADem-like pathology in a pediatric patient taken through a biopsy procedure. Understanding the neuropathology may shed informative light on the autoimmune process affecting COVID-19 patients and provide critical information to guide the clinical management.
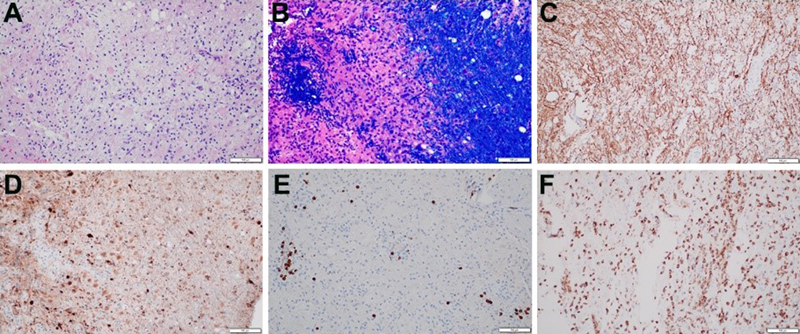
Numerous evidence has confirmed that coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) [1], affects the nervous system [2]. Most of the associated neurological dysfunctions are mild symptoms such as anosmia and dysgeusia [3] while severe debilitating neurological disorders such as stroke and meningoencephalitis are less frequent [4, 5]. These manifestations are likely caused by SARS-CoV-2 entering brain through direct infection of olfactory neuroepithelium [6], or transmitted by circulating lymphocytes and monocytes that are able to cross the blood-brain barrier [7]. Within the brain and spinal cord, various cell types including endothelial cells, vascular pericytes and smooth muscle, neurons and glia all express angiotensin converting enzyme 2 (ACE2) receptor [8, 9], the primary receptor for SARS-CoV-2 spike protein [10]. It is true that SARS-CoV-2 could be detected in olfactory epithelium [11], brain and cranial nerves by RT-PCR [12, 13], immunohistochemistry (IHC) [14], in situ hybridization (ISH) [11] and electron microscopy [15]. In addition, neuropathological findings such as leptomeningeal and parenchymal lymphocytic inflammation, microglial nodules and neuronophagy are compatible with a diagnosis of viral meningoencephalitis [12, 16]. Nevertheless, neither viral inclusions nor cytopathic changes have been observed on hematoxylin and eosin (H&E) stained slides. Furthermore, in the few studies that have reported evidence of viral RNA or protein in the cranial nerves or brainstem, the degree and distribution of neuropathologic changes have shown no correlation with the amount of virus in a given area of pathology, suggesting that the pathology is rather secondary to the systemic effects of viral infection. Indeed, convincing evidence has elucidated that systemic hypercoagulability plays an important role in COVID-19 related stroke process, as SARS-CoV-2 could induce cytokine storm and endotheliopathy [17, 18], which in turn lead to the histologic findings of microthrombi, hemorrhages and infarcts [19, 20]. In contrast, there is still considerable debate over whether parainfectious, autoimmune mediated process such as acute disseminated encephalomyelitis (ADem), or its hyperacute form, acute hemorrhagic leukoencephalopathy (AHLE), can truly be attributed to COVID-19. One reason for this controversy is the lack of neuropathological descriptions of ADem and AHLE despite that a handful clinical and imaging case studies of COVID-19 patients have suggested lesions characteristic of ADem or AHLE [21-31]. So far, there are only few case reports with neuropathological features of ADem and AHLE in adult patients who died from complications of COVID-19 [32-34]. Another reason for the controversy, as will be discussed further below, is whether the observed ADem- or AHLE-like pathology is truly due to a primary demyelinating process or merely a secondary white matter injury of a comorbid vascular disease or a combination. R. Ross Reichard et al. reported the neuropathological findings of a 71-year-old patient who died from complications of COVID-19 [32]. Hemorrhagic white matter lesions were present throughout the cerebral hemispheres. Luxol fast blue/ periodic acid–Schiff (LFB/PAS) identified loss of myelin, PAS-positive macrophages, and fragmented axonal processes within these lesions. It has features of AHLE, although necrotic blood vessels and perivascular inflammation were not identified within the hemorrhagic lesions. A second distinct pathology identified was characterized by small subcortical white matter pallor with a variable perivenular distribution, resembling an ADem-like histological appearance. Notably, prominent acute axonal injury was present in the regions of myelin loss, which is not characteristic of classic ADem [32]. Jamie M. Walker et al. presented two cases of fatal COVID-19 with severe neurologic sequalae [33]. One was a 51-year-old woman with an irregular pattern of demyelination centered primarily around veins and venules. Both perivascular CD3+ T-lymphocytes as well as frequent perivascular and parenchymal CD68+ histiocytes and activated microglial cells were present, consistent with a diagnosis of ADem. Another autopsy examination of a 64-year-old demonstrated myelin pallor, perivascular CD3+ T-lymphocytes, axonal spheroids, as well as numerous ring- and ball-hemorrhages throughout the white matter with central blood vessels showing fibrinoid necrosis, most consistent with a diagnosis of AHLE. It should be noted that in all three aforementioned cases, global hypoxic-ischemic injury was present, in addition to microscopic cortical infarcts in the first case [32] and large areas of cerebral intraparenchymal hemorrhages in the third case [33]. Thus, the neuropathological lesions should be interpreted with caution and the possibility of a cerebrovascular origin with secondary demyelinating pathology should be considered. ADem and AHLE usually affects children and young adults after an infection or vaccination [35]. However there are very few reported cases of ADem in pediatric population with SARS-CoV-2 infection based on clinical features and MRI findings [25, 36, 37]. This is consistent with the differing clinical presentations of COVID-19 in children and adult patients. Recently, we have examined a brain biopsy taken from an 8-year-old girl who was admitted with new-onset seizures. On hospital day 2, COVID-19 spike IgG antibody testing was positive. Brain MRI demonstrated extensive T2 hyperintensity centered at bilateral basal ganglia, extending to the frontal white matter, external and internal capsules, corpus callosum, thalami, insula, as well as the cerebellar hemispheres, brainstem and the spinal cord. Interval MRI imaging demonstrated persistent diffusion restriction in the affected white matter throughout much of the central white matter tracts, cerebral peduncles, corticospinal tracts and cerebellar white matter, suggesting ongoing demyelination, but no evidence to suggest hemorrhages. Three weeks later, there was vacuolating necrosis in bilateral basal ganglia. Ventriculoperitoneal shunt placement and stereotactic brain biopsy were performed on hospital day 48. Neuropathological examination of the brain biopsy tissue revealed subcortical white matter pallor with perivascular lymphocytic infiltrates centered primarily around venules (Figure 1A). Immunohistochemical staining for SARS-CoV-2 spike protein was negative. No microglial nodules or evidence of neuronophagia was present. Demyelination was confirmed by LFB stain (Figure 1B) whereas axons were relatively preserved as shown by neurofilament immunostain (Figure 1C). Interestingly, APP immunostain highlighted damaged, swollen axons in areas surrounding the vessels, a pattern seen in adult patient as well (Figure 1D). The lymphocytes were composed predominantly of CD3-positive T cells (Figure 1E) whereas CD68 stain highlighted numerous perivascular macrophages and the diffuse distribution of activated microglia (Figure 1F).
Figure 1. Neuropathological findings of a brain biopsy from a child post SARS-CoV-2 infection. A. H&E section of white matter pallor, reactive astrogliosis and perivascular lymphocytic infiltrates around small veins and venules. B. LFB stain demonstrates the perivascular myelin loss within the subcortical white matter lesion. C. Neurofilament immunostain shows preservation of most axons in the region of myelin loss. D. APP immunostain identifies axonal swellings adjacent to the perivascular areas. E. Perivascular lymphocytes are predominantly CD3-positive T cell. F. CD68 immunostain confirms both perivascular and diffuse distributions of macrophages within the area of white matter pallor. Scale bar, 100 μm in A-E. In this case, the absence of confounding concomitant cerebrovascular lesions makes the pathological interpretation relatively straightforward. These ADem/AHLE cases represent rare, but the most severe end of the COVID-19 neuropathologic spectrum. Consequently, ADem/AHLE should be a consideration during evaluation of patients, especially children with encephalopathy, seizures and/or focal neurologic deficits after recovering from COVID-19. Another intriguing development in this pediatric patient is the later MRI findings of bilateral basal ganglia necrosis, suggestive an even rarer entity, acute necrotizing encephalopathy (ANE), also referred as acute necrotizing encephalopathy of childhood. ANE is characterized by multiple, symmetrical lesions in the thalami, striatum, cerebral white matter, and brain stem [38]. Despite its association with viral infection, ANE is not considered an inflammatory encephalitis in comparison to ADem and AHLE. In fact, it has been suggested that an intense surge of cytokines causes damage to the blood-brain barrier with necrosis as a secondary effect [39]. Given SARS-CoV-2 is a cytokine storm trigger, it is not surprising to observe ANE as a probable association of COVID-19 [40, 41]. It would be important to understand whether these parainfectious demyelinating diseases reflect distinct pathological processes or a continuum of a single disease. References 1. Zhu, N., et al., A Novel Coronavirus from Patients with Pneumonia in China, 2019. N Engl J Med, 2020. 382(8): p. 727-733. 2. Lou, J.J., et al., Neuropathology of COVID-19 (neuro-COVID): clinicopathological update. Free Neuropathol, 2021. 2. 3. Lechien, J.R., et al., Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Eur Arch Otorhinolaryngol, 2020. 277(8): p. 2251-2261. 4. Merkler, A.E., et al., Risk of Ischemic Stroke in Patients With Coronavirus Disease 2019 (COVID-19) vs Patients With Influenza. JAMA Neurol, 2020. 5. Dogra, S., et al., Hemorrhagic stroke and anticoagulation in COVID-19. J Stroke Cerebrovasc Dis, 2020. 29(8): p. 104984. 6. Fodoulian, L., et al., SARS-CoV-2 Receptors and Entry Genes Are Expressed in the Human Olfactory Neuroepithelium and Brain. iScience, 2020. 23(12): p. 101839. 7. Salamanna, F., et al., Body Localization of ACE-2: On the Trail of the Keyhole of SARS-CoV-2. Front Med (Lausanne), 2020. 7: p. 594495. 8. Brann, D.H., et al., Non-neuronal expression of SARS-CoV-2 entry genes in the olfactory system suggests mechanisms underlying COVID-19-associated anosmia. Sci Adv, 2020. 6(31). 9. Xia, H. and E. Lazartigues, Angiotensin-converting enzyme 2 in the brain: properties and future directions. J Neurochem, 2008. 107(6): p. 1482-1494. 10. Gheblawi, M., et al., Angiotensin-Converting Enzyme 2: SARS-CoV-2 Receptor and Regulator of the Renin-Angiotensin System: Celebrating the 20th Anniversary of the Discovery of ACE2. Circ Res, 2020. 126(10): p. 1456-1474. 11. Meinhardt, J., et al., Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat Neurosci, 2021. 24(2): p. 168-175. 12. Matschke, J., et al., Neuropathology of patients with COVID-19 in Germany: a post-mortem case series. Lancet Neurol, 2020. 19(11): p. 919-929. 13. von Weyhern, C.H., et al., Early evidence of pronounced brain involvement in fatal COVID-19 outcomes. Lancet, 2020. 395(10241): p. e109. 14. Solomon, I.H., et al., Neuropathological Features of Covid-19. N Engl J Med, 2020. 383(10): p. 989-992. 15. Morbini, P., et al., Ultrastructural Evidence of Direct Viral Damage to the Olfactory Complex in Patients Testing Positive for SARS-CoV-2. JAMA Otolaryngol Head Neck Surg, 2020. 146(10): p. 972-973. 16. Al-Dalahmah, O., et al., Neuronophagia and microglial nodules in a SARS-CoV-2 patient with cerebellar hemorrhage. Acta Neuropathol Commun, 2020. 8(147). 17. Song, P., et al., Cytokine storm induced by SARS-CoV-2. Clin Chim Acta, 2020. 509: p. 280-287. 18. Goshua, G., et al., Endotheliopathy in COVID-19-associated coagulopathy: evidence from a single-centre, cross-sectional study. Lancet Haematol, 2020. 7(8): p. e575-e582. 19. Fabbri, V.P., et al., Brain ischemic injury in COVID-19-infected patients: a series of 10 post-mortem cases. Brain Pathol, 2021. 31(1): p. 205-210. 20. Hernandez-Fernandez, F., et al., Cerebrovascular disease in patients with COVID-19: neuroimaging, histological and clinical description. Brain, 2020. 143(10): p. 3089-3103. 21. Parsons, T., et al., COVID-19-associated acute disseminated encephalomyelitis (ADem). J Neurol, 2020. 267(10): p. 2799-2802. 22. Novi, G., et al., Acute disseminated encephalomyelitis after SARS-CoV-2 infection. Neurol Neuroimmunol Neuroinflamm, 2020. 7(5). 23. Abdi, S., A. Ghorbani, and F. Fatehi, The association of SARS-CoV-2 infection and acute disseminated encephalomyelitis without prominent clinical pulmonary symptoms. J Neurol Sci, 2020. 416: p. 117001. 24. Sawlani, V., et al., COVID-19-related intracranial imaging findings: a large single-centre experience. Clin Radiol, 2021. 76(2): p. 108-116. 25. de Miranda Henriques-Souza, A.M., et al., Acute disseminated encephalomyelitis in a COVID-19 pediatric patient. Neuroradiology, 2021. 63(1): p. 141-145. 26. Yong, M.H., et al., A Rare Case of Acute Hemorrhagic Leukoencephalitis in a COVID-19 Patient. J Neurol Sci, 2020. 416: p. 117035. 27. Umapathi, T., et al., Encephalopathy in COVID-19 patients; viral, parainfectious, or both? eNeurologicalSci, 2020. 21: p. 100275. 28. McCuddy, M., et al., Acute Demyelinating Encephalomyelitis (ADem) in COVID-19 Infection: A Case Series. Neurol India, 2020. 68(5): p. 1192-1195. 29. Lopes, C.C.B., et al., Acute Disseminated Encephalomyelitis in COVID-19: presentation of two cases and review of the literature. Arq Neuropsiquiatr, 2020. 78(12): p. 805-810. 30. Langley, L., et al., Acute disseminated encephalomyelitis (ADem) associated with COVID-19. BMJ Case Rep, 2020. 13(12). 31. Handa, R., et al., Covid-19-associated acute haemorrhagic leukoencephalomyelitis. Neurol Sci, 2020. 41(11): p. 3023-3026. 32. Reichard, R.R., et al., Neuropathology of COVID-19: a spectrum of vascular and acute disseminated encephalomyelitis (ADem)-like pathology. Acta Neuropathol, 2020. 140(1): p. 1-6. 33. Walker, J.M., et al., COVID-19 Patients With CNS Complications and Neuropathologic Features of Acute Disseminated Encephalomyelitis and Acute Hemorrhagic Leukoencephalopathy. J Neuropathol Exp Neurol, 2021. 34. Bryce, C., et al., Pathophysiology of SARS-CoV-2: the Mount Sinai COVID-19 autopsy experience. Mod Pathol, 2021. 35. Cole, J., et al., Acute Disseminated Encephalomyelitis in Children: An Updated Review Based on Current Diagnostic Criteria. Pediatr Neurol, 2019. 100: p. 26-34. 36. McLendon, L.A., et al., Post-COVID-19 Acute Disseminated Encephalomyelitis in a 17-Month-Old. Pediatrics, 2021. 147(6). 37. Vraka, K., et al., Two Paediatric Patients with Encephalopathy and Concurrent COVID-19 Infection: Two Sides of the Same Coin? Case Rep Neurol Med, 2021. 2021: p. 6658000. 38. Wong, A.M., et al., Acute necrotizing encephalopathy of childhood: correlation of MR findings and clinical outcome. AJNR Am J Neuroradiol, 2006. 27(9): p. 1919-23. 39. Mizuguchi, M., Acute necrotizing encephalopathy of childhood: a novel form of acute encephalopathy prevalent in Japan and Taiwan. Brain Dev, 1997. 19(2): p. 81-92. 40. Lazarte-Rantes, C., et al., Acute Necrotizing Encephalopathy Associated With SARS-CoV-2 Exposure in a Pediatric Patient. Cureus, 2021. 13(5): p. e15018. 41. Kumar, N., et al., Acute Necrotizing Encephalitis as a Probable Association of COVID-19. Indian J Crit Care Med, 2020. 24(10): p. 991-994.
Copyright: © 2021 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |