|
|
|
Free Neuropathology 2:11 (2021) |
|
Flashback |
|
Taylor’s focal cortical dysplasia revisited: History, original specimens and impact |
|
Burkhard S. Kasper |
|
Epilepsy Center, Department of Neurology, Friedrich-Alexander University Erlangen-Nuremberg, Germany |
|
Corresponding author: |
|
Submitted: 01 April 2021 Accepted: 18 April 2021 Copyedited by: Jerry Lou Published: 23 April 2021 |
|
Additional resources and electronic supplementary material: supplementary material |
|
Keywords: Dysplasia, Epilepsy, History, Taylor, FCD |
|
Original paper: |
|
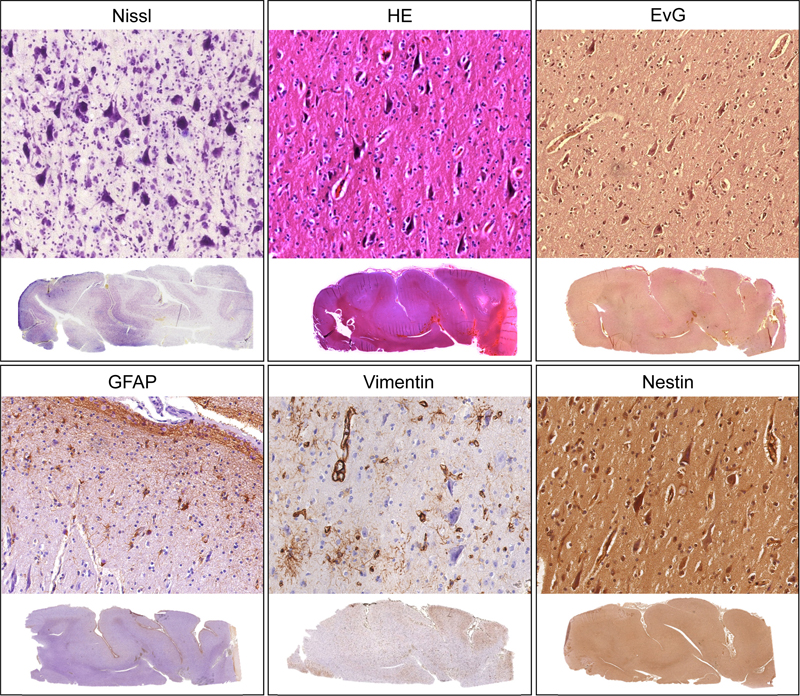
Abstract 50 years ago back in 1971, David C. Taylor and colleagues from England reported on a small series of surgical epilepsy cases proposing a new type of tissue lesion as a cause of difficult-to-treat focal epilepsy: a localized malformation of cerebral cortex. The lesion is now known as focal cortical dysplasia (FCD) Type II or Taylor’s cortical dysplasia. FCD II is not rare, and today is a frequent finding in neurosurgical epilepsy specimens. Medical progress has been achieved in that the majority of FCD II is diagnosed non-invasively by magnetic resonance imaging today. Detailed studies on FCD revealed that the lesion belongs to a spectrum of mTOR-o-pathies, thereby confirming the authors´ initial hypothesis of a relationship to tuberous sclerosis. Here, selected original materials from Taylor´s series are presented as virtual slides, supplemented by original clinical records, in order to give a first-hand impression of this milestone finding in neuropathology of epilepsy. What exactly did the authors report in this study? Tissue findings from surgical brain specimens from 10 epilepsy patients were presented in detail [1], illustrating intriguing but formerly un-appreciated abnormalities of neocortical architecture. As core findings, neurons of bizarre size and shape were described throughout cortical layers II-VI (today known as dysmorphic neurons) causing laminar disruption, in most cases accompanied by another pathological cell type, named grotesque cells of probable glial origin (today known as balloon cells). Disorganization of cortical architecture and these cellular components were defined as pathognomonic features and suggested a new type of malformative CNS lesion, i.e. focal dysplasia, today known as focal cortical dysplasia (FCD) type II or Taylor’s dysplasia [2]. Why is this a milestone paper? The authors’ synopsis was groundbreaking since it defined a new category of circumscript lesion responsible for intractable focal epilepsy, adding to the spectrum of better-known epileptogenic lesions such as hippocampal sclerosis and benign neoplasms. Epilepsy surgery was a rather young discipline back then. Most causal epileptogenic lesions could be detected ex-post by histopathology only, since other supporting diagnostic modalities were unavailable at the time. DC Taylor, a psychiatrist (!), recognized the similarities between these few cases out of several hundreds of cases just by reading through the reports, un-aided by any data such as imaging techniques [3]. These lesions were largely invisible to naked eye macroscopic examination in the operating theater or during tissue preparation [1]. By now, FCD has become a classic cause of epilepsy, ranking among the top 3 structural causes in epilepsy surgical series and in the majority is detected pre-surgically by magnetic resonance imaging (MRI) [2, 4] What had been known before this seminal contribution? The authors in 1971 stated that “no reports of closely similar observations had been traced thus far” [1]. Findings with some similarity to focal dysplasia had been sporadically reported under different names, such as “abortive tuberous sclerosis” [5], “infantile cerebral gliosis with giant nerve cells” [6] or “localized cerebral gliosis with giant neurons” [7]. Maybe the earliest reference to a dysplasia-like pathology from epilepsy brains goes back to 1896 [8], but reports were overall scarce before the era of epilepsy surgery. Which of the authors central hypotheses or conclusions turned out right or wrong? The histological reminiscence to tuberous sclerosis (TS) was noted and pointed out [1]. Corsellis extensively searched for hints towards TS in both the patients and their families (see supplements 2-6). In a preceding conference presentation, the term “cryptic tuber” had already been used [9]. However, absence of any other signs of TS or suspicious familial traits was emphasized [1]. Meanwhile, FCD II has been identified as closely relating to genetic alterations within the mTOR-signalling-cascade and belonging to the spectrum of “mTOR-o-pathies” together with tuberous sclerosis and other malformations [10, 11]. FCD was correctly proposed to be a solitary lesion in most cases, its removal likely predicting seizure improvement or freedom. The authors proposed that dysplasia of their type would directly underlie the electrical and clinical manifestations of certain epilepsies. This has been strikingly verified later, since FCD turned out as intrinsically epileptogenic, i.e. the dysmorphic neurons themselves show the abnormal firing behavior, as proven by many techniques today such as in-vivo invasive recordings, electrocorticography, non-invasive measurements and in-vitro cellular recordings in FCD (for reference, see [4]). While Taylor and the group did not comment on the presumed frequency of FCD, it is remarkable, that they found their 10 cases in a cohort of 300 epilepsy surgeries corresponding to 3%, while nowadays FCD ranks among the top pathologies in surgical series [2], see also below. At what stage of the authors´ career was the paper published? Three out of four authors were well-known authorities in their fields, since Murray Falconer had established his fine epilepsy surgical series at the Maudsley cooperating with the experienced neuropathology service at Runwell, provided by J.A.N Corsellis and Clive Joseph Bruton. David Taylor had been a research fellow at the beginning of his thirties and had started researching the psychiatric aspects of epilepsy surgery at the Maudsley, giving rise to several publications from 1967 on (see also a letter by him in suppl. 7). After recognizing the commonalities in the tissue reports, he and the co-authors meticulously collected all available data leading to this seminal paper. How was the paper received over the time? More than 800 citations have cumulated since publication up to 2020 with about 20 citations per decade in the Seventies and Eighties and >200 citations per decade since then, 75% citations from clinical neurology [12]. The paper was translated early, e.g. to German, French and Russian abstracts [13] and was widely recognized. “Taylor’s dysplasia” as a term was coined by Montreal epileptologist Fred Andermann (personal communication, see [3]). It was discussed later that the microscopic features were not strictly unique to Taylor’s dysplasia, but may be seen in cases of hemimegalencephaly, for example [14]. Dysplasia still was estimated to account for a minority of 2-5% of epilepsy surgery specimens as late as 1992 [14], while numbers have raised in modern series up to 30% [2], which relates to largely improved imaging and recording techniques. What happened to the original histological slides until today? Starting early after 1950 J.A.N. Corsellis built a large collection of brain specimen recruited from his neuropathology service including both surgical and autopsy tissues [15]. This collection came to be known as the Corsellis Collection later on [3]. It was the first of its kind and located in Runwell Hospital/Wickford Essex for years [15,16], and later moved to London (held by the West London Mental Health NHS Trust), after Runwell Hospital closed down. Of note, Corsellis in addition to meticulously performing macro- and microinvestigations documented in great detail the clinical patient findings and obtained many clinical notes (see supplemental material). His activities were funded by the Medical Research Council as early as 1953 [16], he became a reference pathologist consulted by international colleagues [16], and after his death in 1994 his activities were continued by Clive Bruton. The original slides of focal dysplasia remained undiscovered as part of the Corsellis Collection brain bank in London for decades. An incomplete but significant part of slides, paraffin blocks and accompanying material including microphotographs and patient notes were found there and saved during research on the life and work of J.A.N. Corsellis [3] and given to BS Kasper by the Corsellis Collection to act as official custodian of this material when it became clear that the Collection would be dismantled. Did the re-discovery of this material elicit any surprising insights? Vast material accompanying the tissue specimen impressively illustrates the working strategy at the institution led by Corsellis. Clinical notes and findings not only were systematically searched for, collected and saved (see suppl. 1-6), but also valued and integrated into the reports and discussions. There was a close exchange between the pathology group and the clinicians involved, not only the active neurosurgeons, but also the hospital and external neurologists, doctors and caregivers of the patients, as well as possible. This included postoperative years also. Corsellis insisted on postsurgical cognitive tests, for example, and with Taylor even visited the patient at home. No challenge seemed too difficult to overcome for the sake of obtaining further important information, as exemplified by correspondence between Corsellis and neuropathologist Professor H. Orthner from Göttingen/Germany (see suppl. 4) which showed the length to which Corsellis labored to obtain details about this patients mother who had died and had autopsy (see suppl. 6) as well as about the patients son, in order to check for any manifestations of tuberous sclerosis. What can be seen on the original slides? We present case 2 from the Taylor paper for this re-appreciation. Original slides in various stains were found preserved (HE, Van Gieson, Bielschowsky, PTAH, Nissl, Oil-Red, Marchi). These slides correspond to Figure 6 from the 1971 paper (for orientation see original figure and compare to macro-photographs and drawings in suppl. 1). Exploring the original slides in H&E and Nissl stains as well as new stainings obtained from the original paraffin blocks (see figure) nicely illustrates the presence of dysmorphic giant neurons, especially found at the bottom part of a sulcus. You are invited to explore the interactive, virtual microscopy slides in detail, just as Taylor and Corsellis did back then. This lesion nowadays would be classified as focal cortical dysplasia Type IIA, since balloon cells (then described as grotesque cells of probable glial origin) were not found, as confirmed by review. However, the majority of specimens in Taylor´s series did contain balloon cells, i.e. focal cortical dysplasia Type IIB, representing the most common correlate of “FCD” or “Taylor type dysplasia” as defined by imaging today. Remember that in 1971 no magnetic resonance imaging (MRI) was available.
Figure 1. Original (historical) slides from Taylors series (Nissl, HE) and new slides cut from the original paraffin blocks (EvG, GFAP, vimentin, nestin). Clicking into the respective picture will lead you to the full virtual slide. Links to the slides: Nissl: https://omero-imaging.uni-muenster.de/webclient/img_detail/34739 HE: https://omero-imaging.uni-muenster.de/webclient/img_detail/34169 EvG: https://omero-imaging.uni-muenster.de/webclient/img_detail/34358 GFAP: https://omero-imaging.uni-muenster.de/webclient/img_detail/34360 Vimentin: https://omero-imaging.uni-muenster.de/webclient/img_detail/34363 Nestin: https://omero-imaging.uni-muenster.de/webclient/img_detail/35885 Supplementary material Supplements 1-6 as well as their content appear in chronological order. To follow, click on the links. Free full text - Taylor 1971: https://dx.doi.org/10.1136/jnnp.34.4.369 Suppl. 1: Tissue workup incl. notes, macro- and microphotographs by J.A.N. Corsellis Suppl. 3: Documentation relating to Corsellis’ inquiries for clinical data and early follow up Suppl. 4: Correspondence with Prof. Orthner, Göttingen, Germany Suppl. 5: Documents illustrating the patient’s long term follow up Suppl. 6: Medical history of the patient´s mother Suppl. 7: A personal letter from David C. Taylor The notes and records presented here accompanied the preserved patient’s material, as collected, stored and delivered by the Corsellis Collection. The full original material (photos & notes) were digitized in high quality to jpg-format at Erlangen University. Information enabling for identification of the patient or her mother was eliminated by image editing using ACDsee Pro7 software (BSK). Acknowledgement This contribution, 50 years after the original publication in JNNP, is dedicated to the memory of Professor David C. Taylor (1933-2021) [19] and Professor J.A.N. Corsellis (1915-1994) [17,18,3], two great men of neuroscience, who were the right people at the right place in the right time back then. Thanks to Dr. Thomas Zobel from the WWU Imaging Network for support and hosting the OMERO image server. Thanks to Christian Thomas, Münster, for producing the virtual slides. Thanks to Frank Bittner, Erlangen, for excellent digitizing service and to Thomas Sebille (fotomas) for help with image editing. References 1. Taylor DC, Falconer MA, Bruton CJ, Corsellis JAN. Focal dysplasia of the cerebral cortex in epilepsy. Journal of Neurology, Neurosurgery and Psychiatry 1971; 34: 369-387. 2. Blümcke I, Thom M, Aronica E, Armstrong DD, Vinters HV, Palmini A, Jacques TS, Avanzini G, Barkovich AJ, Battaglia G, Becker A, Cepeda C, Cendes F, Colombo N, Crino P, Cross JH, Delalande O, Dubeau F, Duncan J, Guerrini R, Kahane P, Mathern G, Najm I, Ozkara C, Raybaud C, Represa A, Roper SN, Salamon N, Schulze-Bonhage A, Tassi L, Vezzani A, Spreafico R. The clinicopathologic spectrum of focal cortical dysplasias: a consensus classification proposed by an ad hoc Task Force of the ILAE Diagnostic Methods Commission. Epilepsia 2011; 52: 158-174. 3. Kasper BS, Taylor DC, Janz D, Kasper EM, Maier M, Williams MR, Crow TJ. Neuropathology of epilepsy and psychosis: the contributions of J.A.N. Corsellis. Brain. 2010;133: 3795-3805. 4. Kasper BS, Rössler K, Hamer HM, Dörfler A, Blümcke I, Coras R, Roesch J, Mennecke A, Wellmer J, Sommer B, Lorber B, Lang JD, Graf W, Stefan H, Schwab S, Buchfelder M, Rampp S. Coregistrating magnetic source and magnetic resonance imaging for epilepsy surgery in focal cortical dysplasia. Neuroimage Clin. 2018;19: 487-496. 5. Yakovlev PI. Congenital morphologic abnormalities of the brain in a case of abortive tuberous sclerosis. Arch Neurol Psychiat (Chic) 1939; 41: 119-139. 6. Crome L. Infantile cerebral gliosis with giant nerve cells. Journal of Neurology, Neurosurgery and Psychiatry 1957; 20: 117-124. 7. Cravioto H, Feigin I. Localized vertebral gliosis with giant neurons histologically resembling tuberous sclerosis. J Neuropathol Exp Neurol 1960; 19: 572-579. 8. Roncoroni L. La fine morfologia del cervello degli epilettici e dei delinquenti. Arch Psich Scienze Penali Antropol Criminale 1896; 17: 92-116. 9. Corsellis JAN. “Cryptic Tubers” as a cause of focal epilepsy. Proceedings of the Society of British Neurosurgeons (Abstract) Journal of Neurology, Neurosurgery and Psychiatry 1971; 34: 104-105. 10. D'Gama AM, Woodworth MB, Hossain AA, Bizzotto S, Hatem NE, LaCoursiere CM, Najm I, Ying Z, Yang E, Barkovich AJ, Kwiatkowski DJ, Vinters HV, Madsen JR, Mathern GW, Blümcke I, Poduri A, Walsh CA.Somatic Mutations Activating the mTOR Pathway in Dorsal Telencephalic Progenitors Cause a Continuum of Cortical Dysplasias. Cell Rep. 2017;21: 3754-3766. 11. Baldassari S, Ribierre T, Marsan E, Adle-Biassette H, Ferrand-Sorbets S, Bulteau C, Dorison N, Fohlen M, Polivka M, Weckhuysen S, Dorfmüller G, Chipaux M, Baulac S. Dissecting the genetic basis of focal cortical dysplasia: a large cohort study. Acta Neuropathol. 2019;138(6):885-900. 12. https://apps.webofknowledge.com (searched Aug 13 2020). 13. Corsellis JAN, Bruton CJ, Taylor DC, Falconer MA. Lokalisierte Dysplasie der Hirnrinde auf Grund von Gewebeuntersuchungen, die durch neurochirurgische Eingriffe bei Epileptikern gewonnen wurden. Psychiatr. Neurl. Med. Psychol (Leipz) 1973; 17-18: 43-53. 14. Janota I, Polkey CE. Cortical dysplasia in epilepsy - a study on material from surgical resections for intractable epilepsy. Recent advances in epilepsy 1992; 5: 37-49. 15. Schoefert, Anna Kathryn. Research on the human brain post mortem in Britain, c.1950-1980: constituting the Corsellis Collection. M Phil thesis, Cambridge University, 2011. 16. Metters JS. Isaacs report. TSO, May 2003; Page 235-239 17. Janota I. Obituary J.A.N Corsellis (1915-1994). Neuropathology Appl Neurobiol 1995; 21: 168. 18. Crow TJ. Obituary J.A.N Corsellis (1915-1994). Psychiatric Bulletin 1996; 20: 508-509. 19. Kasper BS. In memoriam: David C. Taylor. Epilepsy Behav 2021 Apr 15; 118:107960
Copyright: © 2021 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |