|
|
|
Free Neuropathology 2:12 (2021) |
|
Flashback |
|
Charcot identifies and illustrates amyotrophic lateral sclerosis |
|
Charles Duyckaerts1,2, Thierry Maisonobe1,3, Jean-Jacques Hauw4, Danielle Seilhean1,5 |
|
1 Raymond Escourolle Neuropathology Department, La Salpêtrière Hospital, Assistance Publique des Hôpitaux de Paris, Sorbonne Université, Paris, France |
|
Corresponding author: |
|
Submitted: 31 March 2021 Accepted: 08 May 2021 Copyedited by: Lauren Walker and Henry Robbert Published: 18 May 2021 |
|
Keywords: Amyotrophic lateral sclerosis, Charcot, History of medicine, Pyramidal tract |
|
Abstract Jean-Martin Charcot described what he called amyotrophic lateral sclerosis in his 12th and 13th lessons published in 1873 by Bourneville. He distinguished the symptoms that were related to the lesion of the anterior horn of the spinal cord and those that were due to the degeneration (that he named “sclerosis”) of its lateral column. He thought that “inflammation” progressed from the lateral column to the anterior horn (but the term inflammation is not to be taken in the current meaning): the lesion of the anterior horn was thus “deuteropathic”. An album containing drawings made by Charcot is kept in La Salpêtrière Neuropathology Department. Four drawings are pasted on one of its pages, showing the degeneration of the pyramidal tract. They constitute the original of the engravings illustrating Charcot’s 12th lesson. The illustration of the fascicular atrophy of the adductor pollicis presented in the album does not appear in the lessons, even though this alteration is widely discussed and linked to the lesion of the anterior horn, which was supposed to ensure the “nutrition” of the muscle. The technique used by Charcot and his interpretation of the microscopic pictures, as exposed in his lessons, are discussed. Introduction Jean-Martin Charcot identified amyotrophic lateral sclerosis (ALS) on clinical-pathological grounds. The data, which he collected, and his conception are remarkably summarized in the second volume of his Lessons on the diseases of the nervous system, edited by Bourneville (Charcot, 1873) and in his Lessons on cerebral localization, edited by Bourneville et Brissaud (Charcot, 1876). The Neuropathology Laboratory of La Salpêtrière Hospital keeps an album containing original drawings by Charcot. One of its pages concerns an ALS case. This paper compares the two documents: the drawings and the description of the disease, both by Charcot. The album The album bears the title “Charcot Museum, Pathological anatomy”, handwritten in ink on the black hardcover (Fig. 1). It contains 100 light-blue pages of a format known as “Couronne” in France (37 x 47 cm), commonly used by the artists of the time. Pages 15 to 100 are blank. They were numbered with stencils. “Foxing” (i.e. brown spots and browning of the edges) suggests they are original. The first fourteen pages have been restored, as well as the binding, some twenty years ago, and were renumbered in pencil. The drawings, usually on white papers, are pasted on those pages. There are also a few engravings, some taken from Charcot’s articles. All the drawings have the same style and, although not signed, are reputed to be by Charcot himself. Charcot had hesitated between medicine and the fine arts. He left numerous drawings of pathological anatomy and sketches of patients (see for instance, the case Bachère, Charcot, 1892, fig. 64, p 337, https://gallica.bnf.fr/ark:/12148/bpt6k55646784/f343.item.texteImage; or a case of Parkinson’s disease ibidem, fig. 63, p 336; the illustration of “a labioglossal spasm”, Charcot, 1892, fig. 19 and 20, p 211, https://gallica.bnf.fr/ark:/12148/bpt6k55646784/f217.image.r=fig; or the picture of the face in a case of Parkinson’s disease, Charcot, 1892, fig. 60, p 334, https://gallica.bnf.fr/ark:/12148/bpt6k55646784/f340.image.r=fig).
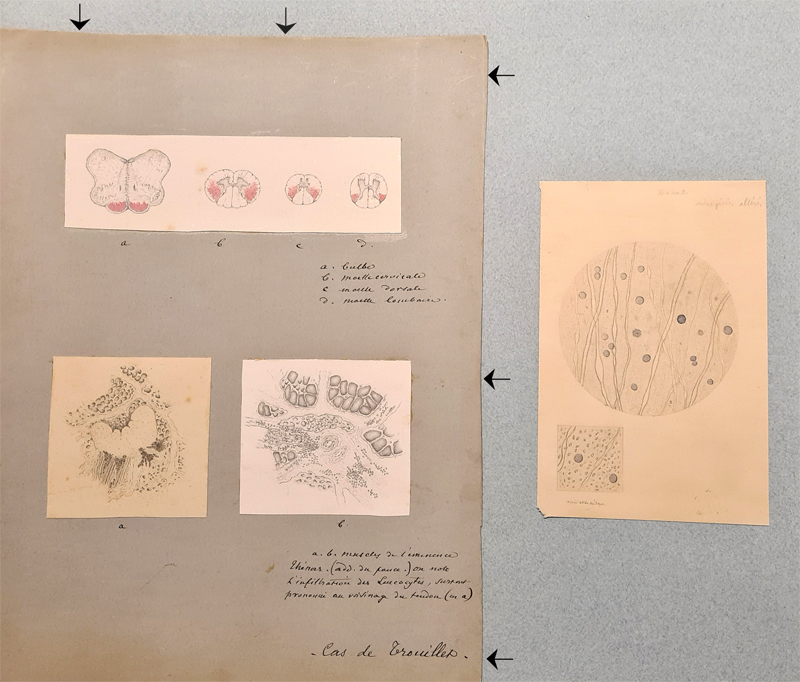
Fig. 1. Hardcover of the album in which Charcot’s drawings were collected. These drawings demonstrate his talent for illustrating the cases that he examined. The style of the drawings found in the album is identical to that of the drawings found in the notes that he prepared for his “lessons” (still visible at Charcot library, now located at Paris Brain Institute-ICM, https://institutducerveau-icm.org/en/actualite/charcot-library): there is no reason to question their authorship. The drawings, initially made on loose sheets, were secondarily collected and pasted in the album that was passed down from Charcot’s own laboratory to the current department of neuropathology. Each page generally concerns a particular topic (Microaneurysm, multiple sclerosis, myelitis, lateral funiculus in a foetus, syringomyelia, Pott’s disease, vertebral metastases, anatomy of the posterior funiculi, lead paralysis, tumor of the spinal cord, ALS, cysticercosis). The album has never been the subject of a specific study, although some of its pictures have been published occasionally (the drawing of the central nervous system of the ALS case under investigation here has been published in Seilhean, 2020). Cases and samples Three original drawings of the ALS case, p 12 of the album (Fig. 2), made on white papers, are pasted on a grey (faded green) cardboard and concern a case, identified as “Trouillet’s case” at its bottom (Fig. 2 and Fig. 4). They include sections of the medulla oblongata and spinal cord, shown in the superior part of the card (Fig. 3) and labeled a, b, c, d, and two views of the adductor pollicis muscle, which occupy the inferior part and are labeled a and b (Fig. 4). A microscopic view of “altered slender columns” of the spinal cord (Fig. 5), possibly from another case, has been directly pasted on the right side of the page as shown in Fig. 2.
Fig. 2. General view of page 12 of the album dealing with amyotrophic lateral sclerosis. Three drawings are pasted on a grey (faded green) cardboard (arrows). They show sections of the central nervous system (at the top) and of the adductor pollicis (at the bottom). In the lower right corner of the card, “Cas de Trouillet” (Trouillet’s case) can be read. An additional drawing on the right illustrates two microscopic aspects of an “altered slender column [of the spinal cord]”. The views of “Trouillet’s case” are not dated but, as we found a great similarity between the drawings of the album and the engravings of the 12th lesson (Charcot, 1873, pp 221, fig. 16-19), we are inclined to believe that they are anterior to 1873. We could not elucidate the identity of that Trouillet, probably the doctor who referred the patient to Charcot. Charcot gave the names of the two ALS cases that he published previously, as was usual at the time. The first case, Catherine Aubel, was published in a paper entitled “Two cases of progressive muscular atrophy with lesions of the grey matter and of the anterolateral fascicles of the white matter” (Charcot and Joffroy, 1869, first case, p 354 reproduced in Charcot, 1873, p 402). The disease of the second case of that paper (named A.C.) is not reported in the lessons and is not identified as ALS by Charcot. The second case identified as ALS, Elisabeth P., was published with only Gombault as its author (Gombault, 1871). It is reproduced in the Lessons (Charcot, 1873, p 416) with Charcot’s commentary “with the collaboration of Gombault” as if he, Charcot, known for his authoritarianism, was the first coauthor. Trouillet is not mentioned in those two articles. As Charcot indicated that his lesson was based on the study of five clinical-pathological cases (Charcot, 1873, p 228, footnote 1) and as three cases are identified (Catherine Aubel, Elisabeth P. and Trouillet’s case), two remain unidentified and, as far as we know, unpublished.
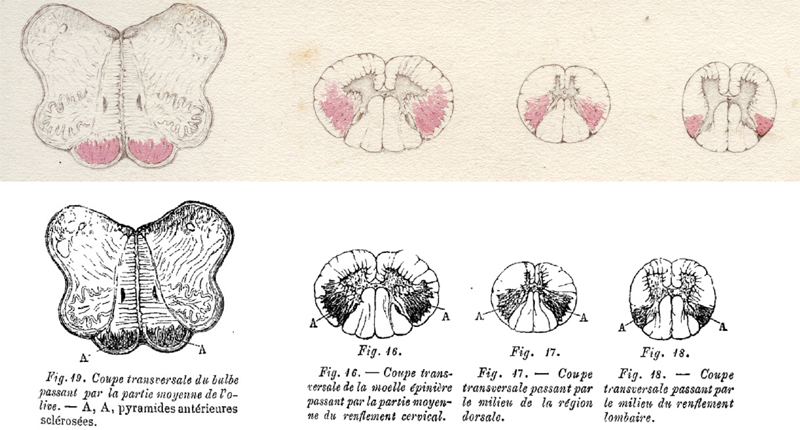
Fig. 3.
a: bulbe
which means: a: medulla oblongata; b: spinal cord at cervical level; c: at thoracic level, d: at lumbar level.
Fig. 19. Cross section of the medulla through the middle part of the olive. A, A, Sclerotic anterior pyramids Preparation of microscopic sections by Charcot (et Bouchard) The technique that has been used to obtain the illustrated sections is not reported. We can rely on two articles in which Charcot indicated how he proceeded (Charcot and Joffroy, 1869 reproduced in Charcot, 1873, pp 402-416; Charcot, 1865). The central nervous system was fixed for “nearly one month” with a “much diluted solution of chromic acid” (the fixation properties of formaldehyde were described by F. Blum two decades later – Blum, 1893). The microtome, as we know it today, was probably not in use in Paris at the time. Its invention by Purkinje in 1841 (Chvátal, 2017) or His in 1866 (Dupont, 2018) is controversial but it is clear that it was commonly used much later. The manual of histological techniques by Mathias Duval (1878), for instance, does not mention microtomes (in the current meaning) and concludes: “A large number of instruments have been invented [to cut fixed pieces]. One comes always back to the simple razor which is more efficient than all complicated ‘discotomes’ [we put in quotes] if the habit required to use it skillfully has been acquired.” The fixed sample was usually stuck in elderberry pith and cut, freehand, with a razor blade. The sections were not dehydrated and mounted in balsam or resin, as they are today. The manual of Mathias Duval (1878) indicates that one common practice was to cover the section with a coverslip (much thicker than they are today) and to introduce between the slide and the coverslip, on one side, a drop of glycerol that would diffuse and push the water out on the other side. The coverslip could then be sealed with wax or bitumen of Judea (Duval, 1878).
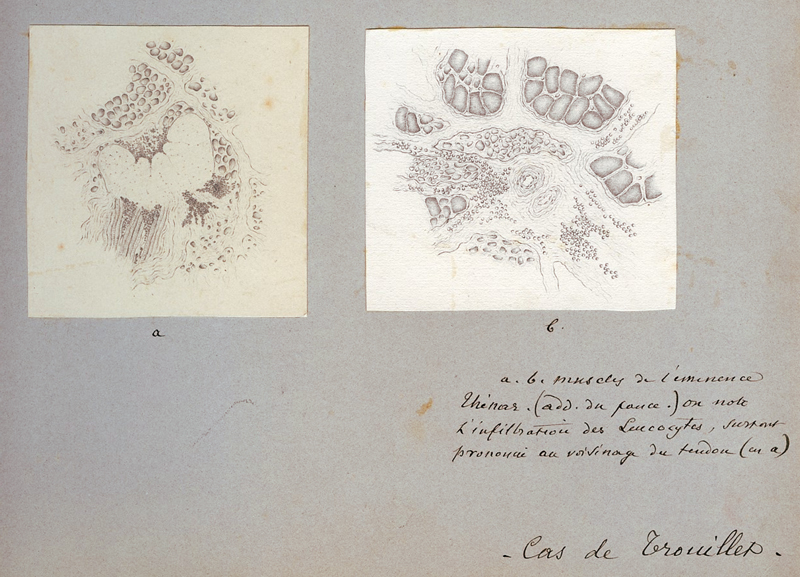
Fig. 4. Two drawings, labeled a and b, are visible in the lower part of the page.
a: one aspect of the adductor pollicis. A tendon appears as an unstained mass in the center of the section. Numerous atrophic fibers are visible. The staining was obtained with a few drops of “a concentrated solution of ammoniacal carmine”. “[…] the sick parts take a violet color, darker when the alteration is more severe. The stain of the healthy part remains unchanged.” (Charcot, 1865, p 31). “This procedure, to make more sensitive to the eye the alterations of sclerosis, which has been erased by the maceration in chromic acid, belongs to M. Bouchard”, then an intern in Charcot’s department and later professor of general pathology at Paris Medicine Faculty. What did ammoniacal carmine stain in sections fixed by chromic acid? We have no definite answer to this question. Astrogliosis is a good candidate. Several methods were developed later to stain “fibrous nevroglia” with crystal violet or other phenyl methane dyes (such as Weigert’s or Holzer’s methods), but the intimate mechanism of the staining remained unknown (Proescher, 1934). The lower square view (at the highest magnification) shows “altered slender columns [literally cords]”, most probably the lateral column, after treatment by acetic acid (as mentioned: “après acide acétique”), a practice that was usual at the time. Mathias Duval (1878) writes in his manual (p 211-212) “The most important [of the “insulating reagents”] and the most used is acetic acid: its special action is to swell and make the connective or laminous fibers disappear, and as there are few tissues where these fibers are not in a certain abundance and do not veil the other elements, there are few preparations in which acetic acid is not used.” Charcot mentions that “We have taken for comparison some very nice preparations of healthy spinal cord which we owe to the kindness of Mr. Lockhart Clarke” (Charcot and Joffroy, 1869, p 366). It is interesting to note that the technique used by Lockhart Clarke was different: the fixation of the tissue was obtained with spirit of wine; the section was then treated with one part of acetic acid and three parts of spirit of wine before being cleared in turpentine oil and observed under a coverslip: in other words, the fixation was alcoholic and there was no staining. Lockhart Clarke’s pictures of the spinal cord were of an exceptional precision and beauty (Lockhart Clarke, 1851, 1858). A case of Lockhart Clarke is cited by Charcot as possible cases of ALS (Turner et al., 2010; Radcliffe and Lockhart Clarke, 1862). The method used to prepare the muscle samples that were drawn in Trouillet’s case is also not indicated. Charcot and Joffroy examined the muscle directly and immediately (“in the fresh state”), dissociating the fibers with needles in the case of Catherine Aubel (Charcot and Joffroy, 1869, p 362). Vulpian (1869), at the same time, mentions that he examined the muscle fibers after fixation in a dilute solution of chromic acid. In the case of Trouillet, this fixation also must have been applied, as Charcot’s careful drawings necessarily took a certain amount of time that an unmounted and unfixed preparation would not have allowed.
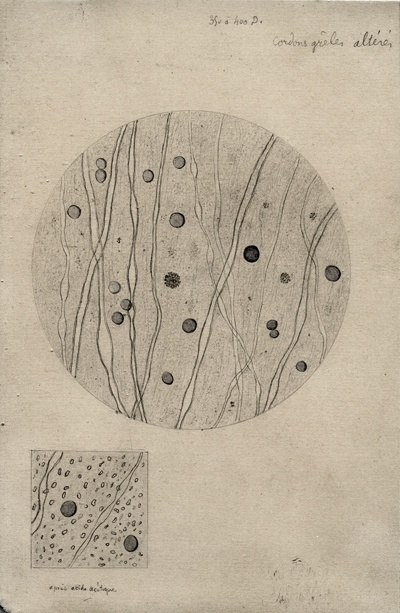
Fig. 5. Microscopic view of an “altered slender column” of the spinal cord. At the top, one reads “350 to 400 D[iameters]” (the magnification) and below the lower view “After acetic acid” (“Après acide acétique” – see text for explanation). The drawings The drawing of Trouillet’s case shows in red the pyramids of the medulla oblongata and the lateral column of the spinal cord, over-colored by ammionacal carmine. Charcot insisted upon the sparing of a fascicle of white matter, outside the pyramidal tract and just below the surface of the spinal cord: “On transverse sections, at the level of the cervical enlargement, the symmetrical alteration is greater in width than anywhere else. The area invaded by the sclerosis reaches anteriorly, and even exceeds the external angle of the anterior horn. Posteriorly, it almost reaches the posterior grey matter. Laterally, however, it is constantly separated from the cortical layer of the spinal cord by a spared bundle of white matter” (Charcot, 1873, pp 220-221). The microscopic view shown on the right of the page (Fig. 5) may have belonged to another case and illustrate “altered slender columns” [of the spinal cord] at a magnification of “350 to 400 D[iameters]”. It shows oligodendroglial nuclei and scanty myelin sheaths. The loss of fibers that it probably intended to show is impossible to ascertain without comparison with a normal case. Two views of the adductor pollicis muscle are shown (Fig. 4, a and b). The fascicular atrophy is evident on panel b. Charcot reported “infiltration by leukocytes, predominant near the tendon” (Fig. 4, a). The tendon is the unstained mass in the center. It is difficult to ascertain the presence of leucocytes. It could as well be atrophic muscle fibers. Charcot’s interpretation Charcot describes the effects of the lesions of the anterior horn of the spinal cord in his 11th lesson, and of the lateral column of the spinal cord in the 12th and 13th lessons, the association of both lesions affecting anterior horn and lateral column, defining ALS. The lesion of the anterior horn and muscle atrophy: According to Charcot’s description, the “large cells” of the anterior horn appear too few and atrophic, and the “neuroglia” is “sclerotic” (Charcot, 1873, p 223). The anterior roots and the nerves are atrophic. Charcot had understood that the muscle atrophy, visible at clinical examination, was due to the lesion of the anterior horn and was related to atrophy of the muscle fibres, visible at microscopic examination, contrarily to what is observed in muscle atrophy due to inactivity. “Motor inertia caused in the lower limbs by the suppression of cerebral action may be complete, absolute. Muscles, however, in such cases, do not lack nutrition or only in the long run because of protracted inaction” (Charcot, 1873, p 199). The anterior horn provides the “nutrition” for the muscle – “nutrition” is a term Charcot uses repeatedly in the study of the lesions of the anterior horn. The atrophy of denervated muscles had been previously described among others by Vulpian (1869), a colleague and friend of Charcot. Charcot thought that the lesion of the anterior horn was responsible for the fasciculations that he named “fibrillar twitching”. (He added a remark that experienced neurologists could still make today: “I could add that [such fibrillar twitching] is not only seen in progressive muscular atrophy, but also in healthy subjects. It may then constitute one of the symptoms of a peculiar form of hypochondria, rather frequent, incidentally, in medical students.”) He considered that the involvement of the anterior horn spared the “faradic contractility” (contrarily to the primary involvement of the muscle). In his view, the involvement of the anterior horn was “secondary” to the lesion of the lateral column (hence, the term “deuteropathic” applied to the “chronic spinal amyotrophy” observed in ALS). “The progression of the inflammatory lesion from the fascicles of the white matter to the grey matter very likely takes place […] through the nervous tubes that physiologically connect more or less directly the two regions”. What was the meaning of the word “inflammation” at that time? Certainly not the meaning of “neuroinflammation” as we understand it today. Cohnheim (1873) was just publishing his observation on the course of inflammation as observed in thin, transparent tissue. With this experimental model, he could observe diapedesis. Metchnikoff had not yet discovered phagocytosis (1893, Metchnikoff, 1968). It is also worth mentioning here that the microglia have been described much later by del Rio Hortega (1919). The use of the term inflammation by Charcot does not correspond, from today’s perspective, to his neuropathological description of the lesions: he did not describe leucocyte infiltration of the white or grey matter of the spinal cord. How could an “inflammatory lesion” progress “through the nervous tubes”? In this context, was the term “inflammation” used as a synonym for “lesion”? The lesion of the “lateral fascicle”, named later “pyramidal tract”: Although the plantar reflex had not yet been described by Babinski (1896), Charcot believed that the motor deficit was initially due to the lesion of the lateral fascicles, rather than to the lesion of the anterior horns. Muscle stiffness was a sign of the involvement of the same fascicle. The autonomy of the “system of the lateral fascicles” or simply of the “lateral fascicle” was discussed at length. He uses embryology to support his reasoning (Charcot, 1873, 12th lesson, pp 215-218), showing that both the lateral fascicle and “Türck’s bundle”, localized in the anterior column and altered in some cases of ALS, developed late in the spinal cord, in an “autonomous” manner. The description of the anatomy is both more precise and functional in his lessons of 1876 (Charcot, 1876; translated in English in 1883 - Charcot, 1883), probably in relation with his recent acquaintance with Flechsig’s work, abundantly referred to but without quotation. Flechsig, head of the histology department and later professor of psychiatry in Leipzig, used the chronology of myelination during development to recognize the spinal cord fascicles. They are correctly identified in Charcot’s Figure 46 “after Flechsig” (Charcot, 1876, p 179): the term “system of the lateral fasciculus” (Charcot, 1873, p 220 with figures on p 221) is replaced by that of the crossed “pyramidal tract” (Charcot, 1876, p 179), due to Türck, who, as a professor of neurology in Vienna, developed the method of secondary degeneration to follow the spinal cord bundles (Türck, 1851). Charcot shows pictures of the spinal cord stained by osmic acid: “Thus, on a plate of Flechsig that I am passing before your eyes and relating to the spinal cord of a newborn, you can see the following particularities: all the parts tinted in black are the developed parts: the cylinder-axis is surrounded by myelin sheath…” The pyramidal tracts, still unmyelinated, remain white (Charcot, 1876, fig. 48 and 49, p 188-189). Charcot had understood that the “autonomous development of the pyramidal tracts” was related to a late myelination. The spared bundle of white matter, outside of the pyramidal tract, precisely illustrated in the album (Fig. 3) is in his 1875 lessons (Charcot, 1876) correctly identified as the dorsal spinocerebellar tract (Flechsig’s bundle or direct spinocerebellar tract): “As for the base of the triangle [made by the pyramidal tract], directed outwards, it is separated from the pia-mater by a band of nervous substance forming a sort of mantle for it and consisting of the direct cerebellar fascicles. But this arrangement occupies only the upper half of the medullary cord; below the dorsal region, the cerebellar bundles end and, in the lumbar region, where there is no trace of them left, the crossed pyramidal bundles touch the pia-mater” (Charcot, 1876, pp 191-192). Charcot’s description of the motor symptoms, based on his clinical-pathological method (Goetz, 2000) is now fully achieved and underlines the systematic aspect of the atrophy, and its functional significance. Charcot underlined the absence of sensory deficit in ALS. He knew that the lesion of the posterior columns were linked with “locomotor ataxia” but there is a stark contrast, in the lessons dealing with “localization”, between the knowledge that Charcot had of the pyramidal tract and the difficulties that he still met in understanding the somatosensory pathways. He could state, for example, that for sensitivity, there is “indifferent conduction through this or that element of the spinal cord” (Charcot, 1876, p 282). In Charcot’s view the typical progression of ALS started in the upper limbs on one side, affecting secondarily the lower limbs, sparing the nerves innervating the vesical and rectal muscles, and ending with “labio-glosso-pharyngeal” paralysis, the nerves located above the VIIth cranial nerve being unaffected. The various clinical aspects of ALS remained, at the time, to be described. A note on the historical context Charcot used to quote rather extensively the literature, at least according to the standards of the time. His library, still visible today, testifies of the extent of his interests. He cited several cases of the literature from France, Germany and the United Kingdom in support of his analysis. The second volume of the lessons, however, was published in 1873, three years only after the siege of Paris by the Prussian troops. People caught in Paris during the siege were hungry and ate dogs, horses, rats and even elephants and antelopes from the zoo (as told by Victor Hugo in his book “Choses Vues” – Hugo, 1900 passim and pp 299, 308)! Charcot had sent his wife and his three children to Normandy, outside Paris where he, personally, continued to work at the hospital (Bonduelle et al. 1996, p. 296). If Charcot used to remain on purely scientific grounds, it is not impossible that the comments on a paper by Nikolaus Friedreich (professor of pathological anatomy in Würzburg, later professor of pathology and therapy in Heidelberg) were tinged with a certain resentment: “Such a neglect in matters of nosographic distinctions, especially in a question in itself rather obscure, is at least regrettable and can only maintain the confusion” (Charcot, 1873, footnote 1, p 208). Such a critical remark is counterbalanced by a good knowledge of the German literature. It is Charcot who names the direct corticospinal tract Türck’s bundle (referring to Türck, probably Türck, 1851) and underlines the importance of Flechsig (unfortunately without quotation) in the functional understanding of the disease that he was identifying (Charcot, 1876, p 191). Flechsig published an early and impressive synthesis of his work in 1876 (Flechsig, 1876); he was only 29. Conclusion It may finally be considered that the wish that Charcot expressed in his lesson has been fulfilled: “I must first declare that the reports on which my description is based, are still few, twenty at the most. But one must notice that it was also the case, some time ago, concerning progressive locomotor ataxia. The clinical picture drawn by Duchenne (de Boulogne) with the help of a small number of facts, nearly 20 years ago, has not aged. [...] May my description of amyotrophic lateral sclerosis experience the same fate!” (Charcot, 1873, p 228) Acknowledgement The help of Véronique Leroux-Hugon, previous curator of Charcot Library, and of Florian Horrein, the current curator, is greatly acknowledged. Charcot’s album belongs to the “Musée de l’Assistance Publique-Hôpitaux de Paris”, which we thank, and kept in the Neuropathology Department of La Salpêtrière Hospital. References Babinski J. (1896) Sur le réflexe cutané plantaire dans certaines affections du système nerveux central. C R Seances Soc Biol. 3: 207-208. Blum F. (1893) Der Formaldehyd als Hartungsmittel. Z Wiss Mikrosk. 10: 314-315. Bonduelle M., Gelfand T., Goetz C.G. (1996) Charcot, un grand médecin dans son siècle. Michalon Publisher, Paris. Charcot J.-M. (1865) Sclérose des cordons latéraux de la moelle épinière, chez une femme hystérique, atteint de contracture permanente des quatre membres. Bull Mém Soc Méd Hôp Paris. 2: 24-35. [The document may be accessed on the internet: https://gallica.bnf.fr/ark:/12148/bpt6k5440456t/f36.item ] Charcot J.-M. (1873) Leçons sur les maladies du système nerveux faites à La Salpêtrière par J.M. Charcot, recueillies et éditées par Bourneville. IIe série. Adrien Delahaye Publisher, Paris. [The book may be accessed on the internet: https://gallica.bnf.fr/ark:/12148/bpt6k6149090r/f12.item ] Charcot J.-M. (1876) Leçons sur les localisations dans les maladies du cerveau et de la moëlle épinière, faites à la faculté de médecine de Paris, recueillies et publiées par Bourneville et Brissaud (1875). A. Delahaye & Lecrosnier Publisher, Paris. [The book may be accessed on the internet: https://gallica.bnf.fr/ark:/12148/bpt6k773614/f177.item ] Charcot J.-M. (1883) Lectures on the localization of cerebral and spinal diseases delivered at the faculty of medicine of Paris translated and edited by Walter Baugh Madden. The new Sydenham Society. Volume CIL. [The book may be accessed on the internet: https://archive.org/details/lecturesondiseas02char ] Charcot J.-M. (1892) Leçons du mardi à La Salpêtrière. Policlinique 1887-1888. Notes de cours de MM. Blin, Charcot et H. Colin, élèves du service. Vve Babé Publisher, Paris. [The book may be accessed on the internet: https://gallica.bnf.fr/ark:/12148/bpt6k55646784/f4.item.r=fig ] Charcot J.-M., Joffroy A. (1869) Deux cas d’atrophie musculaire progressive avec lésions de la substance grise et des faisceaux antérolatéraux de la moelle épinière. Arch Physiol Norm Pathol. 2 : 354-367, 629-649, 744-760 (Note that the paper was published in three parts, in different issues of the journal.) [The paper may be accessed on the internet: https://gallica.bnf.fr/ark:/12148/bpt6k432734s/f354.item ] Chvátal A. (2017) Jan Evangelista Purkyně (1787-1869) and his instruments for microscopic research in the field of neuroscience. J Hist Neurosci. 26: 238-256. Cohnheim J. (1873) Neue Untersuchungen über die Entzündung. August Hirschwald, Publisher, Berlin. Dupont J.C. (2018) Historical perspective on neuroembryology: Wilhelm His and his contemporaries. Genesis. 56: 6-7. Duval M. (1878) Précis de technique microscopique et histologique ou introduction à l’anatomie générale. J.-B. Baillière et Fils Publisher, Paris. [The book may be accessed on the internet: https://gallica.bnf.fr/ark:/12148/bpt6k9618339x.texteImage ] Flechsig P. (1876) Die Leitungsbahnen im Gehirn und Rückenmark des Menschen auf Grund entwickelungsgeschichtlichter Untersuchungen. Wilhelm Engelmann Publisher, Leipzig. Goetz C.G. (2000) Amyotrophic lateral sclerosis: early contributions of Jean-Martin Charcot. Muscle Nerve. 23: 336-43. Hugo V. (1900) Choses vues. Nouvelle série. Calmann-Lévy Publisher, Paris. [The book may be accessed on the internet: https://gallica.bnf.fr/ark:/12148/bpt6k141436z.r=Victor%20Hugo%20choses%20vues?rk=21459 ] Gombault M. (1871) Sclérose symétrique des cordons latéraux de la moelle et des pyramides antérieures dans le bulbe. – Atrophie des cellules des cornes antérieures de la moelle.—Atrophie musculaire progressive. – Paralysie glosso-laryngée, Arch Physiol Norm Pathol. 4: 509-518 [The paper may be accessed on the internet: https://gallica.bnf.fr/ark:/12148/bpt6k432736j/f517.item ] Lockhart Clarke J. (1851) Researches into the structure of the spinal chord. 141: 607-621 [The paper may be accessed on the internet: https://royalsocietypublishing.org/doi/pdf/10.1098/rstl.1851.0029 ] Lockhart Clarke J. (1858) Researches into the intimate structure of the brain, human and comparative. First series. On the structure of medulla oblongata. Philos Trans R Soc Lond. 148: 231-259 [The paper may be accessed on the internet: https://wellcomelibrary.org/item/b22297169 ] Metchnikoff E. (1968) Lectures on the Comparative Pathology of Inflammation, Delivered at the Pasteur Institute in 1891 Dover Publications Publisher, Mineola. Proescher F. (1934) Contribution to the staining of neuroglia. Stain Technology. 9: 33-38 [The paper may be accessed on the internet: https://doi.org/10.3109/10520293409116130 ] Radcliffe C.B., Lockhart Clarke J. (1862) An important case of paralysis and muscular atrophy with disease of the nervous centres. Brit & Foreign Medico-Chirurgical Rev. 30: 215–225 Río-Hortega P. (1919) El "Tercer elemento” de los centros nerviosos. I. La microglía en estado normal, Boletín de la Sociedad Española de Biología. 8: 67-82 Seilhean D. (2020) Neuropathology in Pitié-Salpêtrière hospital: past, present and prospect. Neuropathology. 40: 3–13. doi:10.1111/neup.12616. [The paper may be accessed on the internet: https://onlinelibrary.wiley.com/doi/full/10.1111/neup.12616 ] Türck L. (1852) Über secundäre Erkrankung einzelner Rückenmarkstränge und ihrer Fortsetzung zum Gehirne. Akad Wissensch Wien Math Naturwiss Class Sitzungber. 8: 511-534. Turner M.R., Swash M., Ebers G.C. (2010) Lockhart Clarke’s contribution to the description of amyotrophic lateral sclerosis. Brain. 133: 3470-3479. [The paper may be accessed on the internet: https://academic.oup.com/brain/article-pdf/133/11/3470/882976/awq097.pdf ] Vulpian A. (1869) Sur les modifications que subissent les muscles sous l’influence de la section de leurs nerfs. Arch Physiol Norm Pathol. 2: 558-578. [The paper may be accessed on the internet: https://gallica.bnf.fr/ark:/12148/bpt6k432734s/f558.item ]
Copyright: © 2021 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |