|
|
|
Free Neuropathology 2:8 (2021) |
|
Opinion Piece |
|
The definition and role of brain invasion in meningioma grading: Still controversial after all these years |
|
Arie Perry |
|
Department of Pathology, Division of Neuropathology, University of California San Francisco (UCSF), San Francisco, CA 94143, USA |
|
Corresponding author: |
|
Submitted: 05 March 2021 Accepted: 23 March 2021 Copyedited by: Nima Sharifai Published: 24 March 2021 |
|
Keywords: Meningioma, Brain invasion, Grading |
|
In their landmark 1938 monograph on meningiomas, Cushing and Eisenhardt stated that brain invasion, defined similarly to today by tumoral penetration of the pia, had long been considered a sign of malignancy1. Although this was accepted as undisputed gospel over the following decades, the precise role of brain invasion in meningioma grading and how to best define it remains unanswered nearly a century later. For instance, in 1993, McLean and colleagues questioned the role of brain invasion in grading, since they found no additional prognostic significance of this finding within their 28 otherwise atypical and anaplastic meningiomas; unfortunately, they did not address the controversial issue of brain invasive otherwise benign (BIOB) meningiomas2. Similarly, the second edition of the World Health Organization (WHO) classification scheme in 1993 highlighted that “some participants maintained that gross brain invasion, not only metastasis, qualifies a tumor for the designation malignant; such lesions do not invariably exhibit histological malignancy and their immunocytochemical features may be similar to those of ordinary meningiomas”3. I suspect that the term “gross” in this phrase meant well-developed or extensive, rather than the surgeon’s gross impression. Of course, the significance of brain invasion is a topic near and dear to my heart, as it was one of the first questions I tried to tackle in my neuropathology career, first in a 1997 Mayo Clinic clinicopathology study of meningioma grading criteria and then in a followup 1999 series addressing the issue of brain invasion and other pathologically defined forms of potential malignancy4,5. Along with my mentor, Bernd Scheithauer, Scott Stafford (Radiation Oncology), and other collaborators, we proposed a grading scheme based on statistically significant associations between histopathologic variables and estimated patient survival times (recurrence-free and overall). A fact that is often forgotten today is that these associations were specifically limited to the cohort of patients treated with gross total resection, given that subtotally resected meningiomas frequently recurred regardless of microscopic features. To a large extent, our grading criteria were adopted in the 3rd edition of the WHO scheme in 20006 and have remained fairly intact ever since. Based on our data that BIOB meningiomas had recurrence and mortality rates similar to atypical meningiomas without brain invasion, it was emphasized that such cases are prognostically equivalent to WHO grade II meningiomas. However, it was not until the revised 4th edition of the WHO in 2016 that brain invasion was adopted as a definitive criterion for the diagnosis of atypical meningioma, WHO grade II7.
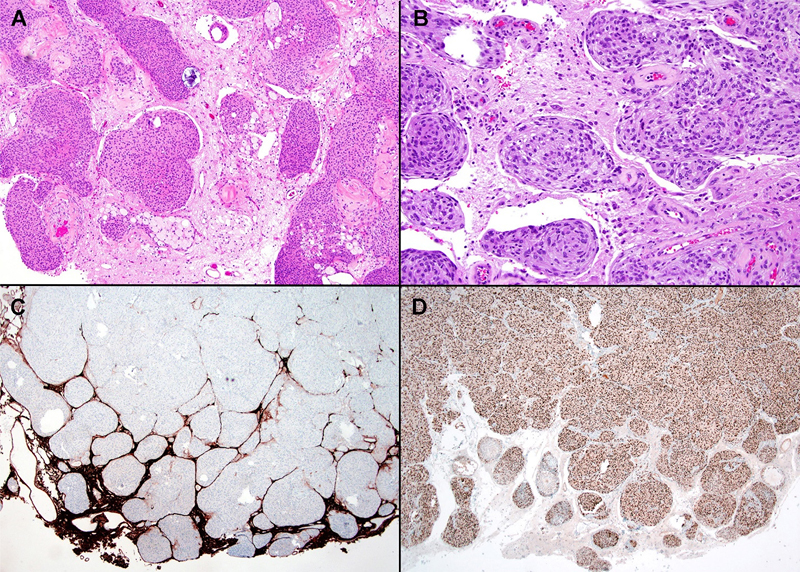
Figure 1. Examples of well-developed and extensive brain invasion that would likely be associated with high interobserver reproducibility. A, B. Note the tongue-like or finger-like protrusions into adjacent brain with no obvious leptomeningeal layer between the two. C. A GFAP stain shows entrapped slivers of gliotic CNS parenchyma deep within the main tumor mass (upper portion). D. This brain invasive otherwise benign (BIOB) meningioma showed benign histologic features, including extensive progesterone receptor expression. Images C and D are courtesy of Dr. Robert Schmidt, Washington University, St. Louis, MO, USA. Given that we found brain invasion in 4% of cases in our 1997 series, and just 23% of brain invasive meningiomas were otherwise benign in our 1999 expanded series, I expected that this classification change in 2016 would only have a minimal impact on clinical practice (with an expected increase in the incidence of WHO grade II meningiomas of 1% at best). In other words, this would be the estimate if BIOB meningiomas only account for a fourth of the roughly 4% of brain invasive tumors, assuming that everyone was previously diagnosing such cases as WHO grade I rather than II, which is clearly not true since some were already designating such cases as grade II. To my surprise, however, I have personally noticed a mini-epidemic in BIOB meningiomas in my personal consults and especially in a clinical trial for which I am serving as the central pathology reviewer. Of interest, I previously served in a similar role for a pre-2016 RTOG/NRG clinical trial that included meningiomas of all three grades; in this series we found a strong concordance rate of 92.4% between the home pathologist’s interpretations of brain invasion and my own (kappa statistic 0.76)8. However, in this post-2016 followup trial focused specifically on atypical meningiomas, there have already been quite a few cases that I have rejected because they initially qualified as grade II based on focal brain invasion alone, but I disagreed with that call during my central review. Admittedly, this is merely an anecdotal impression on my part rather than hard data, given that the study is still accruing cases and no formal analyses have been performed. Nonetheless, it might not be surprising if people have loosened their minimal criteria for calling brain invasion after the 2016 WHO, since it is only human nature (especially among pathologists) to not want to miss even the tiniest example of something if it has a potentially important association with outcome. However, I would argue the opposite approach in favor of stricter criteria so that one does not dilute the potential impact of this prognostic marker with questionable examples. In other words, if brain invasion is the only reason to upgrade a tumor, then I would rather it to be irrefutable before assigning that higher grade.
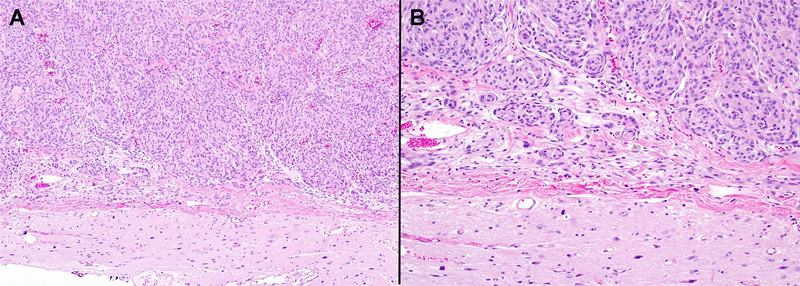
Figure 2. A, B. Most meningiomas with attached CNS parenchyma can be clearly interpreted as being non-invasive, given the broad, linear interface and clear leptomeningeal layer between the tumor and adjacent brain parenchyma. Additionally, the modified WHO 2016 criteria sparked a renewed interest in this controversy and some of the subsequent clinicopathologic series have failed to find any prognostic differences between their BIOB and non-invasive WHO grade I meningiomas9-11. In contrast, a 2016 study of 206 WHO grade II meningiomas found brain invasion to be an independent negative prognostic variable on multivariate analysis12. Another study of WHO grade II meningiomas found that brain invasion was prognostic only if specifically combined with the presence of necrosis13, even though a non-invasive meningioma with necrosis only would normally be considered as otherwise benign. For a more detailed summary of the strengths and limitations of previously published studies on this topic, the reader is referred to the review of Brokinkel, Hess, and Mawrin14. Suffice it to say that there are still no large, highly powered studies of strictly defined, gross totally resected BIOB meningiomas with long clinical followup times, given the overall rarity of such cases. As such, this question remains unanswered and the upcoming 5th edition of the WHO (in press) will include the following text on the question of brain invasion: “Brain invasion by meningioma is characterized by irregular, tongue-like protrusions of tumour cells into underlying GFAP-positive parenchyma, without intervening leptomeninges. Extension along perivascular Virchow-Robin spaces does not constitute brain invasion because the pia is not breached. Such perivascular spread and hyalinization is most commonly encountered in children and can mimic meningioangiomatosis, but does not constitute true brain invasion15,16. Brain invasion occurs most often in meningiomas with additional high-grade features. Nonetheless, the presence of brain invasion in gross totally resected, otherwise benign-appearing meningiomas remains controversial, as it has been associated with recurrence rates similar to other WHO grade 2 meningiomas in some, but not all studies5,10,11; larger series with longer follow-up times may be needed to resolve this issue.” Given the issues raised above, I decided to write this opinion piece and offer my personal views on what does or does not constitute brain invasion, recognizing that this is at best an educated guess and there is no guarantee that I am any more likely to be correct than authors with opposing viewpoints. As a reminder, most cases with brain invasion will qualify for a higher histologic grade using other criteria anyway, and cases with absolutely no other worrisome features are generally rare. Nevertheless, when encountering a BIOB meningioma on routine histopathology, it is perhaps best at this time to: 1) obtain GFAP and other immunostains (IHC) to clarify the brain invasion in borderline cases, 2) order molecular studies to look for other prognostically relevant biomarkers (e.g., specific chromosomal losses, CDKN2A homozygous deletion, TERT promoter mutation, etc.), 3) spell out the remaining uncertainties over the clinical significance of these rare cases in the pathology report, and/or 4) suggest close clinical followup just in case the tumor does behave in a more aggressive fashion.
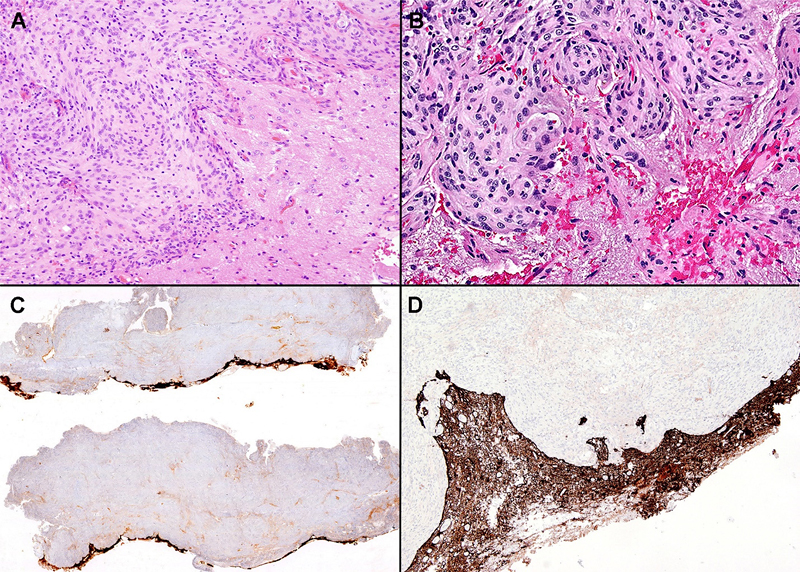
Figure 3. Challenging cases that are more likely to yield discordant interpretations. A. Although the interface is irregular rather than linear, there is a discernible leptomeningeal layer between meningioma and brain; as such, I would not call this brain invasion. B. There is a focally irregular interface in this case and it is difficult to determine whether or not there is intervening leptomeninges; a GFAP stain could help push me in one direction or the other in such a case. C, D. GFAP stains in this case highlight a gently undulating tumor-CNS interface; however, in contrast to figure 1C, there is minimal if any definite GFAP-positive tissue within the main tumor mass. If this was the only worrisome feature in this meningioma, I would err on the side of caution and not accept this as definite brain invasion. In terms of minimal criteria for brain invasion, a common question is whether or not the surgeon’s intraoperative impression can serve as a surrogate. To my knowledge, all studies published to date have shown a much higher frequency of brain invasion on gross impression than that which is confirmed under the microscope, possibly due to cases with simple adhesion to leptomeninges being overcalled macroscopically. More importantly, with only one exception17, none of the published studies have found a statistical association with grossly diagnosed brain invasion and subsequent recurrence-free survival. As such, the gross intraoperative impression of brain invasion should not be considered a reliable surrogate. That said, of course, the detection of brain invasion is highly dependent on sampling issues and it therefore could be especially useful for the pathologist if the surgeon labels the tumor-brain interface or areas most suspicious for invasion intraoperatively. The importance of appropriate sampling has also been emphasized by other authors and, not surprisingly, the frequency of finding brain invasion increases with greater sampling or perhaps with additional guidance from the surgeon, more targeted sampling. That said, the reported frequency of brain invasion in 33% of otherwise benign meningiomas, by Pizem and colleagues in 201418, seems remarkably excessive to me, even in meningiomas that are extensively sampled. In any case, I believe that the original definition of brain invasion, which requires a breach of the pial barrier, is still the best method. In my experience, the two scenarios that are most often mistaken for (or do not show sufficient evidence of) microscopic brain invasion are: 1) an irregular interface with adjacent brain that nevertheless shows an intervening layer of leptomeninges/collagen and 2) perivascular spread along Virchow-Robin spaces. Examples of these and less controversial scenarios are illustrated. Additionally, one should be cautious of overcalling brain invasion in highly cauterized or otherwise poorly preserved fragments of tissue.
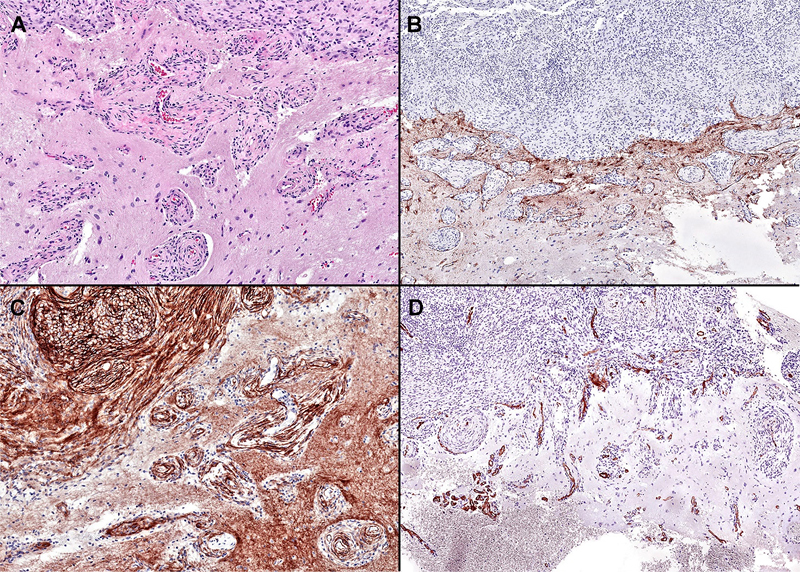
Figure 4. A. There is extensive tumoral spread along perivascular Virchow-Robin spaces in this example, which could easily be misinterpreted as either brain invasion or associated meningioangiomatosis. However, careful examination shows the perivascular arrangement and since this is not considered a breach of the pial barrier, it does not qualify as brain invasion. This type of spread is often associated with radial collars of spindled tumor cells and hyalinization, similar to that seen in meningioangiomatosis. B. A GFAP stain fails to show any convincingly entrapped glial tissue within the main tumor mass (upper portion). C. A somatostatin receptor 2A stain highlights the onion-like radial layers of perivascular tumor cells; note that the brain is also normally positive but displays a fibrillar staining pattern distinct from the spindled meningioma cells. D. The mostly centrally placed blood vessels within the Virchow-Robin spaces are highlighted on this smooth muscle actin immunostain. Although this pattern of spread is more often encountered in pediatric patients, this one was from an adult. Based on the above, my sincere plea is that we all adopt strict rather than loose criteria for brain invasion going forward, so that if this variable really does provide independent prognostic information, we will be in a better position to detect it. To quote the Haarlem white paper from 2014, “diagnostic entities should be defined as narrowly as possible to optimize interobserver reproducibility”19 (or in this case a grading parameter rather than an entity). References 1. Cushing H, Eisenhardt L. Meningiomas: their classification, regional behaviour, life history, and surgical end results. Springfield, IL: CC Thomas; 1938. 2. McLean CA, Jolley D, Cukier E, Giles G, Gonzales MF. Atypical and malignant meningiomas: importance of micronecrosis as a prognostic indicator. Histopathology. 1993;23(4):349-353. 3. Kleihues P, Burger P, Scheithauer B. Histological typing of tumours of the central nervous system. In: Sobin L, ed. World Health Organization. International histological classification of tumours. 2nd ed. Berlin: Springer; 1993. 4. Perry A, Stafford SL, Scheithauer BW, Suman VJ, Lohse CM. Meningioma grading: an analysis of histologic parameters. Am J Surg Pathol. 1997;21(12):1455-1465. 5. Perry A, Scheithauer BW, Stafford SL, Lohse CM, Wollan PC. "Malignancy" in meningiomas: a clinicopathologic study of 116 patients, with grading implications. Cancer. 1999;85(9):2046-2056. 6. Louis D, Scheithauer B, Budka H, von Deimling A, Kepes J. Meningiomas. In: Kleihues P, Cavenee W, eds. World Health Organization classification of tumours. 3rd ed. Lyon: IARC Press; 2000:176–189. 7. Perry A, Louis DN, Budka H, et al. Chapter 10: Meningioma. In: Louis DN, Ohgaki H, Wiestler OD, et al., eds. WHO classification of tumours of the central nervous system (Revised 4th edition). Lyon: IARC; 2016:232-245. 8. Rogers CL, Perry A, Pugh S, et al. Pathology concordance levels for meningioma classification and grading in NRG Oncology RTOG Trial 0539. Neuro Oncol. 2016;18(4):565-574. 9. Spille DC, Hess K, Sauerland C, et al. Brain Invasion in Meningiomas: Incidence and Correlations with Clinical Variables and Prognosis. World Neurosurg. 2016;93:346-354. 10. Baumgarten P, Gessler F, Schittenhelm J, et al. Brain invasion in otherwise benign meningiomas does not predict tumor recurrence. Acta Neuropathol. 2016;132(3):479-481. 11. Biczok A, Jungk C, Egensperger R, et al. Microscopic brain invasion in meningiomas previously classified as WHO grade I is not associated with patient outcome. J Neurooncol. 2019; 145(3):469-477. 12. Champeaux C, Dunn L. World Health Organization grade II meningiomas. Acta Neurochir (Wien). 2016. 13. Garcia-Segura ME, Erickson AW, Jairath R, Munoz DG, Das S. Necrosis and Brain Invasion Predict Radio-Resistance and Tumor Recurrence in Atypical Meningioma: A Retrospective Cohort Study. Neurosurgery. 2021;88(1):E42-E48. 14. Brokinkel B, Hess K, Mawrin C. Brain invasion in meningiomas-clinical considerations and impact of neuropathological evaluation: a systematic review. Neuro Oncol. 2017;19(10):1298-1307. 15. Giangaspero F, Guiducci A, Lenz FA, Mastronardi L, Burger PC. Meningioma with meningioangiomatosis: a condition mimicking invasive meningiomas in children and young adults: report of two cases and review of the literature. Am J Surg Pathol. 1999;23(8):872-875. 16. Perry A, Kurtkaya-Yapicier O, Scheithauer BW, et al. Insights into meningioangiomatosis with and without meningioma: a clinicopathologic and genetic series of 24 cases with review of the literature. Brain Pathol. 2005;15(1):55-65. 17. Behling F, Fodi C, Gepfner-Tuma I, et al. CNS Invasion in Meningioma-How the Intraoperative Assessment Can Improve the Prognostic Evaluation of Tumor Recurrence. Cancers (Basel). 2020;12(12).
Copyright: © 2021 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |