|
|
|
Free Neuropathology 1:24 (2020) |
|
Reflections |
|
The ’Accidental Neuropathologist' – on 40 Years in Neuropathology |
|
Harry V. Vinters |
|
Pathology & Laboratory Medicine & Neurology, David Geffen School of Medicine at UCLA, Los Angeles, CA, USA |
|
Corresponding author: |
|
Submitted: 14 August 2020 Accepted: 16 August 2020 Copyedited by: Christian Thomas Published: 25 August 2020 |
|
Additional resources and electronic supplementary material: supplementary material |
|
Keywords: Neuropathology, UCLA, Personal reflections |
|
This article is dedicated to the memory of my brother Raymond John Vinters (1952-2020). Beginnings in Canada My family were Latvians who, by the end of World War II, had become refugees from the Soviet Union. For the repressive Communist regime that controlled the USSR, my family (on both sides) were or would soon become ‘criminals’ who owned land and were involved in commerce. They saw no future under a Communist regime, and the fate of relatives who remained in Latvia after World War II confirmed the wisdom of their decision and choice – some were exiled to Siberia for many years, others simply had their property confiscated. My family – grandparents, their two children (one my father) and assorted household staff who joined them – fled the country as the Red Army moved in to ‘liberate’ its people and begin a brutal and merciless tyranny that would last until the early 1990s. During that happy time in the early 1990s the USSR thankfully collapsed under the weight of grotesque corruption and reliable, predictable, frequently comical Soviet incompetence. Members of my family lived in various refugee camps in Europe between 1944 and 1949, at which time they were sponsored by distant relatives to relocate to Canada; some of their lasting and most intimate friendships were made in the camps during those postwar years. My parents had wed in Lübeck, Germany. It was their (and my) good fortune that our family ended up on the northwest shore of Lake Superior, in the small city of Port Arthur (now integrated into a larger municipality, Thunder Bay), where I was born. If one envisions Lake Superior as having the shape of a wolf’s head, Thunder Bay is about where its eyes would be located. This beautiful small city is situated on rolling hills overlooking the lake, and is home to one of the harshest (winter) climates of any metropolitan area in Canada. It provided me with an outstanding primary and high school education at the hands of, and with the mentorship of, dedicated and devoted teachers who inspired a love of learning and a first-rate work ethic, of which they themselves were emblematic. Very lucky break for me! Winters were long and brutal in Port Arthur. I well remember sitting in my high school classes, looking out onto the harbor – Port Arthur was a port city thanks to the St. Lawrence Seaway (opened in the late 1950s, Queen Elizabeth II herself came to our fair city for the official opening), which allowed ocean-going vessels to come into the Great Lakes. The harbor was still frozen in April and May, and I longed for warmer days – never dreaming then that I would spend most of my working career in a climate that can safely be described as endless summer. I was also fortunate to have support and encouragement from a wonderful father [Figure 1] who, as a single parent, raised me and my brother after our mother left in the early 1960s to begin a new life in the USA and my parents divorced. He died in 1980 but never a day goes by that I don’t think – with much love and gratitude – of him and his dedication to his sons and family, his generosity, support and kindness. Our loving and resourceful family included grandparents, aunts and uncles, eventually cousins, all trying to find their way in the brave new world into which they had been thrust by World War II and its aftermath and sequelae. As with many immigrant families trying to establish life in a foreign land, barely speaking English and with limited finances, extended family members (usually from three generations) occupied small apartments and houses, then eventually spread their wings and left to make lives of their own in their new homes, when they could finally afford them. My favorite home in those early days was a ramshackle house – little more than a cottage – just outside the Port Arthur city limits, with two tiny bedrooms and one miniscule bathroom (bath, no shower), situated on the banks of a small meandering river and on a gorgeous piece of land. The property was also home to several massive pine trees and came to be known (by the Latvian expatriate community) as Eglaines (loosely translated, The Home of Tall Pine Trees). Seven of us called this home for many years. It had an old coal furnace in which fuel needed to be replenished during the icy winter nights, a task shared by my father and grandfather. My grandparents, who had been ‘saimnieks and saimniece’ (the master and mistress of their household) and oversaw a large farm in Latvia, lovingly cultivated their gardens of flowers, berries and vegetables on the two acres that Eglaines occupied. I often wondered what it would be like to start one’s life over, at the age of 49 or 50, in a foreign land and culture, as my resilient grandparents had; the task was easier – though no less challenging! – for my father and mother, who later became a medical technologist. My father and grandfather worked in the grain elevators that surrounded the harbor (the grain coming from Canada’s prairie provinces and destined to be loaded onto seaway-bound ships) until my dad became a real estate agent, then subsequently a real estate broker. My paternal grandmother worked as a domestic. While I loved Port Arthur (that affection continues to this day) I yearned to pursue higher education in a larger center, and a variety of scholarships allowed me to do so at the University of Toronto (U of T), another lucky twist of fate. Being a Toronto resident introduced me to the joys (and challenges…) of big city metropolitan life, and I have enjoyed urban living ever since. I adore the buzz of large cities, almost without exception. Idyllic country life, a dream for some, is not for me.
Fig 1: My father Gunnar (Gunars) Vinters, 1925-1980 During the summer between my graduation from high school and the beginning of university (1968) I had the marvelous opportunity to work in the laboratory of a family friend (and my aunt’s godmother), Irene Grodums, who after immigrating to Canada had completed her Ph.D. and become a Virologist at the University of Saskatchewan in Saskatoon. Prof. Grodums instilled in me a respect for the importance of careful observation in tissue studies, whether done by light or electron microscopy (she worked on Coxsackie virus effects on the heart) and respect for experimental animals used in biological research. In the 1970s medical school was increasingly regarded as a place of graduate studies, following upon an undergraduate experience. My first degree was in Biology and most of my courses given in the Botany Department (these days, Plant Sciences). U of T undergraduate instruction was loosely based in one of the constituent colleges, and my academic (and residential) home was University College. I thrived on living on an historic campus situated in the middle of a world class city, one with a great sense of history. One of my first summer research jobs was in the Botany Department, studying the kinetics of water movement into and out of giant algae with Profs. Jack Dainty and Mel Tyree (both accomplished Biophysicists); this resulted in my first publication [1]. While in medical school at the University of Toronto (1972-76) I developed an abiding affection for the Neurosciences, though I realized I would never have the skill set, insights, patience or scientific acumen to be a solid basic neuroscientist. Our inspiring Professors included the legendary Neuropharmacologists Phil Seeman and Oleh Hornykiewicz; Dr. Seeman (probably one of the best lecturers I have ever encountered) had previously discovered how anesthetics and tranquilizers interact with cell membranes [2] and subsequently contributed to the molecular understanding of complex genes that control dopamine receptor function, while Dr. Hornykiewicz was the discoverer of the dopamine deficiency [3] that leads to Parkinson disease. The other option was to choose a Clinical Neuroscience in which I would have both clinical responsibilities and an opportunity to do research and teaching. I decided to pursue postgraduate training in Neurology, having eliminated Neurosurgery as a career path – I lacked the required stamina and manual dexterity, both (in addition to excellent clinical judgement) requirements of a first-rate Neurosurgeon. Fortunately, throughout my career I have had the opportunity to work with some of the very best in the latter field, in numerous productive collaborations and diagnostic challenges (see below). How Neuropathology chose me Neuropathology was a largely invisible specialty while I was in Medical School. Admittedly, in the early 1970s it was itself a fledgling discipline in the Clinical Neuroscience firmament, certainly in Canada. We received wonderful lectures from Neuropathologists – including Dr. Barry Rewcastle – but were never really apprised of how a Neuropathologist spends her/his time and contributes to the diagnosis and understanding of neurologic disease. Indeed, we hardly knew that such individuals existed or how one went about becoming a Neuropathologist, this despite several significant Neuropathologic discoveries having been made at U of T’s Banting Institute on College Street, then home of the research components of the Pathology Department. (Frederick Banting, the discoverer of insulin, was the first and is still one of the few Canadians to be awarded the Nobel Prize in Medicine or Physiology). The initial report of progressive supranuclear palsy [4] was co-authored by the great Jerzy Olszewski, though he had unfortunately passed on by the time I was in Medical School. I spent my internship year at the University of Alberta Hospital in Edmonton, in retrospect a wise choice because it introduced me to the beauty of the rugged Canadian west (stunning prairie skies and amazing geography) and facilitated my meeting people who remain steadfast friends to this day. Of course that year also provided a terrific opportunity to learn important fundamentals of Medicine from energetic and knowledgeable instructors. The University of Alberta Hospital would, many years later, become a place where I would do an extended locum. I began training in Neurology in London, Ontario in 1977 in the Department of Clinical Neurological Sciences (CNS) at the University of Western Ontario / UWO (subsequently renamed Western University). This Department represented a logical fusion of talent from Neurosurgery, Neurology, Neuroradiology, and Neuropathology. Its leadership included two legends of 20th century Neurosurgery (Charles G. Drake) and Neurology (Henry J.M. Barnett). London was also a major center for stroke research; the clinical specimens we were shown in surgical pathology and at autopsy conferences inspired an appreciation and respect for the importance of cerebrovascular disease in Neurology. The weekly 3-hour city-wide Clinical Neuroscience rounds included presentations from all four of the sub-disciplines, including a clinicopathologic conference weekly or every two weeks. I was coming to an important, somewhat uneasy career juncture: Neurology felt like perhaps not quite the optimal choice of specialization for me. However… An inspirational figure during that first year of Neurology training came to be Dr. John C.E. Kaufmann, chief of Neuropathology at the (recently built) University Hospital on the main UWO campus in the north end of the city. Dr. Kaufmann (or JCEK, as his trainees knew him, Figure 2) had been recruited from South Africa to be the first Neuropathologist at UWO, and one of only a handful in Canada at the time. More than being a marvelous diagnostician, JCEK was the essence of a ‘gentleman and scholar’, someone who took responsibility for the wellbeing and mental and physical health of his trainees. I daresay most of us lucky to be in that multi-year cohort try to emulate JCEK in our own careers. He and his wife Suzanne Kaufmann loved art (they had an inspiring collection which included an Andy Warhol), entertaining on a grand scale, fine (exquisite) cuisine usually prepared in their own kitchen, good and witty conversation and travel. The presentations JCEK oversaw at the weekly Clinical Neuroscience rounds were marvels of clarity and insights into neurologic disease. Throughout that year of training in Neurology, I came to the conclusion that Neuropathology might be a more appropriate career path for me. Fortunately, Dr. Barnett was very passionate about the vital importance of Neuropathology in neurodiagnostics. When I requested the possibility of doing a full year of Neuropathology training (then configured as part of my Neurology residency) Dr. Barnett was favorable to the idea, as was JCEK. I embarked on the road to my career as a Neuropathologist with some trepidation, but a passion for the study of the anatomic basis of neurologic diseases using a multitude of special stains, which in those days (late 1970s) were, together with electron microscopy, the ‘gold standard’ for neuropathologic investigations. Oh yes, things have changed!
Fig 2: Dr. John C.E. Kaufmann, Chief of Neuropathology, University Hospital, London, Ontario, Canada My other mentors in London were Dr. Melvyn J. Ball, who was already a prominent Alzheimer researcher, and Dr. Joseph Gilbert [Figure 3], who had trained in Neurology and Neuropathology in Cleveland, though practiced the latter. Neuropathology in Canada is configured as a specialty rather than a ‘subspecialty’ requiring Fellowship training. JCEK and Joe Gilbert were in charge of NP training at the two major UWO teaching hospitals, University and Victoria, and possessed complementary, mutually reinforcing didactic skills. JCEK was an experienced, meticulous and insightful neurohistologist. Joe Gilbert was a master of providing clinicopathologic insights based upon careful correlation of neuropathologic findings with clinical signs and symptoms (structural brain imaging in the late 1970s was still in its infancy). The experience of working with them both and learning from them was exhilarating, humbling and yes – a little daunting.
Fig 3: Dr. Joseph J. Gilbert, Neuropathology mentor, London, Ontario Joe Gilbert also suggested to me a translational research project that would determine and define my research interest for the coming decades: diseases of the cerebral microvasculature. As a stroke referral center, UWO was encountering many patients with lobar intracerebral hemorrhages caused by, or at least associated with, cerebral amyloid angiopathy (CAA). Joe suggested that we collect our cases of (putative) CAA-related brain hemorrhage and write a descriptive paper on this association; a companion study would assess the topography and severity of CAA in relation to brain aging. In the late 1970s and early 1980s (well before the discovery of beta-amyloid protein in 1984, see below) CAA was evaluated by the use of Congo red staining and polarization microscopy (alternatively using thioflavin stains and fluorescence microscopy). The ‘topography/severity of CAA with age’ study was performed simply by staining a large number of brain sections, from uniformly sampled autopsy brains, with Congo red and evaluating CAA in these. The two resultant manuscripts went through several drafts, were eventually submitted to the journal Stroke as ‘back-to-back papers’, and published in 1983 [5,6]. It is gratifying that the findings we described using fairly primitive (by today’s standards) technology have been replicated using beta-amyloid immunohistochemistry in later studies; it is perhaps especially satisfying that the papers are still being cited 37 years after their publication (combined total citations of 500+ per the Web of Science). Examining the pathogenesis and consequences of CAA and other microangiopathies in the brain would constitute a major theme of my subsequent research endeavours. My NP residency was spent feasting on the instruction and support of my mentors and the remarkable and stimulating milieu created by the clinical Neurologists, Neuroradiologists and Neurosurgeons at UWO. This showed and highlighted the importance of collaborative activities in understanding complex neurologic diseases. Luminaries in Neurology and Neurosurgery (Fred Plum, Raymond Adams among them) were frequent visitors to this small but ‘neurologically important’ city half way between Toronto and Detroit. One of my interests was in the effects on cerebral arteriovenous malformations (AVMs) of agents used in novel embolization therapies that were just being developed, many of them at UWO. Two skilled endovascular specialists (Drs. Fernando Vinuela and Allen Fox) were pioneering new agents and approaches to non-surgical therapies for vascular brain lesions, and continued to do so throughout their careers. When these lesions (usually AVMs) were subsequently resected, they showed unique and sometimes dramatic reactive changes caused by the embolotherapy agents (about which more later…). Many of my research interests have been driven by clinical or clinicopathologic questions. Here were two large and important ones: Why (and how) do embolotherapy agents work through their interactions with vessel walls in vascular malformations? What might be some neuropathologic clues to why they sometimes fail? They were also questions that could be effectively addressed by simple observation (using routine stains) of previously embolized lesions when they made their way to the Surgical Neuropathology laboratory. There was discussion of my returning on faculty to UWO, but only after I had spent some time developing basic research skills pertinent to the study of cerebrovascular disease. The University would provide or facilitate funding for my research endeavours, but I had the freedom to choose a laboratory in which I might develop appropriate experimental techniques and skills that I could repatriate to UWO. At that time, some of the most exciting work on cerebral microvascular biology (especially the blood-brain barrier/ BBB) was being done using cell biologic techniques in the laboratories of Drs. Pasquale (Pat) Cancilla [Figure 4] and Michael N. Hart [Figure 5] at the University of Iowa (U of I) [7,8]. It was arranged that I would spend two years working with them, after a 6-month period refining my diagnostic skills in Pediatric Neuropathology with Dr. Margaret Norman in Vancouver; Marg became and remained a good friend for the rest of her life.
Fig 4: Dr. Pasquale (Pat) and Enid Cancilla, undated photograph Trying my hand at (basic) research I arrived in Iowa City (in which the University of Iowa is located) in January 1982, in the midst of a nasty midwestern blizzard. During a lonely weekend in a slightly seedy motel in Coralville (a suburb of Iowa City) I frequently thought: ‘What on earth have I done?’ During my first day in the new laboratory environment at the U of I, Pat Cancilla asked if I could go with him for a cup of coffee. Then came the bombshell: he had just accepted the Chair of Pathology position at University of California Los Angeles (UCLA). He suggested that, since I had independent funding that was not tied to a specific institution, I might either stay at the U of I and work with Michael Hart, or move with him to UCLA. As I looked outside at the heavy snowfall and felt the subzero temperature en route back to the lab, I had essentially made my decision, and moved with Dr. Cancilla to UCLA that summer. During the six months I resided and worked there, however, I developed an affection for Iowa City, sometimes described as the ‘Athens of the Midwest’—famous for its world class medical center (including brilliant translational neuroscience and behavioral neurology) and the Iowa Writers Workshop. My colleagues there included Drs. Jonathan Fratkin and David Beck, the latter an outstanding Neurosurgeon (then still a resident) bursting with excellent research ideas that might optimize the use of cultured cells in understanding BBB physiology and abnormalities [9].
Fig 5: Dr. Michael Noel Hart UCLA, destined to become my academic home for most of the remainder of my career (though that decision was still in the future), was research heaven for a young scientist. It was fun helping to set up Pat Cancilla’s laboratory (our senior technician at the time was Jim Bready) with top-of-the-line equipment and facilities that were the perks of being a newly recruited Chair and entering the academic milieu of a major research university. Our ‘lab warming’ party was a smash hit throughout the medical center. Pioneering studies of cerebral microvessels (especially the BBB) were ongoing in the laboratories of two ‘Bills’ – William Pardridge and William Oldendorf. Dr. Oldendorf had previously (1975) won the Lasker Award, and probably deserved the Nobel, for suggesting the principles that led to computerized tomographic (CT) scanning, but was also an innovative and creative investigator looking at the physiology of the BBB, especially using isotope tracer techniques. He was also Bill Pardridge’s mentor. Pat Cancilla’s lab became part of an informal consortium of investigators (also including Drs. Judith A. Berliner, an experienced cell biologist, and Eain Cornford at the West LA VA Medical Center) interested in cerebral microvasculature (especially its endothelium) and optimal ways to study it. Our laboratory was mainly intrigued by the potential use of tissue culture approaches and had been able to isolate and culture endothelial and smooth muscle cells from brain microvessels, initially from mouse brains but eventually (some years later) even those derived from human corticectomies for intractable epilepsy. I was also smitten by the city of Angels, Los Angeles. It represented a far different world from the one in which I grew up. L.A. was (and is…) a city with a near perfect climate (summer and winter), far cleaner air than is widely believed, stunning geography with canyons, hills and flatlands, a brilliant seaside location on Santa Monica Bay, and remarkable ethnic and cultural diversity. It reminds itself almost daily that it is the ‘world capital of the entertainment industry’, which is probably true, and ‘the creative center of the planet’ – the latter a claim that London (England), Amsterdam, Tokyo, Paris and a few other cities might dispute. I remember reading that the German novelist Gunther Grass had once described Berlin as representing a city that ‘faced the realities of the 20th century’ (this may be an erroneous recollection…), and thinking that would probably apply quite accurately to L.A. in the late 20th and early 21st centuries. Though I at first lived near the UCLA campus, I found myself spending many weekends at Venice Beach, where I have now had a home for the past 30+ years. (Rationale: If you live near the Pacific Ocean, why not at one of the most famous beaches in the world?) As I was nearing the end of my postdoctoral fellowship, I was working in the lab on a Saturday morning. Pat Cancilla called me into his office (immediately adjacent to the laboratory) and rather directly asked if I might be interested in a UCLA faculty position – one had just come open in Neuropathology because of the retirement of Dr. Jann Brown. We discussed the possibility briefly. This was the second time in my career that a casual chat with Pat Cancilla would alter the course of my career. Return to London, Ontario and UWO (briefly) Because of visa issues and funding, I was committed to return to London, Ontario, but my faculty job there was a ‘soft money’ position, unlike the tenure track post for which I was being considered at UCLA. I had formally applied for the UCLA faculty position while still a postdoc there, interviewed for it, and eventually (a few weeks after returning to London, Ontario) was offered and decided to accept the job. It was a decision made over an agonizing weekend during which I weighed the many pros and cons – the University of Western Ontario would have made a wonderful academic home for me, and London a welcoming and very livable city (I had already bought a home there). John Kaufmann and Joe Gilbert were amazing mentors and colleagues. Yet I had enjoyed my postdoc at UCLA so much… that I felt I had to ‘give it [the faculty position] a try’. Having heard that American academic medicine could be rather brutal and fiercely competitive (though I had seen little evidence of this during my postdoc), I began to wonder whether I had the stomach for this. I rationalized the decision by thinking I would remain at UCLA for 2-3 years, then return to London, Ontario (assuming a position was still open there…). At the appointed time, I considered this move back, and decided to remain at UCLA, where I am (part time, semi-retired) today. My 18 months in London (pending receipt of the green card / permanent resident status that would allow me to take up life in the USA) were delightful and rewarding both professionally and personally – so much so that I began having some doubts as to whether I had made the correct decision in accepting the UCLA job. (Timing is everything. Were I making this same career-changing deliberation in the current unwelcoming USA immigration climate, I would almost certainly have stayed in London!) I managed to set up a small tissue culture laboratory at University Hospital – thanks to the fact that a fully equipped laboratory with appropriate equipment had just been made available by a departing or retiring faculty member. We were able to successfully culture endothelial and smooth muscle cells from human cerebral microvessels [10]. I continued to have an interest in ‘embolized AVMs’. As a result of the neurosurgical skills and expertise of Drs. Charles Drake and Sidney (‘Skip’) Peerless, brilliant endovascular therapy experts Vinuela and Fox (see above) and their respective teams, London and UWO attracted complex AVM cases from around the world that might be candidates for this unique therapy. If one is going to do translational research, it helps to have a unique collection of abundant clinical and pathologic specimens to study – and our Neuropathology laboratory had just such an array of treated AVMs, an amazing experiment of nature, though one admittedly manipulated by physicians. With the help of JCEK and a very industrious undergraduate student (Mark Lundie) I set about a careful examination of AVMs that had been treated by embolization with isobutyl cyanoacrylate, one of the widely used embolotherapy agents at that time. (It is an agent that is injected through a catheter in liquid form, but polymerizes at various rates depending upon how much contrast medium is in the mixture. With this agent, timing of the polymerization process was of paramount importance – if it polymerized too quickly, the catheter could become stuck to the intima of the AVM ‘feeding’ vessel; if too slowly, it would end up passing through the AVM and into a treated patient’s lungs.) We had vascular malformations with a wide range of post-embolization intervals that allowed for inferences about how this polymer was interacting with abnormal vessel walls in AVMs. We put together a significant (and rather unique) data set, which I brought with me to UCLA when I returned there in July, 1985, hoping I would have the time to analyze it in detail and prepare a manuscript.
Fig 6: Dr. Michael A. Farrell, friend, colleague and ‘partner in crime’ I also had the good fortune to meet, during that 1 ½ years back at UWO, Dr. Michael Farrell [Figure 6], a newly arrived Neuropathology trainee from Dublin, Ireland. Michael became a great friend and colleague during that time and after he returned to a consultant post in Dublin. Over the years, we have written many papers (see below) and co-authored a textbook, he has often visited L.A. (even doing a mini-sabbatical in my laboratory during the early 1990s), and I have gone to Dublin dozens of times; it is on my list of favorite cities around the globe. Great and generous friend. Through Michael I eventually came to know the small but vibrant Irish Neuropathology community, including Drs. Katie Keohane and Francesca Brett. On faculty at UCLA How does one summarize 35 years of academic and diagnostic work at one institution? There are many things I love about UCLA: the physical beauty and location of the campus in Westwood (the UCLA Medical Center, now Ronald Reagan UCLA Medical Center, is at the southern edge of the main campus), the collegial and collaborative nature of the faculty, the wealth of expertise in all aspects of basic and clinical science, especially neuroscience, talented and intelligent students and trainees, and the cultural and ethnic diversity of both students and faculty who are committed to scholarly work. Yes, there are things not to like (but one endures them…): the numbing, frequently obstructive bureaucracy, the ‘bend over backwards’ approach to being politically correct are among them. I returned to L.A. and the UCLA family the first week of July, 1985. I used the ‘down time’ in setting up a small research laboratory, to finesse two projects. One was collating the embolized AVM data into a coherent story. As I wrote the manuscript and put the results into perspective, I thought the material was sufficiently novel that it might be worthy of submission to the prestigious New England Journal of Medicine, with the thought that ‘nothing ventured, nothing gained’. As I put the manuscript in the mail (YES, what we now call snail mail...) I was already reformatting the paper for a lower level, less prestigious journal because of the certainty of rejection. Then a few days later I received a surprising phone call from the NEJM telling me the manuscript had been accepted, with minimal revisions; they were calling me to verify that there was no overlap with a review article on cyanoacrylates we had recently written – I assured them there was none [11]. The NEJM paper was published in 1986 [12] and represents one of my two appearances as an author of a paper in this high-profile venue, the second coming almost exactly 20 years later as a co-authored contribution on a totally different topic [13]. My other project was to write a review article on (what else?) CAA – I suggested this to Henry Barnett, then executive editor of Stroke, and he liked the idea. That paper eventually appeared (after a few revisions) in 1987 [14] and is still frequently quoted today. In the meantime, I resumed my tissue culture studies but decided to embark on other scientific adventures. While I was impressed by the simple questions that could be addressed (and answered) using in vitro methods, I was (like many investigators) concerned about how these phenomena could be understood in the context of complex multi-cellular tissues and organs, especially in the brain. Being a junior faculty member at UCLA was the academic equivalent of being a child at a candy store. Colleagues were always approaching one about working on any variety of projects, some utilizing human CNS specimens, others exploiting interesting animal models, transgenic and knockout mice, etc. Neuropathologists were and are in the unique position of understanding the structure of the nervous system (normal and abnormal), and how best to study it. I re-established a close collaboration with William Pardridge (see above), an Endocrinologist in the Dept. of Medicine who was interested in the biochemistry (and eventually molecular biology) of transport mechanisms through the BBB, but was now also looking for a way to study abnormalities (diseases?) of small blood vessels. We had many discussions about cerebral amyloid angiopathy (CAA), which of course affects arterioles and capillaries and, together with arteriolosclerosis, is one of the two most common microvasculopathies found in the brain. In 1984, Glenner and Wong [15] had isolated the ‘A4’ protein from amyloid-laden meningeal vessels of an Alzheimer patient. Bill Pardridge was amazingly skilled at making antibodies and proceeded to make a polyclonal antibody to ‘A4’, using the partial sequence of the peptide provided by Glenner and Wong in their paper. It worked magnificently in immunohistochemical protocols to demonstrate both senile plaques and CAA, resulting in several publications [16,17]. Bill Pardridge was also the best person in the School of Medicine to review the draft of a grant proposal; I am eternally grateful for his merciless critique of one of my first independent National Institutes of Health (NIH) proposals, which through his intervention helped me transform an unfocused and improbable set of studies into a fundable application. My Chief of Neuropathology was M. Anthony Verity, and we divided the service and diagnostic commitments equally – each of us covered 6 months of the year. My interests were obviously in cerebrovascular disease and dementia, Tony’s in neurotoxicology and neuromuscular diseases. When one of our outstanding Neurologists, Dr. Jeffrey Cummings, decided to submit an NIH (National Institute on Aging) grant that, if successful, would fund an Alzheimer Disease Center (ADC) at UCLA in the late 1980s/early 1990s, I seemed the logical choice to head the Neuropathology Core and Brain Bank. We were funded on the first submission and I was thrilled to formally become part of the Alzheimer research enterprise at UCLA, even though my main academic focus (CAA and related microvascular diseases) were at the periphery of most debates on AD pathogenesis. This situation has changed drastically in recent years. It is also worth noting that Glenner and Wong had isolated A4 from amyloid-laden meningeal microvessels (‘a novel cerebrovascular amyloid protein’) rather than senile plaques (SPs); as is now well known, the anti-A4 antibody indeed labels SPs as well as CAA, but not neurofibrillary tangles, despite initial claims that it might. Over the years until his departure from UCLA, Jeff Cummings was an amazing leader: a superb diagnostician and organizer who supported basic research efforts and consistently brought out the strengths in investigators and his staff. And oh yes, he was a masterful fund raiser, successful in obtaining private donations that were crucial to supporting the ADC when NIH funding lapsed or became thin. He eventually secured an endowment that led to re-naming of the ADC as the Mary Easton Alzheimer Center. I had obtained NIH and other funding for my own projects within 3-4 years of arriving at UCLA, but have always felt most at home scientifically in the environment of a collaborative Center or Program Project Grant; pieces of these have constituted most of my research efforts and funding support while on faculty at UCLA. Of course, in the early to mid-1980s other events were taking center stage in the world of medicine: the disease that was eventually named acquired immune deficiency syndrome (AIDS) presented in a handful of gay men, initially studied in New York City and L.A. (Please also see Herbert Budka’s thorough and excellent description of the beginnings of this epidemic in his Reflections piece published earlier this year.) As Pathologists, we were witnessing the evolution of a feared illness that, at the time and for many years to come, had no effective treatment and was almost uniformly fatal. By the mid-1980s it was known to be caused by the retrovirus HIV-1 (initially named HTLV-III). In that same time frame, thanks to the work of many investigators including George Shaw, Beatrice Hahn, Clayton Wiley, Leroy Sharer and others, it became appreciated that HIV frequently infected the brain in both children and adults, causing a syndrome initially described as AIDS dementia complex (in adults) though later re-named several times. But I’m getting ahead of myself… Pathologists have now (and always have had) a key role in providing morphologic evidence for unique disease mechanisms – some of them based simply upon careful observation of novel but convincing histopathologic changes within tissues. Consider, as one example outside the nervous system, the astute observation by Robin Warren (pathologist) and Barry Marshall (gastroenterologist) of ‘unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration’. This description of Helicobacter pylori, initially published in Lancet (in 1984) eventually led to their being awarded the Nobel Prize in 2005 because the observation led to a complete re-examination of the rationale for ways to treat peptic ulcer disease, a major paradigm shift. Moving back into the CNS, Neuropathologists have made countless key observations (often in human biopsy or autopsy specimens) pertinent to the pathogenesis of neurodegenerative disease, intractable epilepsy, stroke, developmental disorders, tumors, and the list goes on. With the beginning of the AIDS epidemic, here was another opportunity to see a new infectious disease evolving before our eyes. This might be (often is…) called ‘opportunistic research’, with the slight implication that it is not as challenging or important as ‘basic research’. However, when unique opportunities to carefully study a human disease present themselves, one would be foolish not to take advantage. At UCLA Center for the Health Sciences (CHS), one of the bright young residents from Canada, Karl Anders [Figure 7], suggested we review the neuropathologic features of our large and growing autopsy collection of brains from AIDS patients. Karl and I, both recent arrivals from Canada, bonded as soon as I arrived at UCLA. We had both grown up in two cities located about 400 miles apart (Karl in Winnipeg), were raised in the households of immigrant families, and we both liked looking at slides – a lot of slides.
Fig 7: Dr. Karl H. Anders, Pathologist and frequent collaborator on projects, currently in Calgary, Alberta, Canada We also engaged in this neuropathologic enterprise the collaboration of Dr. Uwamie Tomiyasu [Figure 8], an amazingly insightful, organized, helpful and collegial Neuropathologist at the West L.A. VA Medical Center (who over the years became a close friend), and involved a promising young UCLA medical student Wayne Guerra in the project. Karl Anders had been the first author on the report of our initial series of AIDS autopsy cases (less than 30) written while I was still a research fellow at UCLA. We had submitted this detailed report to Clinical Neuropathology. The manuscript had been almost immediately accepted for publication in late 1983 or early 1984. Then, to our amazement and shock, Clinical Neuropathology ‘sat on’ this very topical manuscript for over 2 years before publishing it – in the meantime printing (arguably) less impactful and timely studies that had clearly been accepted after our paper [18]. By 1986 we had compiled data on almost 90 AIDS autopsy cases, and submitted this updated report to the American Journal of Pathology, where it was accepted with minimal revisions, and published a few short months after the much delayed Clinical Neuropathology paper [19]. Karl and I wondered whether someone reading both papers (published in 1986) would question how we accumulated 60 new AIDS cases in a few short months, which of course we had not. The neuro-AIDS work took some interesting twists and turns, largely as the result of collaborations with some of my formidably talented colleagues in Virology and Neurology interested in viral neuropathogenesis. I co-authored two papers together with David Ho and his research group while he was briefly on staff at Cedars Sinai Medical Center in Los Angeles [20,21]; these are the only two publications I have written with a physician-scientist who would eventually become Time magazine’s Man/Person of the Year in 1996. (I very much enjoyed basking in the reflected glow of David’s richly deserved fame.) I was also approached by a brilliant and productive retrovirologist, Dr. Irvin S.Y. Chen, who had trained with one of the discoverers of reverse transcriptase (Howard Temin at the University of Wisconsin) before becoming a faculty member at UCLA at about the same time as me. Irvin was (and remains) keenly interested in the molecular pathogenesis of interactions between HIV and the brain. His laboratory used autopsy brain and CSF specimens from neuro-AIDS subjects to characterize a neurotropic strain of HIV, and exploited PCR to quantify HIV viral load in the CNS of affected patients [22,23]. It seemed an ideal collaboration between a talented basic virologist and someone (HVV) interested in morphologic brain changes induced by HIV. At the same time, my laboratory remained fascinated by the interesting opportunistic infections (OIs) – especially other viral agents, that can cause puzzling varieties of devastating neurologic diseases in immunosuppressed AIDS patients. Cytomegalovirus was one of the viral OIs capable of producing variable CNS disease in AIDS, including (at its worst extreme) severe encephalitis, ventriculitis and myeloradiculitis, yet minimal abnormalities in others. Contributors to these studies included Karl Anders, a postdoctoral fellow from Germany, Dr. Regina von Einsiedel and Marcia Cornford, who was one of our first trainees in Neuropathology and is still a faculty member at Harbor-UCLA Medical Center in Torrance, California [24,25]. I became the Pathologist of record for the UCLA site of the Multi-Center AIDS Cohort Study (MACS, PI Dr. Roger Detels), one of the longest funded NIH projects in history. Karl Anders and I co-authored a monograph on the neuropathologic features of AIDS [26].
Fig 8: Dr. Uwamie Tomiyasu, (Dec 2004), former Neuropathologist, West L.A. VA Medical Center and UCLA faculty member, friend By the mid- to late 1980s and into the 1990s there were other interesting developments in UCLA’s active epilepsy surgery programs. It already had a longstanding research effort on temporal lobectomy for intractable temporal lobe seizures, under the capable and inspiring direction of Jerome (‘Pete’) Engel (Neurologist) and Paul Crandall (Neurosurgeon). Pete was, and continues to be, one of the great advocates for bringing the possibility of curative temporal lobe surgery or ‘neocorticectomy’ to epilepsy patients throughout the world. Paul was a meticulous Neurosurgeon who provided us with anatomically intact (including the hippocampus) temporal lobes. The arrival at UCLA of pediatric Neurosurgeon Dr. Warwick Peacock from South Africa in the mid-1980s ushered in a new era of pediatric epilepsy surgery. Using high resolution neuroimaging (including structural and metabolic/positron emission tomographic imaging) modalities linked with electrocorticography, Warwick and the Pediatric Epilepsy group (under the visionary leadership of Drs. Donald Shields and Raman Sankar) developed the concept that generalized epilepsies in infants and children (e.g. leading to infantile spasms) might have a focal origin – a ‘zone of cortical abnormality (ZCA)’ within the cerebral cortex – and that removing such a focus might effectively treat the seizures. At the time, this was considered a radical, almost heretical – possibly even dangerous! – approach, but our clinicians were certain they had convincing evidence for the ZCA and proceeded with corticectomies for intractable infantile and pediatric epilepsy, sometimes removing a significant portion of one cerebral hemisphere in an infant. The challenge for Neuropathologists was to identify what the underlying structural abnormality (abnormalities) causing the seizures might be. Again, we were handed the opportunity to study unique specimens that might explain important clinical signs and symptoms. By the late 1980s and early 1990s we had accumulated a significant experience with these specimens. Fortuitously, my friend and colleague Dr. Michael Farrell came over from Dublin in 1991 to do a mini-sabbatical at UCLA, and set about collating the data on our collection of pediatric epilepsy surgery cases. The most common neuropathologic change (especially among the youngest symptomatic patients) was a malformation of cortical development that had first been described by David Taylor and colleagues in the 1970s. It had a striking resemblance to the tubers found within the brains of patients with tuberous sclerosis complex (TSC) even though affected individuals showed none of the visceral or cutaneous stigmata of this neurocutaneous disorder [27]. Ironically, ‘tuberectomy’ has now become an accepted treatment for some TSC patients with intractable seizures. A much less common finding among corticectomies was an inflammatory disorder first described in 1958, Rasmussen encephalitis (RE). Dr. Farrell was first author on our initial ‘pediatric corticectomy’ paper [28] and we continued to collaborate on other projects, including one aimed at elucidating the detailed neuropathologic changes of RE [29]. Paul Mischel, then a Neuropathology Fellow and now a leading neuro-oncology researcher at UC San Diego, was a lead author on a paper in which we proposed a ‘grading’ scheme for the (as yet poorly understood) condition of cortical dysplasia (CD) [30] – a scheme that served its purpose in the mid-1990s and has been superseded by others, as it should be. The team of clinicians and basic researchers who collaborated in the Pediatric Epilepsy Surgery program was a pleasure to work with. This was team science at its finest – everyone in the group respected (and utilized) the unique skills of all other basic and clinical neuroscientists, and the resulting multi-disciplinary studies benefited from this synergy. Experts in Linguistics, Neuropsychology, Neuroradiology, Neurophysiology and Psychiatry interacted productively with a simple Neuropathologist. Our goal was not only to understand what structural changes in the brain may have contributed to the catastrophic seizure disorder, but how corticectomy might impact a child’s behavior and language development. Dr. Gary Mathern, a UCLA-trained Neurosurgeon and protégé of Paul Crandall and Warwick Peacock, eventually became the surgeon-of-record for most of the pediatric epilepsy cases. Dr. Mathern also has the ‘soul of an investigator’, is possessed of enviable organizational skills and leadership qualities, and fostered new and exciting directions in which the UCLA Pediatric Epilepsy Surgery Program might move, places where it might thrive. Dr. Carlos Cepeda, Michael Levine, (the late) Robin Fisher, Veronique Andre and others became integral to the study of electrophysiological and morphological properties of the epileptogenic tissue originating from infants and children with intractable seizures [31-33]. Dr. Noriko Salamon in Neuroradiology contributed her powerful diagnostic insights and observations [34,35]. In 2006, and based upon our morpho-anatomical and electrophysiologic studies, we proposed the ‘Dysmature cerebral developmental hypothesis’ as a possible etiology for CD [32]. At the same time, we continued to explore the possible relationship of sporadic CD to TSC tubers. The genes that are mutated to cause TSC (first TSC2, then TSC1) had been discovered in the 1990s; we made probes to the relevant gene transcripts and eventually antibodies to the gene products (tuberin and hamartin), using these to study gene expression in normal brain, tubers of TSC and sporadic cortical dysplasia [36-39]. This led to a valuable collaboration with leading TSC researcher Dr. David Kwiatkowski and his associates in Boston – which included sophisticated molecular genetic analysis of many of our corticectomies and even allowed us to examine a novel animal model of TSC, one of the first to be developed by his group [40,41]. I became UCLA’s Chief of Neuropathology in 1993, when Tony Verity decided to take advantage of the University’s ‘voluntary early retirement incentive plan, VERIP’, though thankfully he remained active as an Emeritus faculty for many years, sharing his expertise in neuromuscular diagnosis (Dr. Negar Khanlou became his protégé and successor) and his passion for cricket. Tony was also an excellent artist and I am proud to have one of his paintings on the wall of my living room in Venice. I served in the Chief of Neuropathology post until I myself took ‘semi-retirement’ in 2016, and had the pleasure to mentor junior colleagues who went on to highly successful careers: Cynthia Welsh, Dennis Chute, Jeff Twiss, Paul Mischel among them. Dr. William Yong, my current Chief, was a medical student who I tutored in the 1980s, later a Neuropathology Fellow in our program, and has been a marvelous colleague – alas, recently departed for a position at University of California Irvine Medical Center. For several years, I was honored to hold the Sarkaria Chair in Diagnostic Medicine. In the mid-1990s I was asked by University of Southern California (USC) Neurologist Dr. Helena Chui to become part of a California-wide study she was planning, examining the clinical, neuroimaging and neuropathologic substrates of individuals with documented (or at risk for) cerebrovascular disease. The overarching (and perhaps overly ambitious) theme and goal of the program project grant was to highlight the neurobehavioral, imaging and neuropathologic features of ischemic vascular dementia (IVD), on the assumption that such an entity exists. Helena was an inspiring and superbly organized leader, and an insightful judge of character, the consummate solver of problems. NIH Program project grants (PPGs), including the one that funded this study, involve the interactions of widely differing personalities and the principal investigator of such an endeavor (i.e. Helena Chui) needs to manage those people and their disagreements as well as their productive interactions. Our group involved Neuropsychologists, Epidemiologists, Neurologists, and experts in neuroimaging: Bruce Reed, Dan Mungas, Mike Weiner, Bill Jagust, Ling Zheng, Wendy Mack and many others. My fellow investigators in the Neuropathology Core included William Ellis (UC Davis), Ewa Borys (now in Chicago) and Chris Zarow (then a talented neuroanatomist at USC). Our studies, over the long duration of the IVD-PPG, showed that ‘pure’ IVD was a comparatively rare phenomenon, but that risk factors for cerebrovascular disease probably contribute to accelerated brain aging, and even some components of Alzheimer disease (AD), a view that is gaining traction in the neuroscientific community and a subject that has generated much research interest [42-44]. Two papers from the IVD group focused on the ‘neuropathologic substrates’ of cognitive impairment resulting from ischemic brain lesions [45,46], though crucial neuropathologic data were integrated into many other publications. For several years, I have had an enjoyable collaboration with Dr. Wolff Kirsch, a Neurosurgeon at Loma Linda University Medical Center (approximately 100 miles east of L.A.) who, rather than quietly retire after a stellar career in Neurosurgery, decided to become a researcher with an interest in, among other things, brain aging and cerebral amyloid angiopathy (see Table 1). Dr. Kirsch is devoted to the idea of eventually preventing or treating this microangiopathy and has enlisted materials from the Easton Center Brain Bank in studies with that goal. Very entrepreneurial and creative Neuroscientist and much fun to work with in joint projects. As the above summary indicates, much of my research has been collaborative and translational. Grant reviewing agencies have, I am quite certain, considered it ‘scattershot’ and unfocused. ‘Can Vinters not focus on a single topic?’ – the answer is clearly ‘no’. I’ve enjoyed all of the disparate research endeavours in which I have been involved. They have included interactions with investigators possessed of unique talents and abilities, providing the possibility of forming irresistible, tantalizing scientific alliances. Table 1 summarizes the key individuals with whom I have worked and published most intensely over the years; it is by no means a complete list. My advice to people entering Neuropathology would be to choose your collaborators carefully, wisely. Consider individuals who can bring projects to completion in a timely fashion and make effective use of a Neuropathologist’s unique skill set. Have I myself been successful in following that mandate for timely completion of projects? Well… not always… but often enough. Work with people who will criticize your work and writing, sometimes brutally. I’ve been fortunate to co-author a manuscript with a pharmacologist, Dr. Louis Ignarro, destined to win the 1998 Nobel Prize in Medicine/Physiology for his discovery of nitric oxide [47]. (Disclosure: Dr. Ignarro did not win his Nobel on the basis of our study!) My favorite projects and papers have been those that translated basic science observations to address and inform important clinicopathologic issues – ones that might eventually be used to help patients avoid or recover from devastating neurologic illnesses. In 2009, Dr. Michael Sofroniew in UCLA’s Dept. of Neurobiology approached me with the idea to write a review of basic astrocyte biology (his expertise), and how astrocytic dysfunction might mediate neurologic disease (my interest) [48]. It resulted in my most cited publication and led to further productive collaborations that continue now – studies of astrocyte derangement in certain seizure conditions.
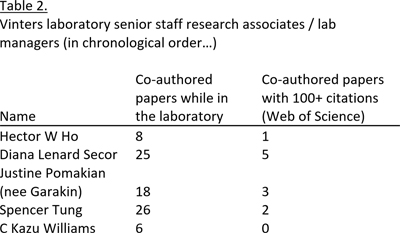
I benefit daily from my colleagues (Drs. William Yong, Shino Magaki, Negar Khanlou), fellows (currently Drs. Zesheng Chen and Josh Byers) and technically super-skilled histotechnologists and staff research associates (e.g. Kazu Williams, current laboratory manager of the Easton Center Brain Bank, Nelly Vehabedian, Jennifer Yi, Cecilia Choi). Part of the group is shown in Figures 9 and 10, masked and ‘social distancing’ (at least in Figure 10) as appropriate for the pandemic. When one of the technical staff contributes significantly to a research project and the resultant publication, I include her/him as a co-author on the manuscript. Table 2 lists key senior research technicians and lab managers who have each co-authored several publications, many of which have been cited 100+ times (per the Web of Science). I take pride that many of these skilled technicians have a publication record that surpasses (in both quantity and quality) those of some junior faculty. Sadly, one of the individuals on that list (Justine Pomakian) passed earlier this year after a long battle with leukemia. Another (Spencer Tung) will graduate this year as a physician. A huge bonus or perk of academic life is the possibility to teach, train and influence others – including medical students, basic science colleagues, graduate students, postdoctoral fellows, residents and clinical fellows. I am especially proud of the many Neuropathology fellows who have graduated from the UCLA training program and have gone out to initiate clinical and/or research programs of their own. Our goal as teachers and mentors should be to foster the creation of individuals who are better than we are – more creative, more energetic, better and more insightful diagnosticians. I flatter myself to think that overseas visitors who spent significant time at UCLA Neuropathology – Drs. Sung Hye Park from Korea, Remco Natte from the Netherlands, Orestes Solis from the Philippines, Hajime Miyata from Japan, Regina von Einsiedel from Germany, many others – brought back to their home countries skills and knowledge gained in Los Angeles in UCLA’s laboratory of Neuropathology.
Fig 9: Team Neuropathology at UCLA, 2020 (briefly suspending social distancing rules during the COVID 19 epidemic) The joy of scientific meetings, sabatticals, visiting professorships and academic visits Academics can be fun, terrific fun! Most of us enjoy scientific meetings – well, used to enjoy them before they devolved into sitting in front of a computer screen, asking ‘Should I share my screen? UNMUTE yourself… Can everyone hear me? Interesting living room décor, or is it an artificial background? OH NO, black screen again’, etc. I have a nagging fear that the trainees of today will come to think: This really isn’t so bad! Perhaps it is acceptable as a temporary substitute, but of course there is nothing to compare with the give and take of in person conferences, the body language and passion that are evident in heated or even subdued scientific debates, the stimulating discussions – and yes, gossip! – that occur over cocktails and meals. I recall an American Association of Neuropathologists meeting (in the early days of my career) during which two senior prominent academics who both worked on neurodegenerative diseases (names withheld to protect the guilty… though alas, both are now deceased…) almost came to blows in front of a poster focusing on the pathogenesis and significance of senile plaques. A little embarrassing, but also somewhat gratifying that each should care so completely and enthusiastically about the significance of these tiny (though controversial) brain lesions – whose importance and relevance to Alzheimer’s disease are still debated today.
Fig 10: Team Neuropathology at UCLA, practicing social distancing What would academic life be without sabbaticals? I spent a marvelous year in the early 1990s with Dr. Clayton A. Wiley at UC San Diego, learning the basics of molecular biology and diagnostics as applied to human brain specimens, especially those originating from corticectomies for intractable seizures [49]. I had the opportunity to work with an outstanding technician, Rebecca Wang (who sadly died of metastatic melanoma a few years later) and Dr. Cris Achim, who remains a friend and collaborator while now on faculty at UCSD. In 1993, I was kindly and generously funded by the DAAD (German Academic Exchange Service) to work for several weeks with Heiko and Eva Braak in Frankfurt – learning how elegant neuroanatomic methods that they had perfected could provide insights into Alzheimer’s disease.
I’ve had the opportunity to speak and study in countries I would probably not have visited, save for an invitation to lecture or work there – usually at the expense of the host nation/city/academic institution, for which generosity I am sincerely grateful. I’ve even given a lecture in Riga, Latvia (2015) and was interviewed in Latvian (of course I speak the language, in fact English is my second language) on their national radio network. In 1997 (for 6 months) and later in 2004 (for a shorter time interval), I had the chance to do research and teaching as a Visiting Professor (‘Hoogleraar’) at the Leiden University Medical Center, located in an historic city that is home to an equally ancient and revered university – what might be described as a college town in the USA. Leiden is situated between Amsterdam and The Hauge (closer to the latter) in the Netherlands and is a short bicycle ride to Katwijk on the North Sea coast. I shared an office, and many stimulating discussions (about neuropathology, politics, the Dutch royal family and other non-scientific matters) with Dr. Marion Maat-Schieman [Figure 11]. I had the privilege to study, in great detail and with Marion’s assistance and much input from Dr. Remco Natte (now a successful Pathologist in Holland), the fascinating and unique Dutch form of hereditary cerebral amyloid angiopathy that results from a distinctive APP codon 693 mutation. This causes perhaps the purest form of vascular dementia resulting from microvascular disease, at least beta-amyloid CAA [50]. Remco later spent several productive months performing complex tissue culture experiments (using vascular-derived smooth muscle cells) in my lab at UCLA. In 1998, Burroughs Wellcome generously provided me with funds to work for a month with Dr. Michael Farrell at the Beaumont Hospital in Dublin. For several years in the early 2010s, I had the privilege to travel to Manila in the Philippines to lecture at the University of Santo Tomas and several national and international meetings held in that fascinating country. Manila itself is full of paradoxes – great wealth and grinding poverty among them, sometimes existing in close physical proximity – and is one of the most welcoming and hospitable nations in the world.
Fig 11: Dr. Marion Maat-Schieman, retired Neuropathologist, Leiden University Medical Center, the Netherlands I am proud to be both Canadian and American, hold two passports and even have a home in Vancouver, Canada – which I hope to see again some day after the COVID19-related Canadian/USA travel restrictions are lifted or at least decreased. For several summers from 2013-2017, I spent a 1-2 week micro-sabbatical in Vancouver, working with Dr. Ian Mackenzie and his associates at the Vancouver Hospital, refining my diagnostic skills in the area of frontotemporal dementia and lobar degenerations, enjoying this almost impossibly beautiful city, and Ian’s amazing knowledge of this complex group of disorders. One of the great tragic consequences of COVID 19 is the impact it has had on international travel. Joining in the life of the university UCLA Medical Center (for many years now the Ronald Reagan UCLA Medical Center/ RRUMC) is located at the southern part of the larger UCLA campus. Unlike many metropolitan medical centers, it is thus closely linked not only to the non-medical scientific departments with which we interact (including most notably Chemistry and Biochemistry, Biomedical Engineering) but also the arts and humanities. While I have been at UCLA, two faculty members in the Department of Chemistry/Biochemistry (Donald Cram and Paul Boyer) have been awarded Nobel Prizes; excellent resource to have when one is contemplating experiments with a biochemical component. Since arriving at UCLA as a junior faculty member, I’ve taken advantage of this proximity, having served for several years on the campus-wide Graduate Council and, more recently, the university’s Council on Academic Personnel (CAP). CAP is a committee of 12-15 senior faculty members representing all (most) segments of UCLA, who review the dossiers of other UCLA academic faculty for initial appointment, major academic promotions (e.g. to the rank of Distinguished Professor) or appointment to an endowed Chair. Serving on CAP provided a remarkable overview of the diversity of talent and skills at the university. It also gave an interesting perspective into the heterogeneous activities that qualify as creative accomplishment in UCLA Departments such as Near Eastern Languages and Culture, English, Philosophy and Digital Media, to name four among many. Life does not end with retirement – nor should it… and closing comments I formally retired from my full time equivalent (FTE) in July 2016, and have been on ‘recall’ for clinical and academic work since then, continuing to the present time. For some unknown reason, UCLA allows recall faculty to work 43% of time (??!!), though I probably spend more time than that in my office and lab. In 2017, I was honored by the British Neuropathological Society with the Alfred Meyer Medal and Lectureship, received and delivered in London; the British surely are the masters at doing this sort of festive event, and I was suitably ‘chuffed’ and grateful for the honor. That same year I received the award for Meritorious Contributions to Neuropathology, from the American Association of Neuropathologists. Agreed – awards are not that important, but they are a lovely symbol of regard from one’s colleagues. Over many years, I have established the Gunnar Vinters bursary at Lakehead University in my home town of Thunder Bay. Last year, I also endowed the Elise and Arnold Vinters scholarship, in memory of my grandparents, at the Northern Ontario Medical School in the same university. I enjoy building on the endowment for each academic award, annually and encouraging others to contribute. Since 2018 I have been doing locum work at the University of Alberta, in a unit known as Alberta Precision Laboratories (APL). My wonderful colleagues there are Drs. Laura Schmitt, Frank van Landeghem and Sumit Das [Figure 12]. The work is currently on hiatus (since February, 2020), pending resumption of travel between Canada and the USA, but I hope that happens soon. I recently co-authored my first paper with colleagues at APL [51]. It is a form of coming full circle, since I interned at the old University of Alberta Hospital in 1976-77.
Fig 12: My Neuropathology colleagues at Alberta Precision Laboratories, Edmonton, Alberta, 2020 (L to R Drs. Laura Schmitt, Frank van Landeghem, Sumit Das) I love travel, including (and especially) air travel… but as of this writing have not been on an airplane or near an airport for 5+ months. However, there is much still to do at UCLA, projects that – so I hope – benefit from my input, complex cases on which I can shed some light. In my spare time, I revel in the delights of Venice Beach, California, where there is – shall we say – never a dull moment. It is a beachside region of Los Angeles founded in the early 1900s by Abbot Kinney, a tobacco heir who was so impressed with Venice, Italy, that he thought it would be fun to replicate it in southern California. I have great friends there, throughout L.A. and in Canada and five accomplished Godchildren whose antics keep life interesting. In my spare time, which seems sometimes not to be terribly abundant, I write short stories and OPED pieces, none of which is destined for publication, though I’ve published a few ‘back in the day’. Now it is time to end this reflection, which seems to have expanded to the length of a novella! When I was in medical school, I never dreamed I would spend most of my adult life in southern California. As I heard or read somewhere, ‘Life is what happens to you while you are making plans…’ – how true. I appreciate Free Neuropathology giving me the opportunity to write this piece. Acknowledgements Kazu Williams assisted with preparation of figures. Dr. Shino Magaki and Kazu Williams assisted with critical reading of the manuscript. References 1. Vinters H, Dainty J, Tyree MT. Cell-wall elastic properties of Chara corallina. Canadian Journal of Botany. 1977; 55: 1933-1939 2. Seeman P. Membrane actions of anesthetics and tranquilizers. Pharmacological Reviews. 1972; 24: 583-655 3. Hornykiewicz O. Dopamine (3-hydroxytyramine) and brain function. Pharmacological Reviews. 1966; 18: 925-964 4. Steele JC, Richardson JC, Olszewski J. Progressive supranuclear palsy. A heterogeneous degeneration involving the brain stem, basal ganglia and cerebellum with vertical gaze and pseudobulbar palsy, nuchal dystonia and dementia. Archives of Neurology. 1964; 10: 333-359 5. Gilbert JJ, Vinters HV. Cerebral amyloid angiopathy—incidence and complications in the aging brain. 1. Cerebral hemorrhage. Stroke. 1983; 14: 915-923 6. Vinters HV, Gilbert GG. Cerebral amyloid angiopathy—incidence and complications in the aging brain. 2. The distribution of amyloid vascular changes. Stroke. 1983; 14: 924-934 7. DeBault LE, Cancilla PA. Gamma-glutamyl transpeptidase in isolated brain endothelial cells: Induction by glial cells in vitro. Science. 1980; 207:653-655 8. DeBault LE, Cancilla PA. Induction of gamma-glutamyl transpeptidase in Isolated cerebral endothelial cells. Advances in Experimental Medicine Biology. 1980; 131: 79-88 9. Beck DW, Vinters HV, Hart MN, Cancilla PA. Glial cells influence polarity of the blood-brain barrier. Journal of Neuropathology & Experimental Neurology. 1984; 43: 219-214 10. Vinters HV, Reave S, Costello P, Girvin JP, Moore SA. Isolation and culture of cells derived from human cerebral microvessels. Cell Tissue Research. 1987; 249: 657-667 11. Vinters HV, Galil KA, Lundie MJ, Kaufmann JCE. The histotoxicity of Cyanoacrylates. A selective review. Neuroradiology. 1985; 27: 279-291 12. Vinters HV, Lundie MJ, Kaufmann JCE. Long-term pathological follow-up of Cerebral arteriovenous malformations treated by embolization with bucrylate. New England Journal of Medicine. 1986; 314: 477-483 13. Small GW, Kepe V, Ercoli LM, Prabha S, Bookheimer SY, Miller KJ, Lavretsky H, Burggren AC, Cole GM, Vinters HV, Thompson PM, Huang S-C, Satyamurthy N, Phelps ME, Barrio JR. PET of brain amyloid and tau in mild cognitive impairment. New England Journal of Medicine 2006; 355: 2652-2663 14. Vinters HV. Cerebral amyloid angiopathy. A critical review. Stroke 1987; 18: 311-324 15. Glenner GG, Wong CW. Alzheimer’s disease: Initial report of the purification and characterization of a novel cerebrovascular amyloid protein. Biochemical and Biophysical Research Communications 1984; 120: 885-890 16. Vinters HV, Pardridge WM, Yang J. Immunohistochemical study of cerebral amyloid angiopathy: use of an antiserum to a synthetic 28-amino-acid peptide fragment of the Alzheimer’s disease amyloid precursor. Human Pathology 1988; 19: 214-222 17. Vinters HV, Nishimura GS, Secor DL, Pardridge WM. Immunoreactive A4 and gamma-trace peptide colocalization in amyloidotic arteriolar lesions in brains of patients with Alzheimer’s disease. American Journal of Pathology 1990; 137: 233-240 18. Anders K, Steinsapir KD, Iverson DJ, Glasgow BJ, Layfield LJ, Brown WJ, Cancilla PA, Verity MA, Vinters HV. Neuropathologic findings in the acquired immunodeficiency syndrome (AIDS). Clinical Neuropathology 1986; 5: 1-20 19. Anders KH, Guerra WF, Tomiyasu U, Verity MA, Vinters HV. The neuropathology of AIDS. UCLA experience and review. American Journal of Pathology 1986; 124: 537-558 20. Li XL, Moudgil T, Vinters HV, Ho DD. CD4-independent, productive infection of a neuronal cell line by human immunodeficiency virus type 1. Journal of Virology 1990; 64: 1383-1387 21. Ho DD, Bredesen DE, Vinters HV, Daar ES. The acquired immunodeficiency syndrome (AIDS) dementia complex. Annals of Internal Medicine 1989; 111: 400-410 22. Koyanagi Y, Miles S, Mitsuyasu RT, Merrill JE, Vinters HV, Chen ISY. Dual infection by of the central nervous system by AIDS viruses with distinct cellular tropisms. Science 1987; 236: 819-822 23. Pang S, Koyanagi Y, Miles S, Wiley C, Vinters HV, Chen ISY. High levels of unintegrated HIV-1 DNA in brain tissue of AIDS dementia patients. Nature 1990; 343: 85-89 24. Vinters HV, Kwok MK, Ho HW, Anders KH, Tomiyasu U, Wolfson WL, Robert F. Cytomegalovirus in the nervous system of patients with acquired immune deficiency syndrome. Brain 1989; 112 (Pt 1): 245-268 25. Von Einsiedel RW, Fife TD, Aksamit AJ, Cornford ME, Secor DL, Tomiyasu U, Itabashi HH, Vinters HV. Progressive multifocal leukoencephalopathy in AIDS. A clinicopathological study and review of the literature. Journal of Neurology 1993; 240: 391-406 26. Vinters HV, Anders KH. Neuropathology of AIDS. Boca Raton, Florida: CRC Press, 1990; 229 pp 27. Taylor DC, Falconer MA, Bruton CJ, Corsellis JA. Focal dysplasia of the cerebral cortex in epilepsy. Journal of Neurology, Neurosurgery and Psychiatry 1971; 34: 369-387 28. Farrell MA, DeRosa MJ, Curran JG, Secor DL, Cornford ME, Comair YG, Peacock WJ, Shields WD, Vinters HV. Neuropathologic findings in cortical resections (including hemispherectomies) for the treatment of intractable childhood epilepsy. Acta Neuropathologica 1992; 83: 246-259 29. Farrell MA, Droogan O, Secor DL, Poukens V, Quinn B, Vinters HV. Chronic encephalitis associated with epilepsy. Immunohistochemical and ultrastructural studies. Acta Neuropathologica 1995; 89: 313-321 30. Mischel PS, Nguyen LP, Vinters HV. Cerebral cortical dysplasia associated with pediatric epilepsy. Review of neuropathologic features and proposal for a grading system. Journal of Neuropathology and Experimental Neurology 1995; 54:137-153 31. Cepeda C, Hurst RS, Flores-Hernandez J, Hernandez-Echeagaray E, Klapstein GJ, Boylan MK, Calvert CR, Jocoy EL, et al. Morphological and electrophysiological characterization of abnormal cell types in pediatric cortical dysplasia. Journal of Neuroscience Research 2003; 72: 472-486 32. Cepeda C, Andre VM, Levine MS, Salamon N, Miyata H, Vinters HV, Mathern GW. Epileptogenesis in pediatric cortical dysplasia: The dysmature cerebral developmental hypothesis. Epilepsy & Behavior 2006; 219-235 33. Cepeda C, Chen JY, Wu JY, Fisher RS, Vinters HV, Mathern GW, Levine MS. Pacemaker GABA synaptic activity may contribute to network synchronization in pediatric cortical dysplasia. Neurobiology of Disease 2014; 62: 208-217 34. Chandra PS, Salamon N, Nguyen ST, Chang JW, Huynh MN, Cepeda C, Leite JP, Neder L, Koh S, Vinters HV, et al. Infantile spasm-associated microencephaly in tuberous sclerosis complex and cortical dysplasia. Neurology 2007; 438-445 35. Salamon N, Andres M, Chute DJ, Nguyen ST, Chang JW, Huynh MN, Chandra PS, Andre VM, Cepeda C, Levine MS, et al. Contralateral hemimicrencephaly and clinical-pathological correlations in children with hemimegalencephaly. Brain 2006; 129: 352-365 (Part 2) 36. Menchine M, Emelin JK, Mischel PS, Haag TA, Norman MG, Pepkowitz SH, Welsh CT, Townsend JT, Vinters HV. Tissue and cell-type specific expression of the tuberous sclerosis gene, TSC2, in human tissues. Modern Pathology 1996; 1071-1080 37. Vinters HV, Park SH, Johnson MW, Mischel PS, Catania M, Kerfoot C. C. Cortical dysplasia, genetic abnormalities and neurocutaneous syndromes. Developmental Neuroscience 1999; 21 (3-5): 248-259 38. Johnson MW, Miyata H, Vinters HV. Ezrin and moesin expression within the developing human cerebrum and tuberous sclerosis-associated cortical tubers. Acta Neuropathologica 2002; 104: 188-196 39. Johnson MW, Emelin JK, Park SH, Vinters HV. Co-localization of TSC1 and TSC2 gene products in tubers of patients with tuberous sclerosis. Brain Pathology 1999; 9: 45-54 40. Qin W, Chan JA, Vinters HV, Mathern GW, Franz DN, Taillon BE, Bouffard P, Kwiatkowski DJ. Analysis of TSC cortical tubers by deep sequencing of TSC1, TSC2 and KRAS demonstrates that small second-hit mutations in these genes are rare events. Brain Pathology 2010; 20: 1096-1105 41. Goto J, Talos DM, Klein P, Qin W, Chekaluk YI, Anderl S, Malinowska IA, Di Nardo A, et al. Regulable neural progenitor-specific Tsc1 loss yields giant cells with organellar dysfunction in a model of tuberous sclerosis complex. Proceedings of the National Academy of Sciences of the USA 2011; 108: E1070-E1079 42. Reed BR, Mungas DM, Kramer JH, Ellis W, Vinters HV, Zarow C, Jagust WJ, Chui HC. Profiles of neuropsychological impairment in autopsy-defined Alzheimer’s disease and cerebrovascular disease. Brain 2007; 130 (Pt 3): 731-739 43. Jagust WJ, Zheng L, Harvey DJ, Mack WJ, Vinters HV, Weiner MW, Ellis WG, Zarow C, Mungas D, Reed BR, et al. Neuropathological basis of magnetic resonance images in aging and dementia. Annals of Neurology 2008; 63: 72-80 44. Chui HC, Zarow C, Mack WJ, Ellis WG, Zheng L, Jagust WJ, Mungas D, Reed BR, Kramer JH, DeCarli CC, et al. Cognitive impact of subcortical vascular and Alzheimer’s disease pathology. Annals of Neurology 2006; 60: 677-687 45. Vinters HV, Ellis WG, Zarow C, Zaias BW, Jagust WJ, Mack WJ, Chui HC. Neuropathologic substrates of ischemic vascular dementia. Journal of Neuropathology and Experimental Neurology 2000; 59: 931-945 46. Vinters HV, Zarow C, Borys E, Whitman JD, Tung S, Ellis WG, Zheng L, Chui HC. Review: Vascular dementia: Clinicopathologic and genetic considerations. Neuropathology and Applied Neurobiology 2018; 44: 247-266 47. Mitrovic B, Ignarro LJ, Vinters HV, Akers MA, Schmid J, Uittenbogaart C, Merrill JE. Nitric oxide induces necrotic but not apoptotic cell death in Oligodendrocytes. Neuroscience 1995; 65: 531-539 48. Sofroniew MV, Vinters HV. Astrocytes: Biology and pathology. Acta Neuropathologica 2010; 119: 7-35 49. Vinters HV, Wang R, Wiley CA. Herpesviruses in chronic encephalitis associated with intractable childhood epilepsy. Human Pathology 1993; 24: 871-879 50. Vinters HV, Natte R, Maat-Schieman MLC, van Duinen SG, Hegeman-Kleinn I, Welling-Graafland C, Haan J, Roos RAC. Secondary microvascular degeneration in amyloid angiopathy of patients with hereditary cerebral hemorrhage with amyloidosis, Dutch type (HCHWA-D). Acta Neuropathologica 1998; 95: 235-244 51. Chan J, Magaki S, Zhang XR, Chin C, Greenspan S, Linetsky M, Kattar M, Vinters HV. Intravascular carcinomatosis of the brain: a report of two cases. Brain Tumor Pathology 2020; 37: 118-125
Copyright: © 2020 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |