|
|
|
Free Neuropathology 1:10 (2020) |
|
Review |
|
Top ten discoveries of the year: Neurotrauma |
|
Daniel P. Perl |
|
J. Edward Hebert School of Medicine, “America’s Medical School”, Uniformed Services University, Bethesda, MD, USA |
|
Corresponding author: |
|
Submitted: 12 February 2020 Accepted: 22 March 2020 Copyedited by: Nicole Schwab Published: 30 March 2020 |
|
Keywords: Neurotrauma, TBI, Chronic traumatic encephalopathy, CTE, Tau, MRI, PET, Cryo-EM |
|
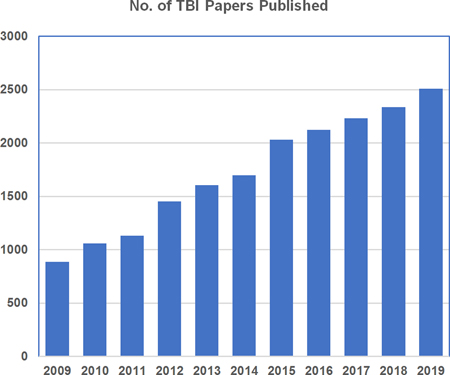
Abstract Neurotrauma represents a major public health problem and is one of the leading causes of death and disability worldwide. Despite its high prevalence, there are major gaps in our understanding of the underlying pathophysiology leading to the substantial morbidity and mortality associated with this problem. Here, ten studies published in 2019 are reviewed that addressed issues related to the acute and long-term effects of neurotrauma. These studies can be broken down into three separate categories, namely, the importance of neurotrauma-based damage to the cerebrovascular unit, white matter damage following neurotrauma, and research related to the long-term neurodegenerative consequences of repeated head trauma, especially chronic traumatic encephalopathy. The advances highlighted here indicate that progress has been made. However, major gaps in knowledge remain which will require additional neuropathologic studies of clinical specimens, as well as the development and investigation of a wide range of relevant pre-clinical models. Further efforts in this field are clearly needed if there are to emerge better clinical outcomes for the numerous patients that suffer neurotrauma each year as well as those currently suffering from its long-term effects. Abbreviations CHIMERA - Closed-Head Impact Model of Engineered Rotational Acceleration, cryo-EM - cryo electron microscopy, CRASH - Clinical Randomisation of an Antifibrinolytic in Significant Haemorrhage, CT - computerized tomography, CTE - chronic traumatic encephalopathy, GCS - Glasgow Coma Scale, GFAP - glial fibrillary acidic protein, MRI - magnetic resonance imaging, mTBI - mild traumatic brain injury, NFL - National Football League, PET - positron emission tomography, TBI - traumatic brain injury, WT - wild type. Introduction According to PubMed, in 2019 there appeared 2,508 publications which included traumatic brain injury (TBI) as a keyword. This compares to 886 papers with TBI as a keyword published in 2009. Each year, over the past decade, there has been a steady increase in publications, addressing this topic (see figure 1). This almost three-fold increase in published reports over the past decade reflects, I believe, increasing awareness of the importance of the health issues related to neurotrauma, opportunities for neurotrauma research, as well as increased funding for research on the topic. However, as will be pointed out, despite this increased research attention, there is much more to be done.
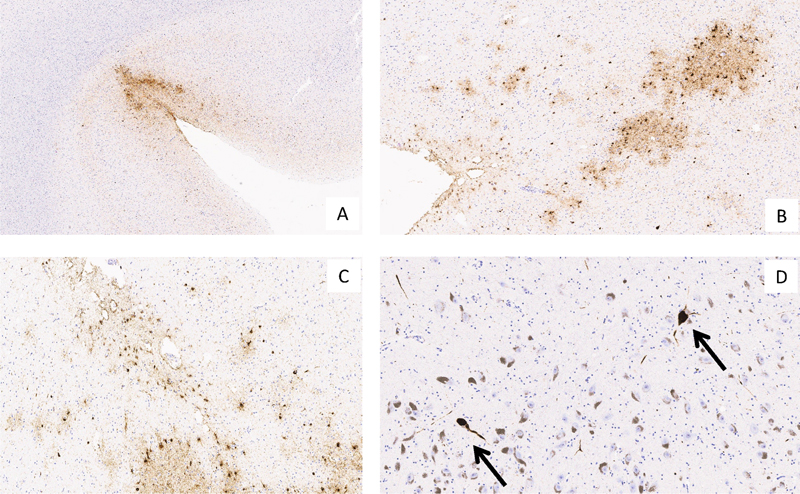
Figure 1: No. of TBI Papers Published (source: www.ncbi.nlm.nih.gov/pubmed) According to the Centers for Disease Control and Prevention, in the United States, in 2014 there were 2.87 million TBI-related emergency room admissions, 288,000 hospital admissions and 56,800 deaths (155 per day) (see www.cdc.gov/traumaticbraininjury). That number of annual deaths is greater than occurs each year related to other, more widely recognized, health issues such as breast cancer (42,170 deaths, data from the American Cancer Society), colon and rectal cancer (53,200 deaths, data from the American Cancer Society), pancreatic cancer (47,050 deaths, data from the American Cancer Society) and influenza (51,376 deaths, data from 2014-15 from the CDC) (see www.cancer.org and www.cdc.gov/flu as sources of data on death rates). A further reason for increasing attention to neurotrauma has been concerns about the long-term effects of TBI on the brain and the possible link to the subsequent development of neurodegenerative disorders. There has also been increasing interest among the US Department of Defense and Veterans Administration in both the acute and the long-term effects of impact and blast TBI among the more than 2 million military service members who have been deployed to the Middle East to fight the war against terrorism. Finally, there has been particular concern about the long-term effects of participation in contact sports, such as American football, with the occurrence of repeated concussive and subconcussive impact TBIs and a risk of developing chronic traumatic encephalopathy (CTE). All of this has combined to promote increasing attention to neurotrauma research. Obviously I was not able to review all 2,508 papers appearing in the past year in making my selections of the most important contributions to this field. I readily admit that there is a degree of personal bias to those I have chosen, however, the following is a list of what I consider to be the most influential papers to have appeared in the past year, plus comments on how I believe they have influenced both clinical and pre-clinical concepts. Role of the Vasculature in TBI Pathophysiology In 2019, there have been several reports that highlighted the importance of the cerebrovascular unit in the pathophysiology of TBI. In 2019, this was emphasized by the positive results of a very large clinical trial (CRASH 2019), the use of magnetic resonance imaging (MRI) and subsequent neuropathology correlation in TBI patients (Griffin, Turtzo et al. 2019) and a pre-clinical model of sub-concussive blast exposure in the rat (Gama Sosa, De Gasperi et al. 2019). Over the past several years, unfortunately, there have been a large number of failed clinical trials seeking to improve outcomes of acute victims of TBI. However, in 2019, a randomized placebo-controlled clinical trial on the effects of treatment by tranexamic acid on death and disability in patients with acute TBI (CRASH 2019) was successful. The rationale for this approach is that tranexamic acid reduces bleeding by inhibiting the enzymatic breakdown of fibrin blood clots. Fibrinolysis, with increased concentrations of fibrinogen degradation products, is commonly seen in the brains of acute TBI patients and predicts the development of further intracranial hemorrhagic expansion (Zhang, He et al. 2018). The report involved an extremely large trial, consisting of a total of 12,737 hospitalized patients with acute TBI. Enrollment criteria included adults with TBI who were within 3 hours of injury, had a Glasgow Coma Scale (GCS) of 12 or lower or showed evidence of intracranial bleeding on CT examination. The study clearly demonstrated that administration of tranexamic acid within 3 hours of head injury significantly reduced the risk of death. The authors stressed that early treatment was essential to elicit this effect and that patients with a GCS score of 3 or less or who had non-reactive pupils at baseline failed to show a reduction in death-rate. In the tranexamic acid-treated group, excluding patients with a GCS of 3 or with bilateral unreactive pupils at baseline, the risk of head-injury-related death was 12.5% versus 14.9% in the placebo group (485 vs 525 events; RR 0·89 [95% CI 0·80–1·00]). In addition, their study demonstrated that tranexamic acid administration in the TBI patients had a very good safety record. The risks of serious vascular occlusive events (deep vein thrombosis, pulmonary embolism, stroke or myocardial infarction) or of seizures were not increased in the tranexamic treated patients when compared to the placebo group. Importantly, tranexamic acid is a widely available drug which is quite inexpensive. Indeed, the total cost of this medication, as given in the trial, was less than $10/patient! TBI is not just a problem in rich industrialized countries, but is seen worldwide, especially in developing countries. TBI is a leading cause of death and disability worldwide, with an estimated 10,000,000 cases being hospitalized or dying each year (Roberts, Belli et al. 2018). The low cost and demonstrated safety of this treatment makes it ideal for use throughout the world and, according to the authors, promises a dramatic impact on the survival of large numbers of patients. This important paper reports what I believe is the first clinical drug trial to ever show significantly reduced mortality from TBI. It is promising for changing clinical practice and saving numerous lives, worldwide. For neuropathologists, this paper emphasizes the importance of bleeding and vascular ischemic lesions as important factors leading to fatal outcomes following head trauma. These aspects have been poorly documented and understood in the neuropathology literature and will require further investigation, both in a clinical setting and in pre-clinical models. An example of this approach is my next chosen publication which involves MRI and correlative neuropathology in the evaluation of acute TBI patients (Griffin, Turtzo et al. 2019). Full disclosure requires that I identify myself as a participant in, and an author of this study which reports on the identification and characterization of microbleeds in the work-up of acute patients with TBI (Griffin, Turtzo et al. 2019). Nevertheless, the results reported are sufficiently important to include it on my list of important contributions to the field of neurotrauma. Within the initial clinical workup of patients coming into an emergency department following TBI is the use of CT examination looking for evidence of major sites of intracranial bleeding that might require surgical intervention. Some research groups have now begun to employ MRI imaging as a means of providing the more detailed morphologic spatial resolution inherent to this technology to the information available for acute TBI clinical management. In doing so, it has been noted that the brains of many TBI patients being evaluated in this way show the presence of multiple small, often punctate or linear hypointensities on T2-weighted imaging (Huang, Kuo et al. 2015, Chiara Ricciardi, Bokkers et al. 2017). MRI lacks a cellular level of resolution leading to conjecture as to what the underlying pathology of these lesions might represent. Some have interpreted them to be traumatic microbleeds, while others have suggested them to represent the sites of hemorrhagic axonal injuries. Importantly, whether such MRI findings may be used as a biomarker for predicting successful, partial, or poor recovery remains an unanswered question. The data in this study (Griffin, Turtzo et al. 2019) is from a large number of civilian TBI victims who were clinically evaluated in several urban trauma centers in the Washington, DC area. Eligible patients were entered into an MRI screening protocol along with further longitudinal clinical follow-up. A total of 439 patients met inclusion criteria for the initial neuroradiologic analysis. Most of those enrolled were determined to have mTBI (83%), with a mean GCS at the time of initial evaluation of 15. Importantly, approximately one-third of these mild patients showed evidence of punctate and/or linear microbleeds on initial MRI exam, indicating that such lesions are not uncommon following mild and mostly asymptomatic head trauma. The presence of traumatic microbleeds was shown to be an independent predictor of subsequent disability in the cohort (P >0.05; odds ratio = 2.5). One of the patients who had received MRI within 48 hours of injury and showed the presence of multiple punctate and linear intraparenchymal hemorrhages, died 7 months following the accident and was subjected to post-mortem examination with brain donation for use in research. Using the clinical MRI exams, supplemented by ex vivo imaging of the formalin fixed brain specimen, a correlational neuroimaging/neuropathology investigation was performed on the specimen in an attempt to identify the histopathologic nature of the punctate/linear hemorrhages that had been identified. Using co-registration of the clinical and ex vivo MRI images with histopathologic stained sections, the post-traumatic microhemorrhages showed the presence of iron-laden macrophages, predominantly within perivascular spaces. In these colocalized histopathologic slides, evidence of axonal injury was not observed in conjunction with the microhemorrhages. This study highlights the importance of damage to the cerebral vasculature as a consequence of mTBI and its effect on clinical outcome. This result, combined with the findings of the previously discussed paper on the effectiveness of tranexamic acid, underscores the importance of studying the effects of TBI on the integrity of the cerebrovasculature unit. We are far from knowing how best to use such MRI findings for a more rational therapeutic approach to patients. However, additional correlational neuroimaging / neuropathology studies of this type will clearly lead to important information that will, in the future, refine clinical diagnostic and treatment guidelines. In a further investigation of the role of the cerebrovascular unit in the pathophysiology of TBI, Gama-Sosa and colleagues reported findings in a pre-clinical rat model of repetitive mild blast TBI (Gama Sosa, De Gasperi et al. 2019). Using a blast tube facility, the dose of blast exposure to the rats was mild and determined to represent 74.5 kPa (equivalent to 10.8 psi) and animals were exposed to one blast per day, over three consecutive days. Exposed rats were sacrificed at 6 weeks, 8 months and 10 months following blast exposure. This model was considered to be a low level of blast exposure, comparable to those endured by military Service Members in training activities and combat exercises (thus emphasizing the clinical relevance of this model), and exposed animals failed to show evidence of generalized neuronal pathology at either the light or electron microscopic level. However, upon detailed examination of the neurovascular unit, significant pathology was identified. Using purified vascular fractions, decreased levels of vascular-associated glial fibrillary acidic protein (GFAP) and that of several neuronal intermediate filament proteins (α-internexin and low, middle and high neurofilament proteins) were identified 6 weeks following the blast exposure. Electron microscopy showed evidence of damage to astrocytic end-feet associated with blood vessels. At 8 months following blast exposure, there was evidence of alterations of the vascular smooth muscle layer. These findings indicate that despite the low dose of blast exposure, significant chronic vascular damage had been induced. These intriguing findings need to be further investigated and serve to add additional support to the importance of the above discussed papers. White Matter Involvement in TBI A consistent clinical finding in patients with TBI is slowing of information processing. Damage to neuronal circuitry, with disruption of long axons, is thought to play a major role in this phenomenon. In an attempt to model this aspect of TBI, a group experimentally studied aspects of TBI damage using a direct impact concussion model in mice (Marion, Radomski et al. 2018) that has previously been shown to induce traumatic axonal injury to the corpus callosum (Mierzwa, Marion et al. 2015). Animals were studied neurophysiologically and morphologically. Following impact, compound action potential velocities along myelinated axons were slowed within 3 days of injury with partial recovery of function by 2 weeks. This suggested to the authors that partial demyelination, followed by remyelination was responsible for the changed action potential velocities. Using electron microscopy, dispersed demyelinated axons and disorganized myelin attachments to axons at paranodes were noted within the corpus callosum of the injured mice. Animals examined after longer periods following TBI exhibited an overall loss of axons at 6 weeks post-injury and observable corpus callosum thinning was seen by 8 weeks. White matter damage is a consistent finding in the brains of patients who survive TBI and have significant cognitive issues and conspicuous thinning of the corpus callosum is often noted in such patients (Johnson, Stewart et al. 2013). This paper provides a useful experimental model for this phenomenon and is promising for a better understanding of the pathophysiology of such white matter damage and a substrate to explore treatment options for patients with this important aspect of head trauma’s clinical effects. The year 2019 has, among other things, witnessed increasing attention to the MeToo movement, recognizing the high prevalence and importance of sexual harassment and violence against women. I was intrigued to find a publication which identified the importance of intimate partner violence as a substrate for TBI, as evidenced by its effects on the integrity of white matter (Valera, Cao et al. 2019). The authors point out that it is estimated that in the United States, about 42,000,000 women over age 15 have experienced physical or sexual abuse and that 75% of women with a history of intimate-partner violence have sustained at least one partner-related TBI, while 50% have sustained repeated TBIs. Despite this staggering number of victims, there has been almost no study of the long-term functional and structural consequences of such violence. The Valera, et al preliminary study attempted to address this gap in knowledge by recruiting 20 women who had sustained such intimate partner assaults, based on a detailed semi-structured interview. Participants underwent detailed study, including 3T MRI neuroimaging. The neuroimaging aspects of the study revealed evidence of abnormalities in fractional anisotropy in the posterior and superior corona radiata as well as the posterior thalamic radiation. However, this was a preliminary study with limited power and lacked a control population for comparison. Nevertheless, this paper identified a potentially very large group of women who are at-risk for significant TBI and has been largely overlooked. Their preliminary results indicate that the degree of neurotrauma in women who sustain TBI through intimate partner violence is sufficient to produce changes in white matter integrity visible with 3T MRI neuroimaging. As the authors point out, the number of women that could be affected vastly overwhelms that of professional contact sport athletes or even those with non-professional participation in such sporting activities. The underlying neuropathologic nature of damage related to this form of neurotrauma remains unstudied and is an issue that clearly needs further investigation. Advances in the Investigation of the Effects of Repeated Impact TBI on the Development of Neurodegeneration (Chronic Traumatic Encephalopathy, CTE) There has been considerable interest in the subsequent development of neurodegeneration following repeated impact TBI, particularly in the form of CTE. In specific, this has involved concerns about how prevalent the disorder is among professional contact sport athletes and, more broadly, about possible risks to the general public following much lesser extents of TBI exposure. In 2019, these concerns have been addressed in a number of ways. Currently, CTE can only be diagnosed by neuropathologic examination of the brain at autopsy. Clinically, there is a considerable need to identify an approach by which patients at-risk for this condition can be evaluated and confidently diagnosed during life. For the most part, this effort has involved the use of a variety of positron emission tomography (PET)-scan ligands directed against tau deposits in the brains of at-risk subjects (Dickstein, Pullman et al. 2016, Marquie, Normandin et al. 2017). The use of similar PET ligands directed at beta-amyloid has been employed with considerable success in the diagnostic work-up of patients thought to be suffering from Alzheimer’s disease and this paper (Stern, Adler et al. 2019) represents the use of similar approaches for CTE, a form of tauopathy. In a 2019 study (Stern, Adler et al. 2019), 26 former National Football League (NFL) players and 31 controls were evaluated using both flortaucipir and florbetapir PET ligands, reagents directed against tau and beta-amyloid, respectively (Wong, Rosenberg et al. 2010, Marquie, Siao Tick Chong et al. 2017) . The former football players had a minimum of 2 years playing in the NFL (mean 9.1 years ± 3.0) and a minimum of 12 years total football playing experience (mean 18.8 years ± 4.6). All participants reported to be suffering from cognitive, mood, and behavioral symptomatology. The controls were free of a history of TBI or evidence of cognitive impairment. The former football player cohort showed significantly elevated uptake by the tau PET ligand in the three neuroanatomic regions that had been examined (bilateral superior frontal, bilateral medial temporal and left parietal areas) when compared to that of the control group. There was no difference between groups in the beta-amyloid directed PET results. As the authors point out, the differences noted were based on collective group findings and the results “do not inform the use of testing in individual patients to determine CTE pathology during life.” At the time of publication, all of the participants in this study are presumably still alive and thus there was no opportunity to validate the findings with post-mortem assessment. This is an important first step but validation using a much large sample will be necessary to determine the specificity and sensitivity of this approach to the diagnosis of at-risk individual patients. Neuropathologists will need to be actively involved in such studies, particularly in attempts to identify individuals with CTE and distinguish them from patients with other forms of neurodegenerative disorders, especially other forms of tauopathies. Most studies to date have depicted CTE in patients who participated in boxing or American professional football. In 2019, an epidemiologic study appeared documenting evidence of an increased incidence of neurodegenerative disorders among individuals who had been former professional soccer players (Mackay, Russell et al. 2019). The authors used mortality data derived from the death certificates of 7,676 former Scottish professional soccer players and compared them to 23,028 controls that were drawn from the general population. Further, they compared prescription information on the use of medications prescribed for the treatment of dementia between the two groups. The results indicated that Scottish professional soccer players had a lower all-cause mortality rate than the general population but showed a significantly increased tendency to die of all forms of neurodegenerative disease. Indeed, significantly higher mortality rates from 1) dementia, not otherwise specified, 2) Alzheimer’s disease, 3) non-Alzheimer’s dementias, 4) motor neuron disease and 5) Parkinson’s disease were all seen in the former soccer players when compared to general population controls. Recognizing the weakness of possible errors in death certificates’ stated causes of death, the authors turned to the prescription data for drugs used to treat dementia, showing a higher rate of use among the former soccer players. Obviously, there was no opportunity to verify by autopsy examination the indicated causes of death on the death certificates. However, errors in ascribing such deaths would be expected to be roughly equal among the athletes and the controls. This study expands the growing epidemiologic literature supporting the concept that repeated head trauma has a correlation with the subsequent development of neurodegenerative diseases and dementia. The nature of that association and, in particular, whether it speaks to the induction of CTE and/or Alzheimer’s disease, Parkinson’s disease or amyotrophic lateral sclerosis, will require additional study and neuropathologic investigation of incident cases. This paper points to the importance of such studies in the future. As an additional point, the authors remind their readers that soccer is played in over 200 countries worldwide with more than a quarter billion participants. While this study could not address the risks of more casual amateur play, it does raise further concerns regarding the long-term consequences of repeated head trauma, a subject that is likely to attract increasing interest and research in the coming years. Attempts to Model Chronic Traumatic Encephalopathy (CTE) in Rodents Chronic traumatic encephalopathy (CTE) is a progressive neurodegenerative disease that has been closely linked to repeated head trauma, primarily in the setting of participation in contact sport athletics. The neuropathologic features of CTE include deposition of abnormally phosphorylated tau in neurons and astrocytes in a unique and distinguishable pattern (McKee, Cairns et al. 2016) (see Figure 2). Despite considerable efforts, no laboratory has been able to produce a consistent and appropriate experimental model of CTE. In 2019, two papers (Gangolli, Benetatos et al. 2019, Mouzon, Bachmeier et al. 2019) described efforts to do so using differing impact rodent models and both failed to induce intraneuronal tau deposits in their injured animals.
Figure 2. Characteristic tau neuropathology features of chronic traumatic encephalopathy (CTE), including: A. depth of sulcus involvement, B,C. perivascular foci with involvement of neurons and astrocytes, and D. neurofibrillary tangles in substantia nigra, pars compacta neurons (arrows). Hyperphosphorylated tau immunohistochemistry (AT-8) in a former collegiate American football player. First and foremost, one needs to recognize that rodent tau is different from human tau and there has been an almost universal failure, under any experimental condition, to induce tau aggregates comparable to human neurofibrillary tangles in wild-type mice. Accordingly, both groups used a humanized mouse transgenic model with knock out of the expression of the native mouse tau, in the hopes that this maneuver would enhance their chances of inducing such changes. In the Gangolli et al. (Gangolli, Benetatos et al. 2019) experiment, head trauma was produce using the Closed-Head Impact Model of Engineered Rotational Acceleration (CHIMERA) approach. CHIMERA is a relatively newly developed technology that is capable of producing both concussive and subconcussive injury to experimental animals and also produces a significant rotational acceleration component (Namjoshi, Cheng et al. 2017). Mice were exposed to 20 daily impacts for 20 consecutive days and the energy used for the CHIMERA impact was controlled to yield animals with either a subconcussive or concussive level of injury. All animals underwent behavioral testing at 3 months and 12 months post-injury and were sacrificed for morphologic and biochemical studies at the later time period. Behavioral abnormalities were seen in both the subconcussive and concussive-exposed animals (more prominent following the higher energy impact model) and this was accompanied by evidence of white matter disruption. Importantly, there was no evidence of tau pathology in any of the injured animals. Clearly, these experiments demonstrated that repeated exposure to head trauma through the CHIMERA approach could induce white matter damage, important in and of itself, but this failed to induce a model that could be used in studying the underlying tau-related pathophysiology of CTE. The Mouzon, et al. paper (Mouzon, Bachmeier et al. 2019) reports exposing humanized transgenic mice to closed-head impact injury with either a single blow or 5 successive blows over a ten day interval (48 hours apart). The animals were then allowed to survive for either 24 hours or 12 months, post-injury. Evaluations included behavioral testing and, on sacrifice, morphologic and biochemical assays. The behavioral testing showed persistent and progressively worsening deficits in visuospatial learning from 2 to 12 months and significant deficits in visuospatial memory consolidation at 12 months post-injury. Neuropathologic evaluation at both 24 hours and 12 months revealed evidence of axonal injury, thinning of the corpus callosum and activation of microglia and astrogliosis in the white matter. Tau immunohistochemistry and ELISA studies showed an increase in phosphorylated tau in the cortex at the site below the impact point and in the CA1/CA3 region of the hippocampus of both the single and repeated injury mice. However, this response was transitory in the immediate post-injury (24 hours) phase and was not detected at the 12-month survival time period. No neuronal tau aggregates were detected in the injured animals. The authors point out that the “post-TBI neuropathology in hTau and WT mice was otherwise comparable, with essentially similar levels of axonal injury and chronic neuroinflammation in both study groups.” They further suggested that the observation of transient tau hyperphosphorylation at acute time periods post-injury “may be a normal physiologic response of the brain to mTBI.” Both articles failed to show that the use of humanized tau mice with repeated impact TBI was able to develop a rodent model of CTE and thus their results could not be used to mimic the human disease. In my opinion, despite considerable effort, the neurotrauma field has yet to identify a consistent and valid animal model of CTE. Characterization of Tau Filaments in Chronic Traumatic Encephalopathy Cases by Cryo-Electron Microscopy Cryo-electron microscopy is a technology that is capable of imaging the three-dimensional structure of complex biomolecules at the single digit Angstrom level of resolution. This newly developed approach is so powerful, that its developers, Drs. Jacques Dubochet, Joachim Frank and Richard Henderson, were honored with the 2017 Nobel Prize in Chemistry for their work. Tau filaments isolated from the brains of patients with Alzheimer’s disease (Fitzpatrick, Falcon et al. 2017) and Pick’s disease (Falcon, Zhang et al. 2018) have been reported using this technique and have been shown to form differing configurations. In 2019, Falcon, et al. (Falcon, Zivanov et al. 2019) reported a cryo-EM study of tau filaments isolated from three cases of CTE (a former American football player and two former boxers). The configuration of the filaments isolated from each of the CTE cases were identical and were distinctly different than that isolated from the Alzheimer’s disease and Pick’s disease brains. In the CTE-derived tau filaments, the β-helix region of the molecule displayed a distinct hydrophobic cavity that was not seen in tau filaments from Alzheimer’s or Pick’s disease specimens. This cavity contained an additional density whose identify has yet to be identified but was thought to be a non-proteinaceous co-factor. These exciting findings serve to define CTE as representing a distinct and different neurodegenerative process from Alzheimer’s disease. In addition, the identity and function of the associated co-factor represents a potentially exciting therapeutic target for patients with CTE. Conclusions In this review a number of studies are presented, some involving clinically relevant issues while others use preclinical models to investigate pathophysiologic mechanisms related to neurotrauma. The studies discussed here have relevance to neuropathologists with an interest in aspects of neurotrauma, whether they be involved in clinical diagnostic issues or preclinical models. Despite the clinical importance of neurotrauma and its acute and long-term consequences, there exist major knowledge gaps throughout the field that require further investigation. I hope the studies discussed here will help to stimulate neuropathologists, especially those newly entering the field, to become active in this important and fertile area of investigation. Disclosure Statement The opinions expressed herein are those of the author and are not necessarily representative of those of the Uniformed Services University of the Health Sciences, the United States Department of Defense or of the United States Army, Navy or Air Force. References Chiara Ricciardi, M., R. P. Bokkers, J. A. Butman, D. A. Hammoud, D. L. Pham, S. Warach and L. L. Latour (2017). "Trauma-Specific Brain Abnormalities in Suspected Mild Traumatic Brain Injury Patients Identified in the First 48 Hours after Injury: A Blinded Magnetic Resonance Imaging Comparative Study Including Suspected Acute Minor Stroke Patients." J Neurotrauma 34(1): 23-30. CRASH, collaborators (2019). "Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3): a randomised, placebo-controlled trial." Lancet 394(10210): 1713-1723. Dickstein, D. L., M. Y. Pullman, C. Fernandez, J. A. Short, L. Kostakoglu, K. Knesaurek, L. Soleimani, B. D. Jordan, W. A. Gordon, K. Dams-O'Connor, B. N. Delman, E. Wong, C. Y. Tang, S. T. DeKosky, J. R. Stone, R. C. Cantu, M. Sano, P. R. Hof and S. Gandy (2016). "Cerebral [(18) F]T807/AV1451 retention pattern in clinically probable CTE resembles pathognomonic distribution of CTE tauopathy." Transl Psychiatry 6(9): e900. Falcon, B., W. Zhang, A. G. Murzin, G. Murshudov, H. J. Garringer, R. Vidal, R. A. Crowther, B. Ghetti, S. H. W. Scheres and M. Goedert (2018). "Structures of filaments from Pick's disease reveal a novel tau protein fold." Nature 561(7721): 137-140. Falcon, B., J. Zivanov, W. Zhang, A. G. Murzin, H. J. Garringer, R. Vidal, R. A. Crowther, K. L. Newell, B. Ghetti, M. Goedert and S. H. W. Scheres (2019). "Novel tau filament fold in chronic traumatic encephalopathy encloses hydrophobic molecules." Nature 568(7752): 420-423. Fitzpatrick, A. W. P., B. Falcon, S. He, A. G. Murzin, G. Murshudov, H. J. Garringer, R. A. Crowther, B. Ghetti, M. Goedert and S. H. W. Scheres (2017). "Cryo-EM structures of tau filaments from Alzheimer's disease." Nature 547(7662): 185-190. Gama Sosa, M. A., R. De Gasperi, G. S. Perez Garcia, G. M. Perez, C. Searcy, D. Vargas, A. Spencer, P. L. Janssen, A. E. Tschiffely, R. M. McCarron, B. Ache, R. Manoharan, W. G. Janssen, S. J. Tappan, R. W. Hanson, S. Gandy, P. R. Hof, S. T. Ahlers and G. A. Elder (2019). "Low-level blast exposure disrupts gliovascular and neurovascular connections and induces a chronic vascular pathology in rat brain." Acta Neuropathol Commun 7(1): 6. Gangolli, M., J. Benetatos, T. J. Esparza, E. M. Fountain, S. Seneviratne and D. L. Brody (2019). "Repetitive Concussive and Subconcussive Injury in a Human Tau Mouse Model Results in Chronic Cognitive Dysfunction and Disruption of White Matter Tracts, But Not Tau Pathology." J Neurotrauma 36(5): 735-755. Griffin, A. D., L. C. Turtzo, G. Y. Parikh, A. Tolpygo, Z. Lodato, A. D. Moses, G. Nair, D. P. Perl, N. A. Edwards, B. J. Dardzinski, R. C. Armstrong, A. Ray-Chaudhury, P. P. Mitra and L. L. Latour (2019). "Traumatic microbleeds suggest vascular injury and predict disability in traumatic brain injury." Brain 142(11): 3550-3564. Huang, Y. L., Y. S. Kuo, Y. C. Tseng, D. Y. Chen, W. T. Chiu and C. J. Chen (2015). "Susceptibility-weighted MRI in mild traumatic brain injury." Neurology 84(6): 580-585. Johnson, V. E., J. E. Stewart, F. D. Begbie, J. Q. Trojanowski, D. H. Smith and W. Stewart (2013). "Inflammation and white matter degeneration persist for years after a single traumatic brain injury." Brain 136(Pt 1): 28-42. Mackay, D. F., E. R. Russell, K. Stewart, J. A. MacLean, J. P. Pell and W. Stewart (2019). "Neurodegenerative Disease Mortality among Former Professional Soccer Players." N Engl J Med 381(19): 1801-1808. Marion, C. M., K. L. Radomski, N. P. Cramer, Z. Galdzicki and R. C. Armstrong (2018). "Experimental Traumatic Brain Injury Identifies Distinct Early and Late Phase Axonal Conduction Deficits of White Matter Pathophysiology, and Reveals Intervening Recovery." J Neurosci 38(41): 8723-8736. Marquie, M., M. D. Normandin, A. C. Meltzer, M. Siao Tick Chong, N. V. Andrea, A. Anton-Fernandez, W. E. Klunk, C. A. Mathis, M. D. Ikonomovic, M. Debnath, E. A. Bien, C. R. Vanderburg, I. Costantino, S. Makaretz, S. L. DeVos, D. H. Oakley, S. N. Gomperts, J. H. Growdon, K. Domoto-Reilly, D. Lucente, B. C. Dickerson, M. P. Frosch, B. T. Hyman, K. A. Johnson and T. Gomez-Isla (2017). "Pathological correlations of [F-18]-AV-1451 imaging in non-alzheimer tauopathies." Ann Neurol 81(1): 117-128. Marquie, M., M. Siao Tick Chong, A. Anton-Fernandez, E. E. Verwer, N. Saez-Calveras, A. C. Meltzer, P. Ramanan, A. C. Amaral, J. Gonzalez, M. D. Normandin, M. P. Frosch and T. Gomez-Isla (2017). "[F-18]-AV-1451 binding correlates with postmortem neurofibrillary tangle Braak staging." Acta Neuropathol 134(4): 619-628. McKee, A. C., N. J. Cairns, D. W. Dickson, R. D. Folkerth, C. D. Keene, I. Litvan, D. P. Perl, T. D. Stein, J. P. Vonsattel, W. Stewart, Y. Tripodis, J. F. Crary, K. F. Bieniek, K. Dams-O'Connor, V. E. Alvarez, W. A. Gordon and T. C. group (2016). "The first NINDS/NIBIB consensus meeting to define neuropathological criteria for the diagnosis of chronic traumatic encephalopathy." Acta Neuropathol 131(1): 75-86. Mierzwa, A. J., C. M. Marion, G. M. Sullivan, D. P. McDaniel and R. C. Armstrong (2015). "Components of myelin damage and repair in the progression of white matter pathology after mild traumatic brain injury." J Neuropathol Exp Neurol 74(3): 218-232. Mouzon, B., C. Bachmeier, J. Ojo, C. Acker, S. Ferguson, G. Crynen, P. Davies, M. Mullan, W. Stewart and F. Crawford (2019). "Chronic White Matter Degeneration, but No Tau Pathology at One-Year Post-Repetitive Mild Traumatic Brain Injury in a Tau Transgenic Model." J Neurotrauma 36(4): 576-588. Namjoshi, D. R., W. H. Cheng, A. Bashir, A. Wilkinson, S. Stukas, K. M. Martens, T. Whyte, Z. A. Abebe, K. A. McInnes, P. A. Cripton and C. L. Wellington (2017). "Defining the biomechanical and biological threshold of murine mild traumatic brain injury using CHIMERA (Closed Head Impact Model of Engineered Rotational Acceleration)." Exp Neurol 292: 80-91. Roberts, I., A. Belli, A. Brenner, R. Chaudhri, B. Fawole, T. Harris, R. Jooma, A. Mahmood, T. Shokunbi, H. Shakur and C.-t. collaborators (2018). "Tranexamic acid for significant traumatic brain injury (The CRASH-3 trial): Statistical analysis plan for an international, randomised, double-blind, placebo-controlled trial." Wellcome Open Res 3: 86. Stern, R. A., C. H. Adler, K. Chen, M. Navitsky, J. Luo, D. W. Dodick, M. L. Alosco, Y. Tripodis, D. D. Goradia, B. Martin, D. Mastroeni, N. G. Fritts, J. Jarnagin, M. D. Devous, Sr., M. A. Mintun, M. J. Pontecorvo, M. E. Shenton and E. M. Reiman (2019). "Tau Positron-Emission Tomography in Former National Football League Players." N Engl J Med 380(18): 1716-1725. Valera, E. M., A. Cao, O. Pasternak, M. E. Shenton, M. Kubicki, N. Makris and N. Adra (2019). "White Matter Correlates of Mild Traumatic Brain Injuries in Women Subjected to Intimate-Partner Violence: A Preliminary Study." J Neurotrauma 36(5): 661-668. Wong, D. F., P. B. Rosenberg, Y. Zhou, A. Kumar, V. Raymont, H. T. Ravert, R. F. Dannals, A. Nandi, J. R. Brasic, W. Ye, J. Hilton, C. Lyketsos, H. F. Kung, A. D. Joshi, D. M. Skovronsky and M. J. Pontecorvo (2010). "In vivo imaging of amyloid deposition in Alzheimer disease using the radioligand 18F-AV-45 (florbetapir [corrected] F 18)." J Nucl Med 51(6): 913-920. Zhang, J., M. He, Y. Song and J. Xu (2018). "Prognostic role of D-dimer level upon admission in patients with traumatic brain injury." Medicine (Baltimore) 97(31): e11774
Copyright: © 2020 The author(s). This is an open access article distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited, a link to the Creative Commons license is provided, and any changes are indicated. The Creative Commons Public Domain Dedication waiver (https://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. |