VOL. 2, No. 1
AbstractCardiovascular diseases are an emerging cause of morbidity and mortality in India. India produces less than 150 cardiologists annually, leading to a gap between the need and availability of trained professionals. A three-year cardiology-training programme is available for post-graduate doctors in the conventional medical education system. The majority of the people living in rural areas, small towns, and district towns in the country do not have any access to cardiac care, because trained cardiologists are mostly concentrated in the metropolitan are or capital cities. To address this issue Indira Gandhi National Open University has designed and developed a two-year, full-time training programme in the area of non-invasive cardiology for medical graduates, named the Post Graduate Diploma in Clinical Cardiology, which is being offered through the open and distance learning mode. The objective of the programme is to train a large number of medical graduates effectively to enable early recognition, management and prevention of common cardiovascular diseases. Learners have been given the opportunity to train in different departments and are posted in various areas in this programme, such as management of common cardiovascular diseases (6 months), ECG and Stress Testing (3 months), Echocardiography (3 months), ICU/CCU management (6 months), Paediatrics Cardiology (3 months), preventive cardiology (3 months). Self-learning materials, 33 video programmes (1260 minutes), and a monthly, live, interactive teleconference (90 minutes), have been incorporated into this programme. Beside these, 50 theory counselling sessions, 25 guest lectures, seminars, journal clubs and case discussions have been provided in every training center. Hands-on skills training is provided to every learner as prescribed in this programme. The 72 credits in the programme are divided into seven theory and six practical courses. Students need to pass in each course independently both in the internal examination and the term end examination. The minimum teacher-student ratio has been maintained strictly in both training and term end practical examinations. The topmost cardiac institutes/hospitals across the country have been identified as training centers, as per the norms of the university. This programme began with 116 students in 16 training centers in 2006. In 2013, 443 students were enrolled in 67 training centres. More than 320 cardiologists are involved as academic counselors in this training programme. A total of 1006 candidates have successfully completed their training and many of them are providing services in small or district towns of the country.
Cardiovascular diseases are the most important causes of morbidity and mortality in developed countries. But in developing countries such as India, in addition to the infectious diseases, non-communicable diseases (NCDs) like cardiovascular diseases have also emerged as significant causes of morbidity and mortality.
The increased prevalence of cardiovascular diseases the world over, and particularly in India, is because of changing life styles and increased life expectancy, attributed to improved healthcare systems. Cardiovascular diseases, namely ischaemic heart disease, cerebrovascular disease, rheumatic heart disease (RHD) etc., are responsible for 27 percent of all deaths in the South-East Asia Region.
In a review conducted in 1996 (published in the Annual Report 2006 – 2007, Ministry of Health and Family Welfare, Government of India), it was reported that the prevalence of coronary heart disease (CHD) had increased from 1 percent in 1960 to 9.6 percent in 1995 among urban Indians. Similarly, the prevalence among the rural residents of India rose from 2 percent in 1974 to 3.7 percent in 1995. The prevalence of CHD is now (2006-2007) reported to be 3 – 4 percent in rural areas and 8 – 10 percent in urban areas, among adults. Based on this official data, it is estimated that there were approximately 29.8 million patients with CHD in the year 2003. With an estimated 10 percent attrition and event rate, the Annual Report projected an annual new event or death of 2.9 million persons per year with nearly 1.5 million people dying due to CHD every year. Cardiovascular diseases contributed to 25 percent of deaths among the adult population in 2005.3
The present health infrastructure of India produces less than 150 DM/ DNB cardiologists annually to take care of the burden of the disease. 4 In the conventional education system of the medical stream, DM/DNB in cardiology is a 3 – year, full-time, residential, super-specialist training programme. A Medical School Graduate (an MBBS) needs to complete a 3 - year post graduation in General Medicine/Pediatrics after completion of the five and half years graduation training programme (MBBS) to be eligible for Cardiology training, i.e., a DM/DNB in cardiology.
Most Doctors trained in cardiology were located in metropolitan areas or big cities, as infrastructure, financial resources and clinical practice are easily available, as opposed to a rural or small/district town set up. Hence, trained cardiologists are mostly concentrated in the tertiary setups located in metropolitan areas or big cities, leading to a gap between the need and availability of trained cardiologists. But health or cardiovascular diseases do not distinguish either between rural and urban populations, or the rich and the poor. The National Health Profile 2005 (National Health Profile 2005, pp. 8 & 28) reported that, in India, approximately 26 percent of population live below the poverty line and more than 72 percent live in rural areas.5 Post-graduate doctors in medicine (MD) attend to cardiovascular cases in small/district towns and rural areas, without the appropriate training in cardiology, since a Post Graduate Doctor in Medicine undergoes training in the department of cardiology for only 4-6 months in his or her 3 year-training period.
Keeping the prevalent medical scenario in mind, this paper seeks to critique the two-year training programme conceptualised, designed and developed by the School of Health Sciences, Indira Gandhi National Open University New Delhi, India. This programme is offered through the open and distance learning system in an effort to bridge the gap between the community at large and trained cardiologists. It needs to be re-iterated that this programme was planned with a certain vision in mind, that of providing good cardiac care to all, and in keeping with this vision, the programme was designed and extra advantage was given to medical doctors serving in non metropolitan areas, with the hope that even if only 20 percent of the trained cardiologists serve the district level town then the community at large will benefit from their expertise.
Methodology
To meet the objective outlined earlier, the School of Health Sciences (SOHS), Indira Gandhi National Open University (IGNOU) launched a two-year training programme in non-invasive cardiology for MBBS Graduates in June 2006. The programme being discussed is the Post Graduate Diploma in Clinical Cardiology (PGDCC). It is a 72 - credit programme consisting of seven theory and six practical courses, with 58 percent credit dedicated to the practical component. One credit in the IGNOU system of teaching/ learning methodology is equivalent to 30 hours of study. However, in the PGDCC programme, 1 credit/ 30 hours of study translates into 30 hours of supervised training and does not include the time that one may take to study at home or to write his/her assignments. It means students are receiving approximately 3 hours (2160 hours / 730 days) supervised, hands-on skilled training or theory counselling every day. This programme also prescribes the minimum number of practice cases needed under supervision, e.g., echocardiography, 100 cases; bed-side pediatric, 20 cases, etc. Leaners need to maintain a log book of their day-to-day practical activity, which is assessed by academic counselors periodically and at the time of the term end practical examination.
Table 1: Posting Schedule of the PGDCC Programme
Area of Training |
Duration of Training |
First Year |
|
Wards + OPD (MCCL* 003) |
3 Months |
ECG/Stress Testing (MCCL 001) |
3 months |
Echocardiography (MCCL 002) |
3 months |
ICU/CCU (MCCL 006) |
3 months |
Second Year |
|
Special Observation (MCCL 006) |
1 month |
ICU/CCU (MCCL 006) |
2 months |
Ward+ OPD (MCCL 003) |
3 months |
Paediatric Cardiology (MCCL 004) |
3 months |
Preventing Cardiology (MCCL 005) |
3 months |
*MCCL is a Practical training course code. Candidates need to complete the 24 months training programme within a maximum 48 months, i.e., 4 years.
The selection process of the candidates was through an entrance examination followed by centralized counselling. Induction meetings were organized on the same date after the centralized counseling for allotment of PSC. In this meeting students were informed about the aim and objectives of the training, training package, assessment methods, rule and regulation of the university, etc. The total number of seats in each Programme Study Centre (PSC) is limited to a maximum of 10. This Programme began with 16 PSCs activated in 2006 and, due to the great demand for more seats, the number of PSCs was increased to 67 in 2013. The programme fee is Rs. 100,000/ (Indian Rupees or approximate US$ 1667/, if US$ 1 = Rs. 60/- Indian Rupees). Only Cardiac Hospital Institutions conducting a DM or DNB Cardiology programme are eligible to be training centres for the PGDCC programme. These training centres are called Programme Study Centres (PSCs) in our terminology.
The academic counsellors who counsel the students are fully fledged, trained cardiologists (DM/DNB Cardiology) already working in PSCs. Training packages of this programme consist of self learning materials (SLMs), theory and practical classes/academic counselling at PSC, case discussion, monthly live interactive teleconferences, interactive radio counseling and the broadcast of video programmes. A total of 37 units/chapters in 13 Blocks/Booklets were provided as self-learning materials, along with six practical log books to each of the students. Special hands on training is imparted on electrocardiography (ECG), stress testing, echocardiography, out-patient department (OPD) and ward management of cardiovascular diseases, pediatric cardiology, intensive coronary care, cardiac emergencies and community posting. All training is imparted in reputed cardiac hospitals across the country.
A minimum of 50 theory counseling sessions of academic counselling must be conducted within two years of the training period. Each learner must present eight seminars, eight journal clubs and nine case discussions. PSC must arrange 25 guest lectures of the learners to understand different areas associated with non-invasive cardiology. The 25 guest lectures were further divided into six on Diabetes mellitus, five in Pulmonology, four in Radiology, four in Cardiac Surgery, four in Anesthesiology and two in nephrology. Live interactive teleconferences, which are one-way video and two-way audio, have been conducted for 90 minutes every month. These live teleconference sessions are also webcast, besides being broadcast through Gyandarshan Channel 2. Students from across the country participated and lots of interaction took place during the live teleconference sessions. Short Message Service (SMS) service is utilized to inform the schedule and topic of teleconference sessions, dates of examination, results and other support services. A total of 33 video programmes (1260 minutes) has made available to all learners. It is mandatory for students to maintain a minimum of 85 percent attendance in both the theory and practical components independently.
The evaluation strategy of this programme consists of continuous as well as Term End Evaluation for both theory and practical courses. Continuous Evaluation has a 50 percent weightage and is conducted at the PSC at intervals of three to four months. The first-year theory term end examination is to be attempted only after completing a full academic year of training. The second-year term end theory examination is to be attempted at the end of the two-year training period. The Term End Practical Exam is conducted after the completion of the two-year training period. A one-day, term-end practical examination is conducted in a PSC, depending upon the number of the learners, in the presence of internal and external practical examiners. The number of examiners depends on the number of learners who appear in the practical examination (ratio 1:3). The marking scheme of the term end practical examination is standardized and followed for assessment of each learner.
Quality Assurance
A monthly/quarterly/annual academic training calendar for both the theory as well as the practical component, prepared by the respective PSC is sent to the Regional Centre and Programme Coordinator in the headquarters at IGNOU. Meetings are also arranged with the Programme in-charges (PICs) at a national level annually in order to monitor the quality of training and improve upon the programme every year. The mailing addresses, phone numbers and e-mail addresses of the Programme Coordinator, Regional Director, Programme In-charges (PICs) and other support divisions are distributed to all leaners, PICs and Academic Counsellors. The Programme Coordinator also receives continuous feedback and suggestions from students, PICs, and Regional Directors through various media. The Advisory Board of the PGDCC programme also provides support in monitoring activity.
Table 2: Total number of Programme Study Centre, academic counselors, students enrolled and passed out in the PGDCC programme
Year |
Number of the Programme Study Centre |
No of the Academic Counsellors |
Number of the students Enrolled |
Number of the candidates successfully completed this programme [Year of Convocation]* |
2006 |
16 |
102 |
116 |
---- |
2007 |
22 |
150 |
133 |
---- |
2008 |
35 |
206 |
253 |
88 |
2009 |
44 |
261 |
262 |
101 |
2010 |
56 |
278 |
297 |
194 |
2011 |
66 |
320 |
348 |
210 |
2012 |
66 |
320 |
209 |
180 |
2013 |
67 |
325 |
443 |
233 |
Total |
67 |
325 |
2061 |
1006 |
*There is a lag of 2-4 years in certification, since a valid registration period is 2-4 years; e.g., students enrolled in 2006 would complete their programme in 2008. Students of the 2012 and 2013 batch are still in the training.
It needs to be highlighted that this PGDCC two-year Programme is a highly intensive programme that entails a student – teacher ratio of approximately 2:1. The strength of this programme is that doctors are trained for two years on a full-time basis in non-invasive cardiology, in which all hands-on skill training is guided by trained and experienced cardiologists. Training is implemented only in cardiac institutes already conducting a DM/DNB cardiology-training programme. Orientation training programmes of academic counselors of the training institution have been conducted before students enrolled in the training centre. Learners are benefited by not only an ODL system but also the support of the conventional education system. Since students are directly attached to a cardiac institution on a full-time basis, academic counsellors are available round the clock for expert guidance in theory as well as the practical components of training in cardiology. Students are also getting the benefit of all the support of the university, such as self-learning materials, multimedia packages, live interactive teleconferences, etc. However, the one major weakness of the Programme, as visualised by us, is the non-recognition by the Medical Council of India.
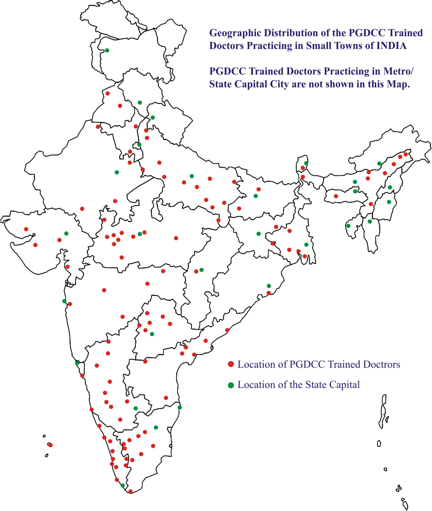
Figure 1: Geographical distribution of PGDCC trained doctors practicing in small towns in India
Conclusion
An academic degree of a Diploma in Clinical Cardiology is viable after a medical graduation degree/MBBS. This programme has in a sense brought to light the fact that quality training, even in a traditionally non-open and distance learning area such as in cardiac care, is not only possible but also highly desirable through the Open and Distance Learning System in convergence with the partnership of reputed cardiac institutes in the country. It needs to be highlighted that such a programme is also not available in the conventional medical education system and is a first for both medical education as well as the ODL. Not only this but the PGDCC programme is also the first and only full-time medical education programme for medical graduates (MBBS) in the world to be imparted through the ODL system.
Already 1006 candidates have successfully completed their training to date. As per informal feedback from PGDCC candidates who have graduated, many of them were successfully practicing in the non-invasive area in district towns (as shown in Figure No 1). The vision also included a bridge to be built between the communities (particularly the rural and non-metropolitan community) and cardiologists through the ODL System, and a fond hope that the medical professional/ personnel would also be able to fulfill some of their social responsibilities.
Recommendation
This is an innovative programme that is still evolving. The programme team is working constantly towards enriching the training package in order to produce quality doctors trained in cardiac care for the community. The Advisory Board of the programme recommended revision of the curriculum of the programme along with the building of an online platform with the learning management system.
Acknowledgement: Post Graduate Diploma in Clinical Cardiology programme team.
Biplab Jamatia is an Assistant Professor, School of Health Sciences, Indira Gandhi National Open University, Maidan Garhi, New Delhi, India. E-mail: biplabjamatia@gmail.com